Von G. Samedi, MD, PhD, is a cytopathologist at the
University of Colorado in Denver, CO. I had the pleasure of meeting Dr. Samedi
as a result of the thoughtful introduction facilitated by Dr. Melissa Upton,
who thought we should talk given our shared interest in global pathology.
I learned that Dr. Samedi is originally from Haiti and
completed his MD, PhD, and pathology training in the US. He has always been
interested in global health as part of his personal and professional passion
and has spent the last decade dedicating his expertise to improving pathology
services in low resource settings. It was readily apparent to me that Dr.
Samedi’s approach to the world’s healthcare issues is based in the fact that he
views these as shared problems – ones that he can and does help solve. This
mindset is reflected in the way he lives his life – admirably contributing to
society in any way that he possibly can. I was eager to hear of the
opportunities he’s found in order to contribute, so that I might learn and
share with all of you the ways that we can all get involved. Read on to
discover the inspiring story of someone who has persisted in finding ways to
give to the world through service!
Q: When did you first get started working in global
health through pathology?
A: I started working with ASCP when I was a 4th
year pathology resident in 2010 when they called me to assist their project in
Haiti, which was in response to the tremendous damage caused from the
earthquake. I had signed up as a potential volunteer on their website prior to
this and they reached out to me seeing that I had language proficiency in both
French and Creole. I spent 21 days working with them and my residency program
allowed me to count this time as an outside elective. Their main goal was to work
with the Haiti’s national public health laboratory (Laboratoire National de
Santé Publique) and its various national and international partners to set up
and run a laboratory in this acute disaster situation, and the hands-on
experience I gained in doing this was well worth my program elective time.
After this, ASCP requested that I continue to volunteer with
them and since then, I have been working on pathology and laboratory medicine
improvement projects at their partner sites all over the world.
Q: Can you tell me about your experiences volunteering
with ASCP’s global health initiatives?
A: Working with ASCP at their global partner sites
has allowed me to volunteer in a variety of ways which is unique to the needs
of each situation. Every trip has been different. In Botswana, I helped process
and read the cervical biopsy specimens that had accumulated as a result of a
government program to address the high incidence of cervical cancer. The biopsy
program was successful except that there weren’t enough pathologists to give
results from the tissue samples – so the government reached out to ASCP to help
fill the gap in care. In Ukraine, I worked with laboratorians and clinicians in
which I helped conduct a workshop on HIV related testing services. In the Ivory
Coast, I worked as a part of a mentorship program to assist a newly formed
pathology organization gain functional independence. In Rwanda, the project was
focused on bringing telepathology services into the laboratory. In Kenya, I
worked with ASCP to offer support to the local pathology association. I’ve also
returned to Haiti since 2010 and now we’ve shifted away from disaster
management and focused on local laboratorian training with the goal of
achieving sustainability.
Q: Why do you volunteer to improve global pathology
services?
A: Historically, pathology and global health are not
thought of as connected, yet without pathology, there is no practice of modern
medicine. It is the same anywhere in the world as it is in the US, you must
have a functioning pathology laboratory in order to effectively deliver health
care. Once you understand this, you understand the need that exists in low- and
middle-income countries where there is ample opportunity to serve and give
back. Doing so gives me a sense of purpose and it is not just a one-way relationship,
as I also benefit from interacting with my global colleagues and learning from
them. What I have seen my colleagues do with so few resources is impressive and
inspiring.
Q: How do you fit volunteering into your schedule?
A: My volunteering experiences have ranged anywhere
between 3 to 21 days. I prioritize this work and have been fortunate to work
for departments that support it, often allowing me to use professional time and
vacation time to work on these projects.
Q: What advice would you give someone new to engaging in
global health?
A: The key is to focus on building relationships for
the long term. Be patient, flexible, and realize that what you want to
accomplish may not happen in the first or even the second visit. Sometimes
things just don’t go as planned and you have to keep working and go with the
flow. If anyone in laboratory medicine is looking for volunteering opportunities,
reach out to ASCP and volunteer to get involved – you can travel to their
partner sites, volunteer to read cases through their telepathology program, or
serve on ASCP’s global health committees. There’s a way for everyone and anyone
working in laboratory medicine to get involved, no matter what your specialty
and capacity to serve is.
-Dana Razzano, MD is a former Chief Resident in her fourth year
in anatomic and clinical pathology at New York Medical College at
Westchester Medical Center and will be starting her fellowship in
Cytopathology at Yale University in 2020. She is passionate about global
health and bringing pathology and laboratory medicine services to low
and middle income countries. She was a top 5 honoree in ASCP’s Forty
Under 40 in 2018 and was named to The Pathologist’s Power List of 2018
and 2019. Follow Dr. Razzano on twitter @Dr_DR_Cells.
Good morning!
We’re entering the holiday season, and it’s an exciting time for all. I love
seeing the ethnic and cultural diversity as we all celebrate our favorite
holidays with family and friends. I myself look forward to the holiday season.
It’s a festive time and a season of giving and sharing. It’s a favorite time of
year to share traditions and create new ones. However, at a time when stores
have Christmas candy on the shelves, holiday lights up and holiday music playing
on the day after Halloween, I feel a bit rushed and want to slow down and find
better ways to celebrate and enjoy the season. Over the past few years I have
been making a special effort to become more environmentally conscious;
remembering my reusable bags at stores, purchasing more reusable products, and
reusing, recycling, and upcycling whenever I can. I belong to a community ‘buy
nothing’ group and am warmed by the generosity of strangers to others in the
community. It’s wonderful to give from our abundance and to receive wish list
items from neighbors without having to exchange money. And it’s great for the
environment, too. Used items are being put to use by others, and not into
landfills. People in the community have asked for or gifted furniture,
clothing, tools, toys and many other goods and services. I have gifted no
longer needed clothing, household items, excess fabric from my fabric stash,
and donated my time to participate in a career fair at a local high school. I
have been given a car set for my grandchildren when they visit, toys, and
someone even loaned me a bike trailer so we could take my granddaughter out for
a bike ride. The generosity makes it feel like the holiday season all year
round.
So, you may be
asking, “where is this blog going?” I saw a memo from Red Cross this week that
there is a critical need for blood and platelets and thought that giving to our
community with the gift of blood would be a wonderful way to make this holiday
season even better! It’s one of the most generous gifts we can give, and costs
nothing. Every 2 seconds in the US, someone needs a blood product. That’s about
36,000 units of red blood cells, 7,000 units of platelets and 10,000 units of
plasma needed every day. 21 million blood products are transfused every year.1
That’s a lot of blood. And, these blood
products cannot be manufactured, so must come from volunteer donors.
In
the US, we need to collect about 13,000 units a day to meet demand. Approximately
14 million units of whole blood are collected each year from roughly
7 million donors.1 The blood is processed into components and
used in the treatment of surgical, obstetric, oncology, and other patients. One
unit of whole blood can be made into up to 3 components and used to help up to
3 patients. Yet, even with all these donations we still cannot keep up with
demand. Weather, holidays, illness and travel can all affect blood donations. Shortages
are not just apparent during the winter holiday season. This past summer, the
Red Cross announced a critical blood shortage around the July 4th
holiday. Compared to other weeks, there were 17,000 fewer blood donations
during the week of July 4th. As of July 9, the Red Cross had less than a
three-day supply of most blood types and less than a two-day supply of Type O
blood. 2 During the summer, and particularly during the holiday
week, people are busy with other activities or traveling. In the winter, busy
schedules, holiday travel, winter weather and seasonal illnesses contribute to
fewer blood and platelet donations. Severe weather can also cause the
cancellation of blood drives which greatly impact the blood supply.
Some people donate blood because they see this critical need
and hear the calls for blood. Others donate because a classmate or friend asked
them to. Some people feel it’s their civic duty. For some, it just makes them
feel good to help another person. And, others donate for the cookies and tee
shirt. Yet, for all donors, it is a form of volunteerism and giving to the
community. But, did you know that, other than the benefits from helping others,
there are benefits to the donor, as well? Helping others can improve our
emotional and physical health. It can help reduce stress, improve emotional well-being
and help people feel a sense of belonging. A study conducted in Sweden
concluded that regular blood donors enjoy better than average health.Blood
donors had an overall mortality 30% lower and a cancer incidence 4% lower than
the control population.3 Donating blood may help reduce high iron
stores, a risk factor for heart attack. In addition, there have been several
studies over the past few years, exploring the hypothesis that regular blood
donations may help in the management of hypertension and high cholesterol.
Another
interesting benefit of blood donation is being able to contribute to science
and research. For example, there is currently a study being conducted on donor
blood to test an investigational nucleic acid test for Babesia microti. Babesia
microti is responsible for most transfusion-transmitted babesiosis cases in the
United States, but there is no licensed test for screening for B. microti in
donated blood. Participation in this study can help obtain FDA approval for a
screening test. By giving
your consent to use your blood sample, there is no additional blood taken and
no further time commitment, but you can help protect the public health by
supporting the development of a new blood safety test.
How
can we, as individuals, help? About 38% of the population is eligible to donate
blood, but less than 10% of the population actually donates. To be eligible to
donate, you should be in good general health and feeling well. You
must be at least 17 years old in most states
(16 years old with parental
consent in some states) but there is no age limit to donation. Adult doors must
weigh 110 lbs, but there are additional height and weight requirements for
donors 18 years old and
younger. There have also been some recent changes to blood donor requirements. I
will not be able list all of them here, but some of them don’t change a
deferral, only the reasoning behind the deferral. One of the most prominent
changes is, as of 2016, the indefinite deferral for men who have had sex with
men, has been changed to a 12 month deferral since the last sexual contact with
another man . Also changed is the minimum hemoglobin for male donors. This has been
raised from 12.5g/dl to 13.0 g/dl. Until this time, the cutoff was the same for
both males and females. Males with a Hgb below 13.0 g/dl are considered anemic
and are no longer eligible to donate blood. On the other hand, the criteria for
females to be mildly anemic is a Hgb below 12.0 g/dl, so females between 12.0
g/dl and 12.5 g/dl, though not considered anemic, are still not eligible to
donate. The minimum hemoglobin for females has not changed and remains 12.5
g/dl. To review other eligibility requirements, visit https://www.redcrossblood.org/donate-blood/how-to-donate/common-concerns/first-time-donors.html
So, in this busy season, we often find ourselves with little time to get our own “to do” lists done, yet alone volunteer our time for others. But most of us would welcome an hour to reduce stress and improve our emotional well-being. Please consider a gift of self this season. It takes about an hour of your time, you get to sit and relax with your feet up, to feel good about yourself, and you’ll even get a snack!
Edgre, G et al. Improving health profile of blood donors as a
consequence of transfusion safety efforts. Transfusion. 2007 Nov;47(11):2017-24.
Kamhieh-Milz
S, et al.Regular blood donation may help in the
management of hypertension: an observational study on 292 blood donors. Transfusion. 2016 Mar;56(3):637-44. doi: 10.1111/trf.13428.
Epub 2015 Dec 8.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
Vitamin D is one of the most commonly ordered laboratory
tests in the primary care setting, as well as one of the most widely used forms
of dietary supplementation today. While the rationale underlying vitamin D
testing and supplementation for deficiency may seem straightforward, in
actuality, the metabolism and physiologic functions of vitamin D in the body
are quite nuanced and complex, and there remains significant controversy
surrounding the appropriate utilization of vitamin D measurement and clinical
interpretation of vitamin D test results. In this post, let’s review the basic
principles of vitamin D metabolism, its function and mechanisms of regulation
in the human body, methods of measurement in the laboratory, and ramifications
of vitamin D values on clinical decision-making and management.
Vitamin D Metabolism
Vitamin D is a fat-soluble vitamin and encompasses a group
of compounds, all containing a four-ring steroid backbone. The two main forms
of vitamin D utilized by humans are vitamin D3 (cholecalciferol) and
vitamin D2 (ergocalciferol). Vitamin D3 is primarily
synthesized in the skin from 7-dehydrocholesterol in the presence of sunlight
(UVB rays), while vitamin D2 is synthesized in plants from
ergosterol and is used to fortify many foods (milk, bread, cereal, etc.).1
Once synthesized in the skin or ingested from the
gastrointestinal tract, both vitamin D2 and vitamin D3
travel in the bloodstream (bound to vitamin D-binding protein) to the liver,
where both are converted to 25-hydroxyvitamin D [25(OH)D,
calcidiol/calcifediol] by the action of 25-hydroxylase.1,2 While 25(OH)D
has only limited biologic activity, it has a very long half-life (2-3 weeks)
and is therefore the primary form of vitamin D found in the blood.1 Notably,
the half-life of 25(OH)D2 is shorter than that of 25(OH)D3
(possibly due to lower affinity to vitamin D-binding protein) and therefore it
is present in significantly lower concentrations than 25(OH)3 in the blood.3
25(OH)D is then further converted to 1,25-dihydroxyvitamin D
[1,25(OH)2, calcitriol] via the action of 1-α-hydroxylase primarily in the
kidney.1 In contrast to 25(OH)D, 1,25(OH)2D is the
biologically active form of vitamin D, but it has a much shorter half-life (5-8
hours) and therefore has much lower circulating levels in the blood.1
25(OH)D may alternatively be converted to 24,25-dihydroxyvitamin D [24,25(OH)2D]
by 24-α-hydroxylase,
also in the kidney. 24,25(OH)2D is an inactive metabolite and thus
serves as an end-product in this degradation-type pathway of 25(OH)D.1,4
Vitamin D Physiology
The overall effect of vitamin D in the body is to increase
calcium and phosphate levels in the blood. Via binding of 1,25(OH)2D
to nuclear receptors within cells, it acts at three main sites: 1) the
intestine, where it increases calcium and phosphate absorption, 2) the bones,
where it increases calcium resorption by promoting osteoclast maturation, and
3) the kidney, where it increases calcium reabsorption by enhancing the effects
of parathyroid hormone (PTH) on the distal convoluted tubule.1
Conversion of 25(OH)D to 1,25(OH)2D by
1-alpha-hydroxylase is tightly regulated by calcium, phosphate, and PTH
concentrations in the body. Decreased calcium or phosphate levels, or increased
PTH levels in the blood (most commonly resulting from a fall in calcium) will
stimulate 1-α-hydroxylase
activity and lead to increased production of 1,25(OH)2D, while
increased calcium or phosphate levels or decreased PTH levels will suppress 1-α-hydroxylase
activity and thus lead to decreased production of 1,25(OH)2D.1,2
From a clinical perspective on vitamin D physiology, there
are numerous causes of abnormal vitamin D levels in the body. Here are some
common causes of low vitamin D levels:
Inadequate intake of vitamin D (whether from
diet, inadequate sunlight, or malabsorption)
Decreased PTH (hypoparathyroidism,
hyperphosphatemia, hypercalcemia of malignancy)
End-organ resistance to PTH
(pseudohypoparathyroidism)
Decreased 1-α-hydroxylase activity (renal
failure, vitamin D-dependent rickets type 1)5
Conversely, causes of high vitamin D levels are listed
below:
Excessive intake of vitamin D (usually from
supplements)
Increased PTH (primary hyperparathyroidism)
Increased extrarenal 1-α-hydroxylase activity (seen in
granulomatous diseases such as sarcoidosis, as well as some lymphomas)
End-organ resistance to vitamin D (vitamin
D-dependent rickets type 2)5
Vitamin D Measurement
in the Laboratory
25(OH)D is the most commonly measured vitamin D metabolite
in laboratory assays, since (as mentioned above) it has a longer half-life and
a larger concentration in the blood compared to 1,25(OH)2D. In
addition, its concentration does not fluctuate as significantly as that of 1,25(OH)2D,
since its production from 25-hydroxylase in the liver is not so tightly
regulated as 1-α-hydroxylase activity in the kidney.1,6
Nevertheless, 1,25(OH)2D measurement is indicated in a few specific
clinical circumstances, including workups for idiopathic hypercalcemia and
bone/mineral disorders, and for evaluation of vitamin D status in the setting
of renal failure (where 1-α-hydroxylase activity is decreased).1,7
While the gold standard for vitamin D measurement is liquid
chromatography coupled to tandem mass spectrometry (LC-MS/MS), most
laboratories utilize immunoassays (including radioimmunoassays,
chemoluminescent immunoassays, and enzyme-linked immunoassays) for vitamin D
quantitation.1,7 One significant difference between these two
methods is that while LC-MS/MS can differentiate vitamin D3 and
vitamin D2 metabolites, immunoassays cannot.6 In
addition, the antibodies used in many 25(OH)D immunoassays often have lower
cross-reactivities with 25(OH)D2 and therefore may underestimate
this form when giving the total 25(OH)D value.6 These antibodies
also have varying cross-reactivities with other vitamin D metabolites and so
may result in an overestimation of the total 25(OH)D due to positive
interference from these metabolites.6
Another advantage of the LC-MS/MS method is that it can
detect C3 epimers of 25(OH)D, while immunoassays cannot.8 The
physiologic significance of these epimers has not yet been clearly delineated,
but recent evidence has shown that while these epimers do not affect calcium concentrations,
they do contribute to suppression of PTH levels.8 In addition, while
these epimers comprise a low proportion (about 2-3%) of the overall 25(OH)D
concentration in adults, they have been found in significantly higher
proportions (up to 60%) in infant and pediatric populations.8,9
Thus, the detection of these epimers (and their quantitation, which is possible
through high-performance LC-MS/MS) may be more important in these patient
populations.
Interpretation of
Vitamin D Results
The optimal serum levels of 25(OH)D are not universally
established. First of all, levels vary with factors affecting sunlight exposure
including latitude, skin pigmentation, and sunscreen use.1 Levels
also demonstrate significant seasonal variation, with winter measurements up to
40-50% lower than summer measurements.1 Recommended minimum 25(OH)D
levels for optimal bone health differ among various national organizations and
generally range from 20 ng/mL to 30 ng/mL; as mentioned above, these thresholds
are controversial and there is no established consensus.10-12
Vitamin D deficiency is very common, with the majority of
patients exhibiting no clinical symptoms and normal calcium and phosphate concentrations.
However, a significant proportion of these asymptomatic patients will have
increased PTH levels and concomitant increased risk of osteopenia/osteoporosis
and fractures; therefore, all patients with vitamin D deficiency should be
treated with repletion.13 If deficiency is severe and persistent,
bone demineralization with rickets (in children) and osteomalacia (in adults
and children) can develop. In contrast, vitamin D toxicity is very rare and is
usually associated with over-supplementation; patients develop hypercalcemia
with related symptoms including confusion, muscle weakness, nausea and
vomiting, and polydipsia and polyuria.14
Recent studies have linked vitamin D deficiency (usually
with residency at higher latitudes) to a wide variety of clinical disorders
ranging from autoimmune diseases (multiple sclerosis, rheumatoid arthritis,
type I diabetes), to cancers (including colon, breast, and prostate), to
psychiatric illnesses (schizophrenia, depression), and cardiovascular disease
(including hypertension and congestive heart failure).15 Whether
these links possess a causal basis or are merely associative needs to be
further investigated. Nevertheless, what is certain is that understanding the
functions of vitamin D in the body and methodologies of vitamin D measurement
in the laboratory is crucial in appreciating its clinical significance and
various, ever-expanding applications in disease pathophysiology and management.
References
McPherson RA, Pincus MR. Henry’s Clinical
Diagnosis and Management by Laboratory Methods. Elsevier Health Sciences; 2017.
Brown AJ. Regulation of vitamin D action.
Nephrology, dialysis, transplantation: official publication of the European
Dialysis and Transplant Association-European Renal Association. 1999 Jan 1;14(1):11-6.
Armas LA, Hollis BW, Heaney RP. Vitamin D2 is
much less effective than vitamin D3 in humans. The Journal of Clinical
Endocrinology & Metabolism. 2004 Nov 1;89(11):5387-91.
Cashman KD, Hayes A, Galvin K, Merkel J, Jones
G, Kaufmann M, Hoofnagle AN, Carter GD, Durazo-Arvizu RA, Sempos CT.
Significance of serum 24, 25-dihydroxyvitamin D in the assessment of vitamin D
status: a double-edged sword?. Clinical chemistry. 2015 Apr 1;61(4):636-45.
Clarke W. Contemporary practice in clinical
chemistry. Amer Assn for Clinical Chemistry; 2016.
Zerwekh JE. Blood biomarkers of vitamin D
status. The American journal of clinical nutrition. 2008 Apr 1;87(4):1087-91.
Hollis BW. Assessment and interpretation of
circulating 25-hydroxyvitamin D and 1, 25-dihydroxyvitamin D in the clinical
environment. Endocrinology and Metabolism Clinics. 2010 Jun 1;39(2):271-86.
Lutsey PL, Eckfeldt JH, Ogagarue ER, Folsom AR,
Michos ED, Gross M. The 25-hydroxyvitamin D3 C-3 epimer: distribution,
correlates, and reclassification of 25-hydroxyvitamin D status in the
population-based Atherosclerosis Risk in Communities Study (ARIC). Clinica
chimica acta. 2015 Mar 10;442:75-81.
Singh RJ, Taylor RL, Reddy GS, Grebe SK. C-3
epimers can account for a significant proportion of total circulating
25-hydroxyvitamin D in infants, complicating accurate measurement and
interpretation of vitamin D status. The Journal of Clinical Endocrinology &
Metabolism. 2006 Aug 1;91(8):3055-61.
Del Valle HB, Yaktine AL, Taylor CL, Ross AC,
editors. Dietary reference intakes for calcium and vitamin D. National
Academies Press; 2011 Apr 30.
Vieth R. What is the optimal vitamin D status
for health?. Progress in biophysics and molecular biology. 2006 Sep 1;92(1):26-32.
American Geriatrics Society Workgroup on Vitamin
D Supplementation for Older Adults. Recommendations abstracted from the
American geriatrics society consensus statement on vitamin D for prevention of
falls and their consequences. Journal of the American Geriatrics Society. 2014
Jan;62(1):147-52.
Valcour A, Blocki F, Hawkins DM, Rao SD. Effects
of age and serum 25-OH-vitamin D on serum parathyroid hormone levels. The
Journal of Clinical Endocrinology & Metabolism. 2012 Nov 1;97(11):3989-95.
Ozkan B, Hatun S, Bereket A. Vitamin D
intoxication. Turk J Pediatr. 2012 Mar 1;54(2):93-8.
Holick MF. Vitamin D deficiency. New England
Journal of Medicine. 2007 Jul 19;357(3):266-81.
-Michelle Lin, MD, is a second-year anatomic and clinical pathology resident at Houston Methodist Hospital in Houston, Texas.
There are often new buzzwords flying around that everyone uses, but few actually understand what they mean. Personalized and precision medicine are two of these terms that are often used interchangeably. Every lab wants to say they are performing personalized medicine. And to be fair we really do all provide personalized medicine in some form. Almost all lab results are used to customize the treatment for patients. However these buzzwords are used to refer to tests that describe linking genetic, lifestyle, or environmental information with predicted response to treatment. Precision medicine may be the more accurate term to describe identifying effective treatment for the right patient at the right time based on genetic, lifestyle, or environmental information. The term personalized medicine may give the false impression that therapies were developed specifically for the patient, when really they are developed to target a specific genotype or phenotype.
One example of precision medicine being used clinically today
is in oncology. Many cancer drugs now require an associated test to determine
the presence or absence of a specific biomarker to determine which patients are
likely respond to the therapy. The biomarker tests that are linked to a
specific therapy are called companion diagnostics. Biomarkers analyzed can be a
specific protein or gene such as programmed death ligand-1 (PD-L1) or epidermal growth factor receptor (EGFR) or they can be much broader such
as tumor mutational burden (TMB) or immune signatures. Identifying biomarkers that
determine which patients are likely to respond to therapy and only giving
patients with the biomarker the drug increases response rates to the therapy
and may decrease side effects. More than half of the clinical trials for cancer
drugs in 2018 were linked to a specific biomarker. Linking drug selection with
specific laboratory tests is causing an increased need for multidisciplinary
collaboration among pathology, oncology, and the laboratory.
In our lab we perform precision medicine using PCR or NGS
assays to analyze patient’s tumor for specific genes. Although we still perform
single gene testing when ordered, most of our cases are analyzed by a NGS
panel. NGS panel testing allows us to look at numerous biomarkers with one
test. This decreases the cost, time and tissue utilized to determine the
patient’s biomarker status. Our NGS panel analyzes 52 genes to look for
mutations that would indicate a patient is likely to respond to a targeted
therapy. Most of our oncology testing is done on lung, colon, and melanoma
specimens, although the panel is validated for most solid tumors. The report
that we issue the oncologist provides clear information on which therapies the
patient is likely to respond to or likely to be resistant to based on their
tumor’s genetic profile. We also include information in the report to match
patients to clinical trials. Precision medicine utilizing panel NGS testing for
predicted response to treatment is becoming standard of care for many solid
tumors.
-Tabetha Sundin, PhD, HCLD (ABB), MB (ASCP)CM, has over 10 years of laboratory experience in clinical molecular diagnostics including oncology, genetics, and infectious diseases. She is the Scientific Director of Molecular Diagnostics and Serology at Sentara Healthcare. Dr. Sundin holds appointments as Adjunct Associate Professor at Old Dominion University and Assistant Professor at Eastern Virginia Medical School and is involved with numerous efforts to support the molecular diagnostics field.
A 65 year
old man with diabetes mellitus type 2 presented to the emergency department
(ED) for left hip pain. He has a remote history of avascular necrosis of
bilateral hips of unknown etiology for which he received a bilateral total hip
arthroplasty and subsequent multiple revisions due to hardware failure several
years ago. He initially presented to an urgent care clinic a few months prior
for “noise with movement” of the left hip and mild lower back pain. Plain radiographs
of the left hip in comparison to his prior imaging were unremarkable and he was
subsequently discharged. Repeat imaging at a follow-up visit at the orthopedic
clinic showed mild superior migration of the femoral head bilaterally secondary
to periprosthetic osteolysis of
the joint headliner. He was scheduled for surgery however presented to the ED prior
to his scheduled appointment with severe crushing left hip pain and restricted
joint mobilization. He denied fevers, chills, night sweats, or any other recent infections. The left
hip was aspirated yielding
10cc of dark
black fluid and a stat gram stain was ordered.
Laboratory identification
The stat gram stain showed many
polymononuclear cells with moderate gram positive bacilli in a background of
dark inorganic material (Image 1). Following 48 hours of incubation, there was anaerobic
growth on the kanamycin and vancomycin (KV) and schaedler agar
plates. A Gram stain of the broth showed gram positive bacilli arranged
singly and in chains with some decolorization (Image 2). The KV and schaedler plates showed moderate growth of a single
organism consisting of small glossy tan colored colonies (Images 3-4). No
aerobic growth was observed on the blood, MacConkey, Columbia Naladixic Acid (CNA),
or chocolate agar plates. Mass
spectrometry (MALDI-TOF) identified the
pathogenic organism as Clostridium innocuum.
Image 1. Synovial fluid Gram stain of the left hip showed moderate gram positive bacilli and many polymononuclear cells in a background dark inorganic debris (100x oil immersion).Image 2. Gram stain from a positive broth culture showed gram positive bacilli arranged singly and in chains with some decolorization (100x oil immersion).Image 3. Anaerobic growth on the schaedler agar showed growth of a single organism consisting of small round glossy tan colored colonies. Image 4. Anaerobic growth on the kanamycin and vancomycin (KV) agar showed growth of a single organism consisting of small glossy tan colored colonies.
Discussion
Bacterial joint infections are more common in prosthetic joints as
compared to native joints with a prevalence of 1-2% following hip arthroplasty
(1). Most cases of bacterial septic
arthritis are due to staphylococci (40 percent),
streptococci (28 percent) or gram negative bacilli (19 percent) organisms (2). Joint
infections secondary to anaerobes are less likely and account for 2-3%
of all cases (3). A review of the literature shows less than 50 documented
cases of septic arthritis due to Clostridium species. Amongst these
cases Clostridium perfringens is the most commonly isolated pathogen (4).
To date there are no documented cases of joint infections secondary to Clostridium
innocuum species.
Clostridium innocuum is a non-motile, anaerobic, gram positive organism
that reproduces by sporulation. These organisms are normally found as a part of
the usual human gut flora and are rarely human pathogens. The name “innocuum”
is derived from the term “innocuous” to convey the innocence of these organisms
as they do not produce clostridial exotoxins. A review of the literature shows
fewer than 20 reported cases of Clostridiuminnocuum infections
with most reported cases being described in immunocompromised patients such as
those with diabetes mellitus, chronic
hepatitis, acquired immune deficiency syndrome (AIDS), leukemia, and
organ transplantation (5-6). Clinically patients can present with a spectrum of
symptoms which include fever
of unknown origin, diarrhea/constipation, and non-specific respiratory symptoms.
In almost all cases bacteremia ensued. Most
cases were associated with a traumatic penetrating injury with few reported
cases due to hematogenous spread (5-6).
Laboratory identification of Clostridiuminnocuum can be challenging due to its variable gram staining morphology and
atypical colony morphology on differing culture media. Most traditional
phenotypic methods can only reliably identify these organisms to the genus
level as a Clostridium species. However, using mass spectrometry
(MALDI-TOF) these organisms can be identified to the species level. Rapid
identification of Clostridium innocuum from the subset of Clostridium
species is clinically important as these organisms are the only known Clostridium
species with intrinsic resistance to vancomycin (7). Although they do not
possess clostridial exotoxins, these organisms are thought to have a
lipopolysaccharide-like virulence factor and have a mortality rate comparable
to toxigenic Clostridium species (7). Due to resistance to vancomycin, metronidazole, piperacillin and ampicillin-sulbactam are the
alternative recommended first-line treatment options.
For this
patient, following the results of the gram smear the patient was started on IV vancomycin
but due to an adverse allergic reaction was switched to intravenous pencillin G
and oral ciprofloxacin. He was subsequently taken to the operating room for
incision and drainage and left hip revision arthroplasty with cup exchange. Blood
cultures were collected post-operatively and showed no growth, possibly due earlier
antibiotic administration. Susceptibility studies from Mayo Laboratories showed
pan susceptibility to penicillin, piperacillin-tazobactam, ertapenem,
clindamycin, and metronidazole. The patient was subsequently switched to
intravenous penicillin and continued to show clinical improvement during his
remaining hospital course.
References
Horowitz DL,
Katzap E, Horowitz S, Barilla-labarca ML. Approach to septic arthritis. Am Fam
Physician. 2011;84(6):653-60.
Ryan MJ,
Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and
Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol.
1997;36(3):370-3.
Gredlein CM,
Silverman ML, Downey MS. Polymicrobial septic arthritis due to Clostridium
species: case report and review. Clin Infect Dis. 2000;30(3):590-4.
Leal J,
Gregson DB, Ross T, Church DL, Laupland KB. Epidemiology of Clostridium species
bacteremia in Calgary, Canada, 2000-2006. J Infect. 2008;57(3):198-203.
Lee NY,
Huang YT, Hsueh PR, Ko WC. Clostridium difficile bacteremia, Taiwan. Emerging
Infect Dis. 2010;16(8):1204-10.
Chia JH,
Feng Y, Su LH, et al. Clostridium innocuum is a significant
vancomycin-resistant pathogen for extraintestinal clostridial infection. Clin
Microbiol Infect. 2017;23(8):560-566.
-Noman Javed, MD is a 3rd year anatomic and
clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
The following case is an interesting overlap of
Hematopathology and Molecular Diagnostics, and shows the utility of sequencing
to detect a cancer before biopsy could.
A 63 year old gentleman presented to a heme/onc physician
with six months of intractable anasarca, fatigue, and a recent mild
thrombocytopenia (Table 1). They were otherwise in healthy condition. The
physician initiated a lymphoma work-up that included a bone marrow biopsy. The
tests were negative for M-protein.
Table 1. Summary of symptoms and relevant abnormal labs.
The bone marrow biopsy was somewhat limited, but the core contained multiple marrow elements. After a thorough review by a Hematopathologist, no evidence of dysplasia or other irregularities could be detected (Image 1). Flow cytometry detected no aberrant blast population. Cytogenetics detected 20del [16/20] and 5del [3/20]. These findings did not clearly indicate a specific diagnosis.
Image 1. 40x view of the bone marrow specimen at the initial presentation. No evidence of dysplasia was found.
As the clinical suspicion for a malignancy was high, the
bone marrow specimen was sent for sequencing on a 1385-gene panel test. The
test included tumor-normal matched DNA sequencing (“tumor” sample: bone marrow,
normal: saliva), RNA whole transcriptome sequencing on the bone marrow, and
Copy Number Variant (CNV) analysis. Tumor-normal matched sequencing helps rule
out variants that are normal and present in the patient.
Somatic mutations were determined as those that were present
in the “tumor” sample and not in the matched normal sample. The somatic
variants found are listed below with their variant allele frequency (VAF) in
parenthesis. Recall that a VAF of 40% means that a mutation is present in the
heterozygous state in 80% of cells.
IDH2 (p.R140Q, 46%)
SRSF2 (p.P95T, 51%)
CBL (p.R499*, 47%)
KRAS (p.K117N, 12%)
Figure 1. View of IGV, which displays the NGS reads for IDH1 along with the variant allele highlighted in red. The color of the bars indicates the direction of the reads (forward in red and reverse in blue). This reflects the allele frequency of approximately 50%.
The mutations in these genes are commonly found in myeloid
cancers including myselodysplastic syndrome. Activating mutation in IDH2 (isocitrate dehydrogenase 2)
increase the production of the oncometabolite 2-HG, which alters methylation in
cells taking them to an undiffereitiated state. SRSF2 (Serine And Arginine Rich Splicing Factor 2) is a part of the
spliceosome complex, which regulates how sister chromatids separate from each
other. Failures in the proper function of the complex creates genomic
instability. CBL (Casitas B-lineage
Lymphoma) is a negative regulator of multiple signaling pathways, and loss of
function mutations (as seen here) lead to increased growth signals through
several tyrosine kinase receptors. KRAS
(Kirsten RAt Sarcoma virus) is an upstream mediator of the RAS pathway, which
acquires mutations that lead to constitutive activation and sends growth
signals to cells causing them to proliferate.
Furthermore the CNV analysis
also found the heterozygous loss of chromosome 20 as reported in cytogenetics.
CNV analysis did not detect chromosome 5 deletion, as it was below the limit of
detection (20% for CNV analysis).
Figure 2. This plot shows the normalized read frequency of genes across each of the chromosomes is shown here. The drop at chromosome 20 is shown in a pale brown color on the right side of the graph. This is consistent with the cytogenetic findings. The loss of 5q isn’t seen as it is below the limit of detection of 30%.
These mutations are all individually common in MDS, but the co-occurance of each gives very strong evidence that MDS is the diagnosis (Figure 3). There have also been studies that provide prognostic implications for several of the genetic mutations present. Some mutations like SRSF2 or CBL at high VAF (>10%) indicate a poor prognosis, but mutations in IDH2 or TP53 at any frequency have not only a high chance of progression, but also a faster time to onset of disease. Another non-genetic risk factor for developing MDS is an elevated RDW, which we saw in our patient.
Figure 3. From Becker et al 2016.
All of these high-risk factors together led us to push for a diagnosis of MDS based off of molecular findings, and the patient was started on treatment with Azacitadine. Our assessment was confirmed 3 months later when, the patient’s follow up bone marrow biopsy showed significant progression with megakaryocytic and erythroid dysplasia and hyperplasia and reticulin fibrosis MF2 (Image 2). Aberrant blasts were detected (1-2%), but not elevated. This demonstrates how molecular findings predicted and predated the patient’s rapid progression to morphologic disease.
Image 2. Dysplastic, hyperplastic megakaryocytes and erythroid lineage.
In summary, multiple molecular mutations indicative of MDS
were found in a symptomatic patient’s unremarkable bone marrow biopsy months
before a rapid progression to MDS.
References
Steensma DP, Bejar R, Jaiswal S et al. Blood 2015;126(1):9-16.
Sellar RS, Jaiswal S, and Ebert BL. Predicting progression to AML. Nature Medicine 2018; 24:904-6.
Abelson S, Collord G et al. Prediction of acute myeloid leukemia risk in healthy individuals. Nature 2018; 559:400-404.
Desai P, Mencia-Trinchant N, Savenkov O et al. Nature Medicine 2018; 24:1015-23.
Becker PM. Clonal Hematopoiesis: The Seeds of Leukemia or Innocuous Bystander? Blood.2016 13(1)
-Jeff SoRelle, MD is a Chief Resident of Pathology at the
University of Texas Southwestern Medical Center in Dallas, TX. His
clinical research interests include understanding how the lab intersects
with transgender healthcare and improving genetic variant
interpretation.
The majority of laboratory injuries and exposures are
preventable, and most of them occur because staff is not paying close attention
to the situation. They lose their situational awareness or were never paying
attention to it from the start. Unfortunately, lab safety professionals spend
much of their time investigating such incidents rather than being able to
prevent them. If laboratory staff could understand the power of the pause, labs
would have fewer dangerous incidents.
One illustration of that power can be seen in a simple
exercise. A group of people is asked to read aloud quickly a list of words that
indicate different colors- green, red, etc. The words themselves, however, are
written in different colors, and the colors do not match the words. For
example, the word “red” is written in black, the word “blue” is written in
green, etc. This first part goes well, you’re just asking them to read the
actual words. Next, however, it gets harder. The people are asked to quickly go
down the list again, but this time they are asked to say the color of the word,
not that actual word. Typically, this does not go well. For the next step, the
exercise is repeated at a much slower pace, with a slight pause between each
word. Once a pause is placed between each word, the people recite the correct
colors. The incongruent words and colors creates what is known as the “Stroop
Effect,” first theorized in 1935, but pausing is a means of overcoming this
issue in our brains.
When investigating a needle stick incident, the lab safety
officer learned the employee completed the draw, attempted to engage the needle
safety device, but stuck their finger when grabbing the needle to toss it into
the sharps container. She did not notice the safety device did not engage and
the needle was still exposed. The employee stated she was busy and in a hurry
because there were many other patients waiting. I have always said that when a
lab employee is stressed and busy, that’s when stopping for a moment to gain
situational awareness is most important. Had this employee paused for a moment
to ensure the needle safety device was fully engaged, the incident would never
have occurred.
The lab manager had to speak to a chemistry tech after a
serum splash exposure to the eyes. When looking at the work area, the manager
noticed there was an adjustable face shield in place but that staff moved it
into place only when needed. The tech admitted he was busy at the time of the
splash and that he neglected to move the shield into place before uncapping
specimens. Again, a pause to think about safety here would have helped.
In another situation, a microbiology technologist was eager
to start the day and get it done since her vacation began the next day. She
quickly went through the daily checklist and checked items off but did not
actually perform the checks. Halfway through the day, she noticed it seemed
warm and that it was unusually quiet at her biological safety cabinet work
station. She decided to look at the gauges and noticed that there was no
protective air flow in operation. She had been working with TB samples all
morning. When she reported the issue, the manager told her that all employees
in the area would need to go to Employee Health and be followed up for TB
exposures. Pausing to perform the safety checks at the beginning of the shift
would have made a big difference in that outcome for several employees.
Pausing for safety in the laboratory setting can be a
powerful tool, even during the busiest moments. In fact, that’s when it works
best. Use that pause in your arsenal, and teach maintaining situational
awareness with your staff so that future injuries and exposures can be
prevented.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A man in his 40’s with a past medical history of acute
lymphoblastic leukemia/lymphoma (in remission), multiple infections including
bacteremia and pulmonary aspergillosis, presented to the hospital with fever
and diarrhea. Over the course of his stay, he had worsening renal function and
developed profound hypotension and shock, which prompted initiation of two
vasopressors and high-dose steroids. Eventually he developed acute hypoxic
respiratory failure, requiring intubation. Complete blood count demonstrated an
absolute eosinophilia of 8.58 x109/L (reference range 0.04-0.62 x109/L).
Imaging revealed bilateral pulmonary infiltrates and a pleural effusion.
Respiratory culture with gram stain was ordered for his tracheal aspirate,
which revealed few polymorphonuclear cells, many gram-negative rods, yeast, and
larvae of Strongyloides stercoralis (Image
1A). Wet mounts of the tracheal aspirate revealed numerous larvae and a few
eggs of S. stercoralis (Image 1B-C);
many of the larvae were motile (Movie 1). Stool examination of ova and
parasites (O & P) were positive for larvae. Given the burden of organisms
and prior administration of steroids, he was diagnosed with severe
strongyloidiasis, consistent with hyperinfection. Concurrent blood cultures
grew Enterococcus faecalis and Stenotrophomonas maltophilia; the
respiratory culture also grew S.
maltophilia, and tracks from the migrating larvae were observed on
respiratory culture bacterial media (Image 1D).
Image 1. Tracheal aspirate Gram stain with S. stercoralis larvae, 100x objective magnification (A). Wet mount of tracheal aspirate revealing larvae (B) and eggs (C), 40x objective magnification. Blood agar plate growing S. maltophilia in an abnormal pattern, indicating motile larvae tracking through the agar (D).
Discussion
Strongyloidiasis is a spectrum of clinical disease caused by
the nematode Strongyloides stercoralis.1,2
Descriptions of acute infection have been described in other Lablogatory
entries here,3,4 and the full lifecycle is described in detail on
the CDC DPDx website.5
Severe strongyloidiasis includes the syndromes of
hyperinfection and disseminated disease. Hyperinfection
is when there is an elevated burden of the typical autoinfection cycle
involving the lungs and GI-tract. Usually there is an antecedent
immunosuppressive event, such as administration of corticosteroids. Within the
GI-tract lumen, increased numbers of rhabditiform larvae transform into the
infective filariform larvae, which traverse the GI mucosa, migrate to the lungs
via bloodstream/lymphatics where they enter alveolar air spaces, then ascend
the respiratory tract, and are coughed up by the host and swallowed to re-enter
the GI tract. In the GI tract adult females lay eggs through parthenogenesis,
which give rise to further rhabditiform larvae. In extreme cases of
hyperinfection, adults can be found in the lungs, where they may also lay eggs.
Finding eggs in respiratory specimens is unusual, and may be related to the
burden of disease.6
Disseminated disease
is when larvae can be found in any additional organs/organ systems, such as the
central nervous system, kidneys, liver, adrenals, etc. Invasive sampling is not
typically performed, and larvae can be observed at autopsy.
Laboratory diagnosis of S.
stercoralis involves identification of rhabditiform larvae in stool O
&P exam; the presence of adults or eggs in stool is rare. Rhabditiform
larvae have short buccal cavities and an ovoid genital primordium structure midway through the body (Movie 2).
O&P exams can be performed on other body fluids, such as sputum and CSF.
Serology can be useful to identify past exposure, especially prior to
initiating immunosuppressive therapeutics such as corticosteroids. A
nonspecific finding can be observed, as in this case, in the complete blood
cell count and differential. Relative and absolute eosinophilia can be found in
patients with parasitic infections; therefore, it is reasonable to rule out
parasitic infection in this subset of patients. In the case presented here, the
absolute eosinophilia was likely due to a persistent S. stercoralis infection, since these nematodes can live in the
human host for decades.
The treatment of choice for severe strongyloidiasis is oral
ivermectin, though albendazole is an alternative therapy. In some instances,
subcutaneous ivermectin administration may be used.7
Follow-up
Oral ivermectin was administered to treat the
strongyloidiasis and antibiotics were administered to treat the bacterial
infections. Over the coming days, serial tracheal aspirates continued to reveal
many larvae and eggs, so therapy was escalated to subcutaneous ivermectin. Over
the course of therapy, the patient developed a fungemia with Candida guilliermondii. Despite
aggressive antimicrobial therapy and intensive care, the patient remained
hypoxemic and hypotensive. The family decided to transition to comfort measures
and the patient passed away.
References
Maguire JH. Intestinal Nematodes (Roundworms), in Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, B. Mandell, Dolin, Editor. 2010, Elsevier: Philadelphia, PA. p. 3577-3586.
Parasitology, in Koneman’s Color Atlas and Textbook of Diagnostic Microbiology, Procop et al., Editors. 2017, Lippincott Williams & Wilkins: China. p. 1452-1454.
Keiser PB and Nutman TB. Strongyloides stercoralis in the Immunocompromised Population. Clin Microbiol Rev, 2004. 17(1): p. 208-17.
Hurlimann E and Keiser J, A single dose of ivermectin is sufficient for strongyloidiasis. Lancet Infect Dis, 2019. 19(11): p. 1150-1151.
-IJ Frame, MD, PhD, Microbiology Fellow, University of Texas Southwestern Dallas, Texas
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
“Never, ever underestimate the importance of having fun,”
said Randy Pausch, a professor of computer science at Carnegie Mellon
University. Indeed, having fun is an important component of life, and that
includes your professional life. However, having fun in the workplace can seem
like an impossible task sometimes. There is, after all, lots of work to be
accomplished, performance to be measured, and projects to complete. This can
make it challenging to find of time and ways to have fun appropriately and
constructively.
The benefits of having fun in the workplace are plentiful. Because
most fun activities require people to work in groups or teams, the shared
experience can increase collaboration, engagement, and foster communication. Having
fun fosters motivation and commitment to an organization as people associate
the positive feelings and experiences with the workplace. This also increases
morale and comradery among the participants, which increases their performance.
All these aspects, in turn, foster creativity, innovative thinking, and
problem-solving skills. The more creative employees are, the more comradery
they feel among themselves, and the better they perform the more turnover is
reduced. Having fun in the workplace is incredibly beneficial to both the
employees and the organization overall.
In today’s workplace culture, people are generally more
aware and considerate of what is appropriate behavior. This also applies to
having fun, because if activities are only fun and enjoyable if they are
appropriate for everyone involved. It is, therefore, important to establish
clear boundaries: what is considered part of this activity and what is not. It
is also important to consider different levels of physical, mental, and
emotional ability. Having fun is inclusive and collaborative, so it is critical
to design activities that everyone can partake in. The activity should also
always be optional. Making participation mandatory is not actually fun for people,
so make sure that there is an opt-in and opt-out option. Finally, every
activity should have some element of learning and education. If you are asking
people to participate in a fun activity, ensure that they are learning
something about one another or about a specific topic.
There are many different ways in which you can incorporate
fun in the workplace. Last year at ASCP, our social committee hosted an ‘Oscar
Party” in which we could vote for our colleagues in categories such as “Outside
the Box Thinker/Innovator,”, “Outstanding Philanthropist,” and “Rookie of the
Year.” Then all staff gathered in the kitchen area of our office that was
decorated with a red carpet and we all received a glass of sparkling cider. The
winners were announced and cheered on as they walked the red carpet. They gave
a short speech after receiving their little Oscar award. It was a simple way to
have some collective fun and it felt so great cheering everyone on and
recognizing certain employees for their outstanding contribution to the society.
On average, babies laugh about 400 times a day. Adults, on the other hand, only laugh about 35 times a day and significantly less often on weekdays than on weekend (Beard, 2014). Laughter is incredibly important to our overall well-being and performance. In fact, “laughter relieves stress and boredom, boosts engagement and well-being, and spurs not only creativity and collaboration but also analytic precision and productivity”(Heggie, 2018). So, let’s try to incorporate more fun and more laughter in both our personal and our professional lives. Let’s find ways to cheer each other up and create a collaborative, warm, and productive environment that fosters engagement, retention, and analytic precision. After all, laughter is the best medicine.
-Lotte Mulder, EdM, is the Senior Manager of Organizational Leadership and Patient Engagement at ASCP. She earned her Masters of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. After she graduated, Lotte started her own consulting company focused on establishing leadership practices in organizations, creating effective organizational structures, and interpersonal coaching. She has worked in Africa, Latin America, Asia, and the U.S. on increasing leadership skills in young adults through cultural immersion, service learning and refugee issues, and cross-cultural interpretation. She is currently working toward a PhD in Organizational Leadership.
During the 2019 ASCP Annual Meeting in Phoenix, I noticed a
morning workshop session entitled “The Impact of Fun.” The title intrigued me,
so decided to take a break from the science and clinical medicine workshops
that I would normally attend, and take advantage of the opportunity to listen
in.
I have been working as a pathologist and lab director for 30
years, and while I hate to admit it, I had never thought seriously about taking
time during the day for playing games with my co-workers. I was always consumed
with meetings, deadlines, and getting the clinical work completed.
At the beginning of the course, I was a little unsure what I
had gotten myself into. However by the time the workshop concluded, the reality
of what I had been missing had set in.
When I returned to work following the meeting, I began to
search for fun activities that our lab team could do over a lunch hour. I set a
date and promised food to entice the wary into attending the event in the
conference room. Once they had assembled, I divided the group into two teams by
drawing an imaginary line down the middle of the room. We then played team trivia
using a book of questions I had acquired. By the end of the hour, everyone was
laughing and having fun. The lab continued to buzz with talk and occasional
laughter all afternoon.
We have continued setting aside one noon hour each month
where we gather for different types of games. Charades, and Pictionary have
been hits. Mostly everyone brings their own lunch, but food or deserts are
provided on occasion to keep these events special. There are a few who choose
not to participate, but even they occasionally show up to watch and laugh along
with the rest. As is pointed out above, you cannot make having fun a mandatory
or it ceases to be fun.
Our lab staff really seem to enjoy these events and so does
this old pathologist. During our most recent event, one of my young colleagues
remarked how much fun these lunches have been, and that they hoped we would
continue these going forward. I intend to keep these going as long as I
continue working. It has provided me with an opportunity to get to know each of
my co-workers much better. I only wish I had learned about the importance of
having fun with your co-workers and teammates earlier in my career. I encourage
other pathologists, lab directors and section supervisors to learn from my
experience and begin finding ways to bring the fun back into the workplace if
you have not already done so.
-Dr. Wisecarver is currently Professor Emeritus in the Department of Pathology/Microbiology at the University of Nebraska Medical Center in Omaha, Nebraska. He served as Medical Director of the Clinical Laboratories for Nebraska Medicine, their clinical affiliate from 1996 until 2017. He currently serves as the Director of the Histocompatibility Laboratory for Nebraska Medicine.
A 77 year old male presented to the hospital with chest
pain, lightheadedness, burning urination for the past few weeks. He has blood
in his urine due to a previously diagnosed neoplasm. The patient moved from
India to the United States in February, with a diagnosis of bladder cancer and
a history of hypertension, congestive heart failure, coronary artery disease,
and atrial fibrillation. In the hospital, abscesses on both right and left
kidneys were found, and patient had nephrostomy tubes placed. Purulent
discharge confirmed he had a severe urinary tract infection.
Laboratory Identification
The patient’s urine culture grew >100,000 colony forming
units/milliliter (CFU/ml) of an oxidase-positive, non-lactose fermenting
Gram-negative rod. On the blood agar plate, large gray, smooth, flat, mucoid, β-hemolytic
colonies were found. Although bacteria growing on solid media should not be
actively smelled, the organism emitted a grape or tortilla smell from the
plate. The organism was identified as Pseudomonas
aeruginosa by MALDI-TOF mass spectrometry. The isolate was plated onto Mueller
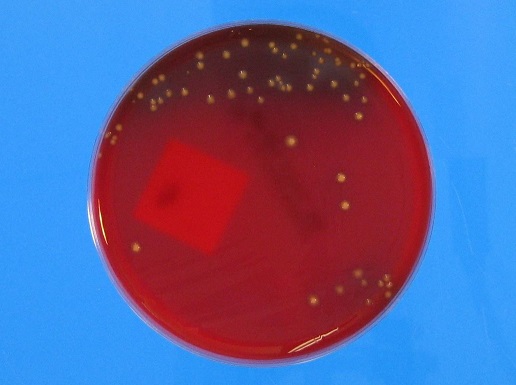
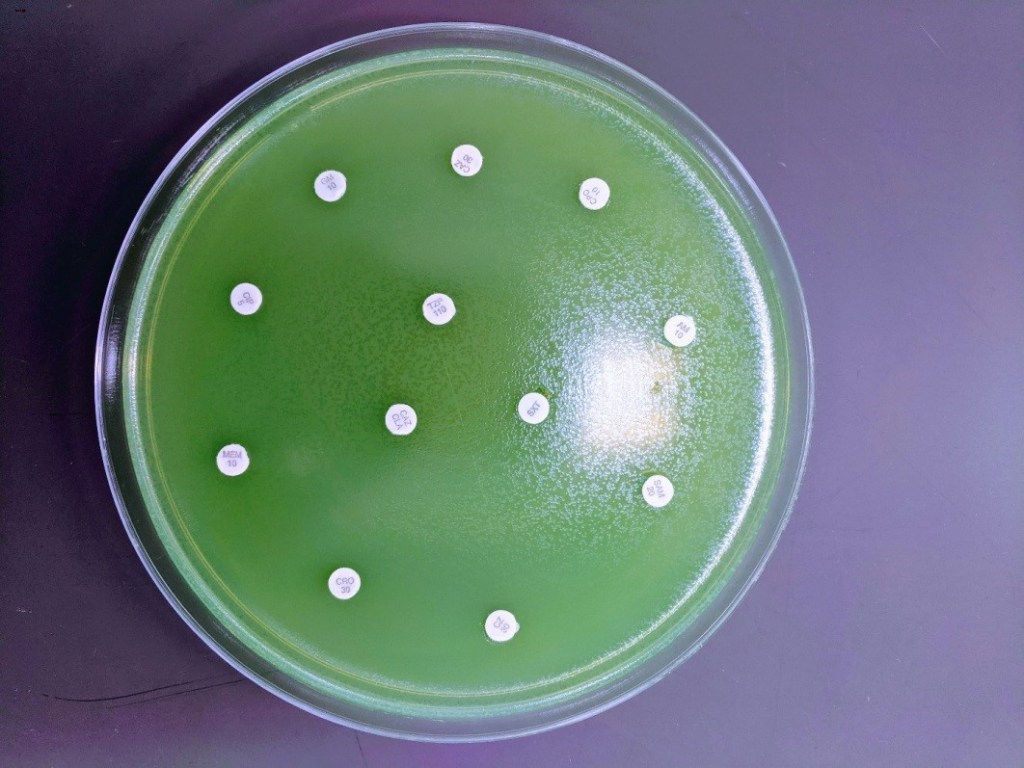
Hinton agar for Kirby-Bauer disc diffusion antibiotic susceptibility testing (Image 1). A fluorescent green lawn of bacteria
grew up to the edge of all discs, indicating high-level resistance to all
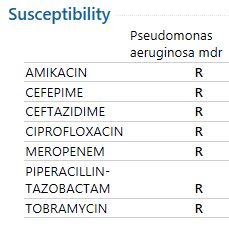
antibiotics tested (Table 1). Modified
carbapenem inactivation method (mCIM) testing was positive and Cepheid
GeneXpert CarbaR PCR testing revealed that this P. aeruginosa isolate carried the New Delhi metallo-β-lactamase-1
carbapenemase (NDM-1).
Image 1. Kirby-Bauer disc diffusion was used for antimicrobial susceptibility testing. Note no zones around any of the antibiotic discs, indicating resistance to all antimicrobials tested.
Table 1. Antimicrobial susceptibility testing interpretations. All drugs tested were resistant to this P. aeruginosa isolate.
Discussion
The issue of super bugs is on the rise, with the fear of
antibiotic resistance disseminating through more bacterial populations and
species. Carbapenems are drugs that are very powerful broad-spectrum
antibiotics, usually reserved as a last resort treatment for serious and
resistant infections.1 β-lactamases are divided into four Ambler
classes: A, B, C, and D. Class B differs from the others because it utilizes
zinc as a metal cofactor for its catalytic activity. The others use a serine
residue for their catalytic activity.2
NDM-1 is a class B β-lactamase. It was named after New Delhi, India when a Swedish resident presented with an extremely resistant infection after a trip to India in 2008. NDM-1 bacteria can now be found with high prevalence in India and China, and increasingly in other countries such as the UK and US.3,4 While the origination of the gene may not have been India, many of these infections are from people who have traveled to India or other Asian continents.5 Concerns about overprescribing and misuse of antibiotics in India are rising, where India is one of the biggest consumers of antibiotics in the world. One study even found striking evidence of this misuse, demonstrating that 2 out of 3 adults under 20 presented antibiotic resistance isolates to fluoroquinolones and/or cephalosporins.6,7,8
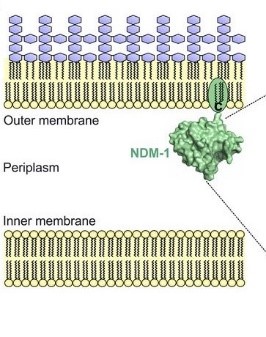
Image depicting the NDM-1 protein anchored in the outer membrane of the bacterium. (Taken from Bahr, Guillermo, et al. “Clinical Evolution of New Delhi Metallo-β-Lactamase (NDM) Optimizes Resistance under Zn(II) Deprivation.” Antimicrobial Agents and Chemotherapy, vol. 62, no. 1, 2017, doi:10.1128/aac.01849-17.)
The gene for NDM-1 is blaNDM-1 and has been found on both plasmid and chromosomal components of different bacteria. Due to its presence on plasmids, the gene can easily spread through bacterial populations and other bacterial species – as has already been documented in Enterobacteriaceae and A. baumannii.3 The β-lactamase that it codes for is a lipoprotein that is anchored in the outer membrane of the gram negative bacteria. Other metalo-β-lactamases (MBLs) are periplasmic proteins, which are more affected by changes in essential metal cofactors in their enzymatic function. Thus far, it has been found that there are 16 discovered variants of NDM. Some variants being more fit than NDM-1. It is hypothesized that these variants are being selected for in the clinical setting, with the protein being more stable and demonstrating higher affinities for zinc during time of metal-chelating (a process the immune system adapts to combat infections).9 Unfortunately, NDM-1 and its variants are resistant to almost all antibiotics. Usually the only option is colistin and tigecycline.3
The disturbing issue, and the big picture, is the capability
of MDR organisms and their genes of disseminating. As previously mentioned, NDM-1
is capable of spreading to other species and within its population. Yet, a
terrifying report has demonstrated blaNDM-1
detection in artic soil samples from 2013, 4 years after the first detection of
the gene.10 This demonstrates the ability for antibiotic resistance
to spread on a global scale, and how serious this battle truly is.
Walther-Rasmussen, Jan, and Niels Høiby.
“Class A Carbapenemases.” Journal of Antimicrobial Chemotherapy, vol. 60, no.
3, 2007, pp. 470–482., doi:10.1093/jac/dkm226.
Khan, Asad U., et al. “Structure, Genetics and
Worldwide Spread of New Delhi Metallo-β-Lactamase (NDM): a Threat to Public
Health.” BMC Microbiology, vol. 17, no. 1, 2017, doi:10.1186/s12866-017-1012-8.
Mohapatra P. R. (2013). Metallo-β-lactamase 1–why blame New
Delhi & India?. The Indian journal of medical research, 137(1),
213–215.
Gupta, M., Didwal, G., Bansal, S., Kaushal,
K., Batra, N., Gautam, V., & Ray, P. (2019). Antibiotic-resistant
Enterobacteriaceae in healthy gut flora: A report from north Indian semiurban
community. The Indian journal of medical research, 149(2), 276–280.
doi:10.4103/ijmr.IJMR_207_18
Kotwani, Anita, and Kathleen Holloway. “Access
to Antibiotics in New Delhi, India: Implications for Antibiotic Policy.”
Journal of Pharmaceutical Policy and Practice, vol. 6, no. 1, 2013,
doi:10.1186/2052-3211-6-6.
Kotwani, Anita, et al. “Antibiotic-Prescribing
Practices of Primary Care Prescribers for Acute Diarrhea in New Delhi, India.”
Value in Health, vol. 15, no. 1, 2012, doi:10.1016/j.jval.2011.11.008.
Bahr, Guillermo, et al. “Clinical Evolution of
New Delhi Metallo-β-Lactamase (NDM) Optimizes Resistance under Zn(II)
Deprivation.” Antimicrobial Agents and Chemotherapy, vol. 62, no. 1, 2017,
doi:10.1128/aac.01849-17.
Mccann, Clare M., et al. “Understanding Drivers
of Antibiotic Resistance Genes in High Arctic Soil Ecosystems.” Environment
International, vol. 125, 2019, pp. 497–504., doi:10.1016/j.envint.2019.01.034.
-Ben Dahlstrom is a recent graduate of the NorthShore University HealthSystem MLS program. He currently works as a molecular technologist for Northwestern University in their transplant lab, performing HLA typing on bone marrow and solid organ transplants. He graduated with a bachelors in Biology at the University of Illinois at Chicago (UIC) and concurrently from the UIC Honors College. He discovered his passion for the lab through his experience in healthcare. His interests include microbiology, molecular, immunology, and blood bank.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.