Researchers from the Walter Reed National Military Medical Center in Maryland discovered a strain of E. coli that carried 15 different genes that confer antibiotic resistance, including the resistance factor MCR, which confers resistance to colistin, a drug of last resort.
This particular E. coli was recovered from the urine of a 49-year-old woman.
The weak D (formerly Du) phenotype describes an individual with a variant RHD allele, leading to low expression of complete D antigen on the surface of their red blood cells. The partial D phenotype describes a variant RHD allele that results in modification of the surface D antigen and can result in the loss of D epitope. The prevalence of these phenotypes is thought to occur in 0.2 to 1% of Caucasians. Typically, alloimmunization with anti-D is more likely to occur in partial D individuals who are exposed to the Rh(D) antigen than in weak D individuals. However, there are instances when weak D individuals may develop an anti-D alloantibody after exposure to Rh(D) positive blood. Since the most common methods of immunohematology testing in the Blood Bank cannot reliably discern between weak D and partial D expression, a standard practice is treat both weak D and partial D individuals as Rh(D) negative when they are recipients of blood products.
The AABB Standards for Blood Banks and Transfusion Services does not require that weak D testing be performed on Rh(D)-negative recipients of blood products. In line with this, our transfusion service does not routinely perform serologic weak D testing on transfusion recipients and our testing algorithm is designed to consider weak D and partial D individuals as Rh(D) negative for transfusion purposes. We believe our testing strategy helps prevent anti-D alloimmunization in a vulnerable population, especially women of childbearing potential, and helps streamline test utilization in the Blood Bank. That said, we continue to perform weak D testing on potential red blood cell donors (i.e. fetus and newborn of Rh(D) negative mother, stem cell and solid organ donors).
Rh typing discrepancies may occur in the following situations:
Obstetric patients: A patient typed as weak Rh(D) positive during her prior pregnancy and did not receive Rh immune globulin prophylaxis (RhIg). However, during the current pregnancy, this patient is now typed as Rh(D) negative due to our updated procedure. If the newborn is Rh(D) positive, a fetal screen and Kleihauer-Betke test will be performed as needed, and an appropriate RhIg dose is recommended.
Previous blood donors, organ donors, and cord blood from neonates: It is important to identify the weak D phenotype in blood donors (including cord blood from neonates) since very low levels of D antigen are sufficient to elicit the formation of an anti-D alloantibody in Rh(D) negative transfusion recipients. A patient who was previously a blood donor would be typed by the blood collection center as Rh(D) positive due to the presence of weak D, but as a transfusion recipient would be typed as Rh(D) negative since weak D testing is not performed on transfusion recipients.
-Thomas S. Rogers, DO is a second-year resident at the University of Vermont Medical Center, a clinical instructor at the University of Vermont College of Medicine, and the assistant medical director of the Blood Bank and Transfusion Medicine service.
A 25 year old male presents to the Emergency Department with a right sided sore throat for the past 3 days which radiates to the right ear. Upon arrival, he was experiencing spasms in his jaw muscles and was unable to open his mouth fully. His past medical history is significant for recurrent peritonsillar abscesses (x5) and sexually transmitted infections (N. gonorrhea and C. trachomatis). He is a current smoker and is sexually active with male partners. Review of systems shows a 10/10 sharp, right sided throat pain, difficulty swallowing, ear pain and shortness of breath. He denies fever, chills, rhinorrhea, neck pain, voice changes and cough. He is currently afebrile and all vitals are within normal limits. His right tonsil is swollen and erythematous, though no petechiae or exudates are seen. His uvula is midline and there is no drooling or “hot potato” voice. Tender cervical lymphadenopathy is present. A rapid strep and HIV testing are negative. A neck CT scan demonstrates a 2.2 cm peritonsillar abscess. An incision and drainage is performed by ENT. Three milliliters of purulent fluid was collected and sent to the Microbiology laboratory for Gram stain and bacterial culture.
Laboratory identification:
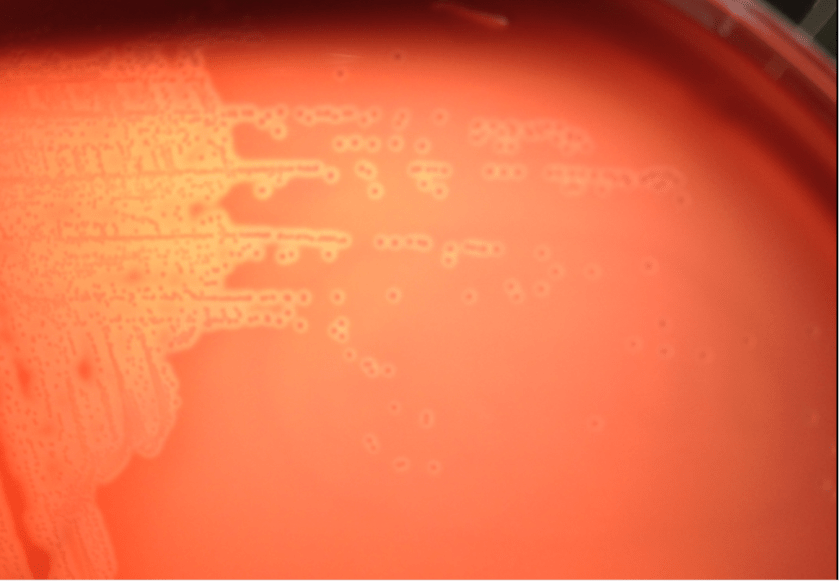
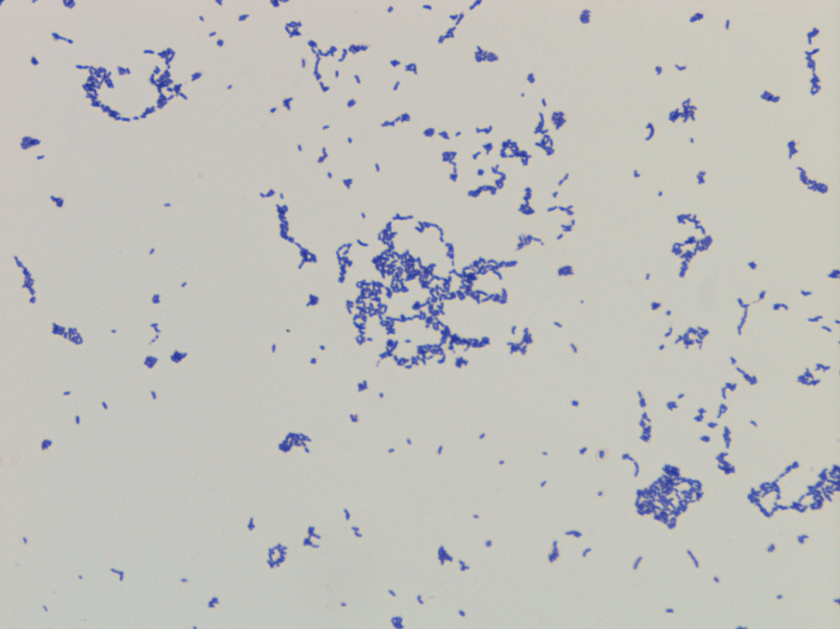
Bacterial culture of the purulent fluid grew small, beta hemolytic colonies after 48 hours of incubation at 35°C. A Gram stain of the colonies showed small Gram positive rods. Biochemical reactions were negative for both catalase and PYR. Arcanobacterium haemolyticum was identified by MALDI-TOF and confirmed with an API Coryne strip. The Streptococcus DNA probe, which is performed on all negative rapid strep results, was also appropriately negative.
Figure 1. Growth of small, dull colonies with a relatively narrow zone of beta-hemolysis on sheep blood agar after 48 hours in a CO2 incubator at 35°C.Figure 2. Gram stain of the isolate from bacterial culture showing small Gram positive bacilli (100x oil immersion).
Discussion:
Arcanobacterium haemolyticum is a facultative Gram positive bacillus, formerly known as Corynebacterium haemolyticum, which was first characterized in 1946 after being isolated from U.S. service members serving in the South Pacific who developed pharyngitis and a skin rash. A. haemolyticum is most commonly implicated in acute pharyngitis in humans where it is accompanied by cervical lymphadenopathy, tonsillitis, and a rash on the extremities and truck that may be confused with the rash of scarlet fever in 20-25% of cases. The infection usually occurs in patients between 15 and 30 years old. Other infections in which A. haemolyticum has also been implicated include wound & soft-tissue infections, sinusitis, and rarely in cases of osteomyelitis, endocarditis, and meningitis.
A. haemolyticum can be recovered in the clinical laboratory, but it may be missed on throat culture specimens if they are not held for 48 hours or the subtle hemolysis in the first or second quadrants of the culture plate is not observed after overnight incubation. It can also be easily misclassified as non-group A streptococcal species unless close attention is paid to the Gram stain and biochemical test results. Similar to Group A Streptococcus, A. haemolyticum is catalase negative. However, on examination of the Gram stain, A. haemolyticum is a Gram positive rod and the PYR reaction is negative whereas the Gram stain of Streptococcus pyogenes is Gram positive cocci arranged in pairs and chains and PYR positive. Another helpful test in the identification of A. haemolyticum is that it is reverse CAMP test positive. This feature is exhibited due to the fact the phospholipase in A. haemolyticum inhibits the effect of the beta hemolysin of Staphylococcus aureus when they are arranged perpendicular to each other in streaks.
In general, A. haemolyticum is susceptible to penicillin, cephalosporins and vancomycin. Resistance to trimethoprim-sulfamethoxazole is common and rare cases of resistance to tetracyclines, macrolides, clindamycin and ciprofloxacin have been described. As for our patient, he was discharged home on a ten day course of Augmentin and scheduled for tonsillectomy due to his history of recurrent peritonsillar abscesses.
-David Marbury, MD, is a 2nd year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
A 47 year old male of Jamaican origin with no known past medical history presented to a clinic with abdominal pain and diarrhea. He has been working as a seasonal farmer and plans to return back to Jamaica by the end of the month. Stool samples were obtained and sent for culture and ova and parasite exam.
Rhabditiform larvae of Strongyloides stercoralis from the wet mount of O&P examBlood agar plate demonstrating tracks made by crawling larvae
Strongyloides stercoralis is the primary species of the Strongyloides genus that causes human disease. The larvae are small and can reach around 1.5mm in length. The primary mode of infection is through contact with soil that is contaminated with larvae. The larvae are able to penetrate the skin and migrate through the body to the small intestine where they burrow and lay their eggs. The eggs hatch into larvae in the intestine, unlike other helminths. Of these larvae, most will be eliminated in feces, but some may shed and immediately re-infect the host. This is achieved either by burrowing into the intestinal wall, or by penetrating the perianal skin. The process is called auto-infection, and if the patient is not treated, they may continue to be infected throughout their life.
Strongyloides is generally found in warm and moist areas, as well as areas associated with agricultural activity. The majority of people infected with Strongyloides are asymptomatic, and those who do develop symptoms have generalized symptoms such as abdominal pain, bloating and diarrhea.
The time of exposure is usually unknown, although a local rash can occur at exposure. People exposed to Strongyloides can also develop a cough several days post exposure. Abdominal symptoms usually occur about 2 weeks later, and larvae can be found in the stool after 3-4 weeks. Strongyloides is treated with ivermectin as a first-line drug. Thiabendazole can also be effective.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 60 year old patient with history of breast cancer presented with pancytopenia and bone marrow study was done to evaluate for metastatic tumor.
CBC revealed pancytopenia with a WBC count of 1.9 K/uL, macrocytic anemia (Hb 7.6 g/dl, MCV 106.2 fl) and decreased platelets at 15 K/uL.
Review of peripheral smear revealed circulating blasts.
Differential Count (100 cells):
13% Blasts
18% Neutrophils
69% Lymphocytes
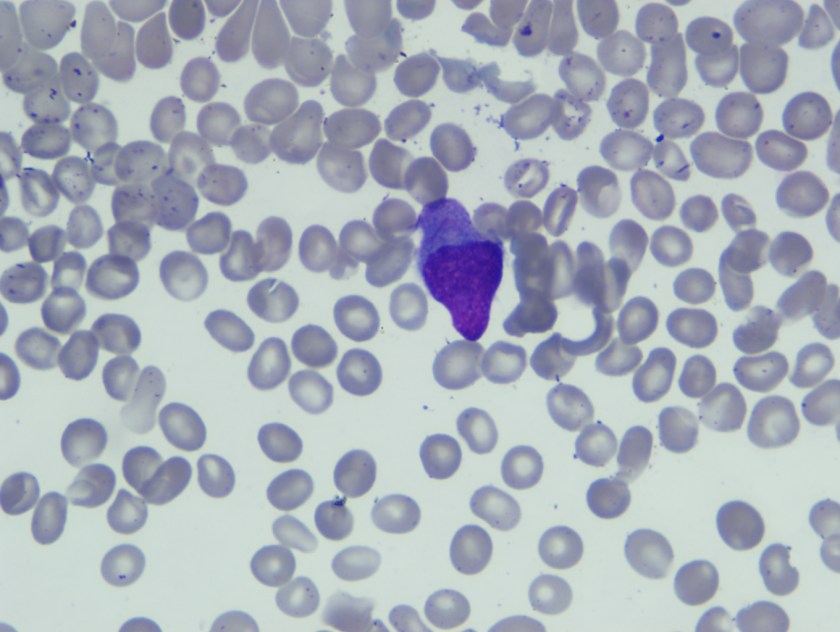
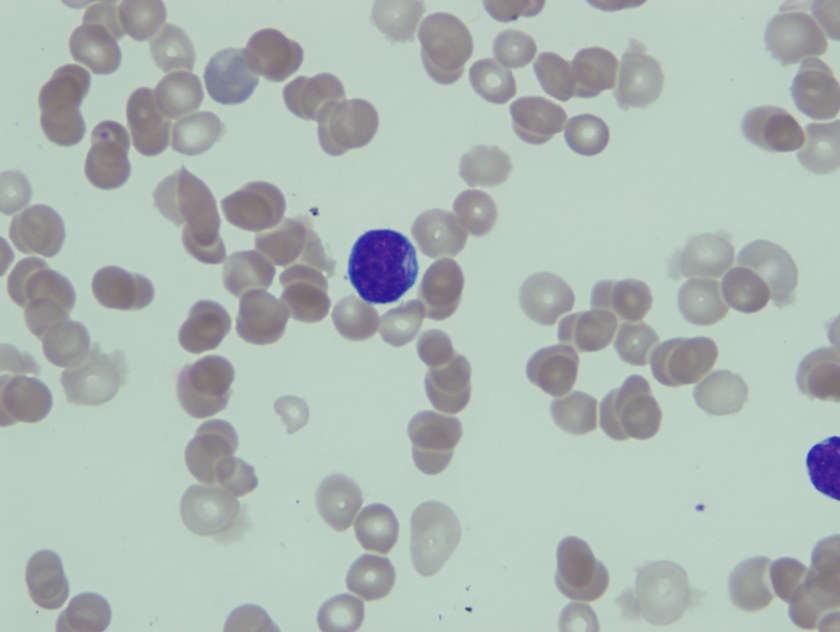
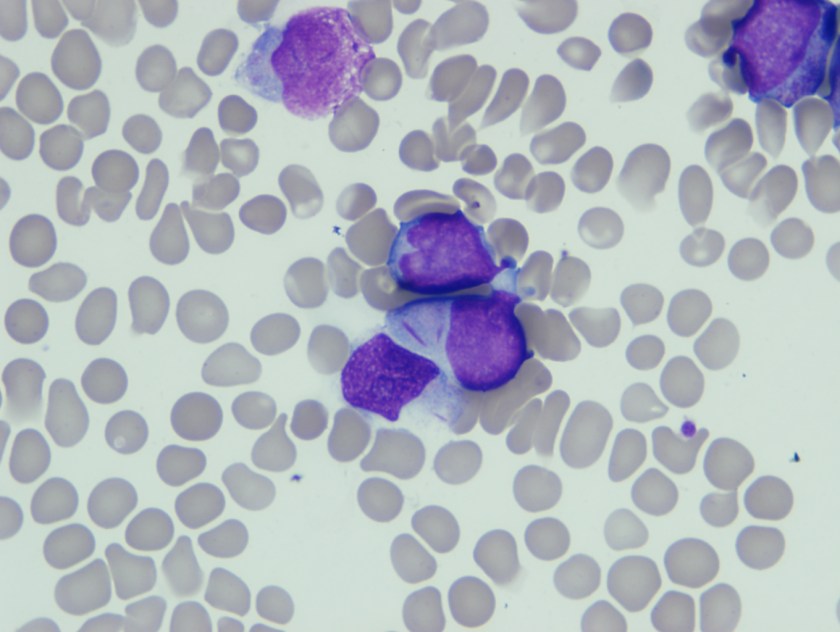
Blasts were intermediate in size with high N/C ratio, fine nuclear chromatin, 0-1 nucleoli, and scant basophilic cytoplasm. Few blasts have convoluted nuclei and in an occasional blasts slender Auer rod was seen.
Peripheral blood smear showing blast with slender Auer rodPeripheral blood smear showing blast with slender Auer rodBone marrow aspirate smear showing blasts with elongated Auer rods.
Based on this morphological finding FISH for t8;21) was ordered along with karytoype analysis.
Translocation (8;21) was detected by both karyotype and FISH analysis (50.5% cells).
nuc ish (RUNX1T1,RUNX1x3)(RUNX1T1 con RUNX1x2)[101/200]
nuc ish (MYC,IgH)x2[97/200]
Based on presence of complex karyotype and t(8;21) together with prior history of chemotherapy for breast carcinoma diagnosis of Therapy related AML with t(8;21) was made.
Discussion
Acute myeloid leukemia (AML) associated with the t(8;21)(q22;q22) represents approximately 5% to 12% of de novo AMLs. At the molecular genetic level, this neoplasm is defined by the presence of the t(8;21)(q22;q22) involving the AML1 (RUNX1) gene on chromosome 21q22.3 and the ETO (RUNX1T1) gene on chromosome 8q22. TheAML1–ETO (RUNX1–RUNX1T1) fusion product disrupts the core binding factor transcription complex, which affects cell differentiation, proliferation, apoptosis, and self-renewal and, thus, initiates leukemogenesis. Patients with de novo AML-t(8;21) have a high complete remission rate and relatively long disease-free survival, especially adults treated with high-dose cytarabine in the consolidation phase.
Therapy-related AML (t-AML) is a known complication of cytotoxic chemotherapy and radiation therapy, which are known to be mutagenic. Causative agents include alkylating agents and topoisomerase-II inhibitors and platinum drugs. The outcomes for patients with t-AML have been historically poor compared with those for patients with de novo AML. t-AML-t(8;21) is uncommon.
Blasts in t-AML and de novo AML associated with t(8;21)(q22;q22) share characteristic morphologic and immunophenotypic features, and affected patients have a comparable initial response to induction chemotherapy. Patients with t-AML-t(8;21), however, have been reported to have a shorter survival.
Therapy related AML with t(8;21) shares morphologic and immunophenotypic features with de novo AML-t(8;21).
Common morphological features include the presence of large blasts with abundant cytoplasm, often containing Auer rods which appear long and slender with tapered ends as was seen in our patient. Additional common morphological findings seen in AML with t(8;21) include presence of numerous azurophilic granules and perinuclear clearing or very large granules (pseudo-Chediak-Higashi), suggesting abnormal fusion.
Both de novo AML with t(8;21) and therapy related AML with t(8;21) are characterized by the AML1–ETO (RUNX1–RUNX1T1) fusion. However, AML1–ETO fusion in t-AML does not predict a favorable outcome in the therapy-related setting. Patients with t-AML-t(8;21) usually have a higher frequency of KIT mutations, which is an adverse prognostic indicator.
-Neerja Vajpayee, MD, is an Associate Professor of Pathology at the SUNY Upstate Medical University, Syracuse, NY. She enjoys teaching hematology to residents, fellows and laboratory technologists.
In their most recent Morbidity and Mortality Weekly Report (MMWR), the CDC issued interim guidance for Zika Virus testing. From the report:
“On the basis of the newly available data, CDC recommends that Zika virus rRT-PCR be performed on urine collected <14 days after onset of symptoms in patients with suspected Zika virus disease. Zika virus rRT-PCR testing of urine should be performed in conjunction with serum testing if using specimens collected <7 days after symptom onset. A positive result in either specimen type provides evidence of Zika virus infection.”
In March of 2016, the United States Government Accountability Office (an independent agency that works for Congress) produced a report stating that stronger oversight mechanisms are needed to improve safety in high-containment laboratories. The laboratories referred to are those which work with hazardous biological agents in order to protect public and animal health and the food supply against contamination of those agents. Because of several very public lab safety lapses in the past two years, the report makes 33 recommendations to improve lab safety. These recommendations include the development and update of policies that contain missing safety elements, the reporting of oversight activity to senior officials, and the development of plans with time frames to implement the safety recommendations. The report basically recommends a “Safety Stand Down.” Has your laboratory seen a similar situation? Have you encountered a series of like safety events that created the need to stop and review?
OSHA’s definition of a safety stand down is “an event for employers to talk directly to employees about safety.” Because of the danger to employees, a more specific definition means that all work stops until the issue is corrected and all affected (or potentially affected) staff has been educated to make sure the issue does not re-occur. However, in the real world, unless someone is in imminent danger, the work of the laboratory must go on for the sake of patient care. Still, a stand down can be important, and there are ways to run one successfully.
Once you have decided there is a need for the stand-down, develop the stand-down education. This can include a set of presentation slides, a hand-out, or talking points to use as the information is delivered. Make sure you stick to the topic(s) at hand, and do not include extraneous information, but be certain to include all items that are pertinent to the stand-down subject.
The next step is deciding on the stand-down delivery approach. Will you meet with staff one-on one, in small groups, or with everyone at the same time? Choose the meeting location(s) and schedule the meetings. Because this is a stand-down and a safety issue that must be dealt with, these steps should occur quickly. If you are facilitating the stand-down but not delivering it personally, be sure to give a short deadline for its completion and mandate that all involved personnel are included. Keep documentation of attendance and subject matter for future reference.
Once the stand-down is completed, gather the documentation of attendance and any other associated information and keep it for your records. This does not end the stand-down, however. Make a plan and a schedule to follow-up on the safety issue. The plan may include daily or weekly checks to ensure new processes are being followed or that staff has understood the information completely.
Conducting a laboratory safety stand-down can seem difficult and time-consuming. It may interrupt the work you planned to do, and it may change your schedule for the next couple of days or weeks. While that may be inconvenient, remember that this course of action was chosen to help prevent harm to employees or patients, and that is what laboratory professionals are here to do.
During the week of May 2, 2016, OSHA called for a construction fall prevention safety stand-down. This was in response to a high number of preventable worker deaths due to falls on the job. What safety issues have you seen in your lab? Have you seen multiple needle sticks? What about slips, trips, and falls? If you notice a group of similar safety events, it may be time to conduct a safety stand-down. If you deliver the information, provide the education, and document the attendance of all affected staff, you will prevent further injury and continue to raise awareness in the lab of vital safety issues.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A 26 year-old G1P0A0 female at 35 weeks 2 days twin gestation presented with contractions and was found to have oligohydramnios and decelerations of both twins. She reported a subjective fever two days prior and the morning of admission, associated with a mild frontal headache, both of which resolved prior to presentation. At the time of admission she was afebrile, however pancytopenic with WBC 4.17 x 109/L, platelets 105 x 109/L of and hemoglobin 7 g/dL with laboratory evidence of hemolysis; haptoglobin <5 mg/dL, reticulocyte 143 x 109/L (6.5%), lactate dehydrogenase 460 units/L and total bilirubin 2.4 mg/dL. Upon further questioning, the patient reported that she recently emigrated from Central Africa where she was found to be anemic and treated for malaria approximately one month prior to presentation. She reported taking oral medication with no follow-up. A malaria workup, including thick and thin smears (Figure 1), was initiated for the patient and her newborn twins after a successful urgent Caesarian section. The placenta was submitted for standard histopathology (Figure 2) according to protocol due to pre-term birth, multiple gestation and fetal distress.
Figure 1. Compilation of several images of Wright Geimsa-stained thin smears of the patient’s peripheral blood, showing numerous and often multiple intra-cellular delicate ring forms, including appliqué forms. Occasional extra-cellular forms were also identified.Figure 2. Wright Geimsa stain of a thick smear showing numerous aggregated ring forms.Figure 3. Hematoxilin and eosin (H&E) stain of formalin-fixed paraffin embedded (FFPE) placental tissue, showing A. intervillous macrophages and hemazoin and B. infected red blood cells (RBCs) in the intervillous (maternal) spaces containing ring forms, sometimes appearing as black, refractile dots (inset).
Peripheral blood findings
Geimsa-stained thin smears of the patient’s peripheral blood showed numerous infected RBCs and several individual RBCs infected with multiple trophozoites (ring forms). Occasional extra-cellular ring forms were also identified. The rings were small (<1/3 size of RBC) and delicate with 1 or sometimes 2 chromatin dots that give the appearance of headphones. Some of the ring forms were marginalized at the RBC membrane; the so-called appliqué, accollé or marginal forms. Gametocytes were not identified. Parasitemia was calculated to be 10% prior to initiation of treatment. Thick smears showed numerous aggregated ring forms. These features are consistent with Plasmosdium falciparum.
Placenta findings
H&E stained sections of FFPE placental tissue, showed focally increased intervillous macrophages associated with mild perivillous fibrin deposits. Malaria pigment (hemazoin) was scattered throughout the specimen; both intracellular pigment within macrophages and extracellular pigment entrapped in fibrin deposits and in the cytoplasm of trophoblasts was identified. Infected red blood cells, containing ring forms, were only identified in the intervillous (maternal) spaces, sometimes appearing as black, refractile dots (inset).
P. falciparum is a blood parasite transmitted by female Anopheles mosquitos found in the tropics and subtropics worldwide with the highest transmission rates in Sub-Saharan Africa and parts of Oceania. Sporozoites are injected into the bloodstream during a blood meal and travel to the liver to proliferate during the exo-erythrocytic cycle. Schizonts mature in hepatocytes and then rupture releasing merozoites into the blood. Unlike P. ovale and P. vivax, P. falciparum does not have a dormant liver stage (hypnozoites). The erythrocytic cycle begins when merozoites infect RBCs at any stage and undergo asexual multiplication (erythrocyte schizogony) producing ring forms (trophozoites) that mature into schizonts which eventually rupture and release more merozoites into the blood. Some trophozoites mature into gametocytes that can undergo sexual (sporogonic) lifecyles within the mosquito vector when consumed by a female Anopheles mosquito. Banana shaped gametocytes can be found in the peripheral blood in late P. falciparum infection. Stages other than trophozoites and gametocytes are rarely found in peripheral blood during P. falciparum infection due to sequestration in the capillaries and venules of organs.
The diagnosis of malaria is typically made by morphologic examination of 2-3 thick and thin smears over a 24 hour period. Exclusion of malaria can only be made after examination of at least 100 oil immersion fields on thick smears or 300 fields on thin smears to achieve a sensitivity of 5 parasites/μL. Flow cytometric, rapid diagnostic antigen, serologic and molecular (PCR) methods have also been developed, however are not widely available, particularly in endemic areas. The degree of parasitemia (percent infected red cells) is an important prognostic factor in P. falciparum infection, with >2% parasitemia considered severe.
Clinical symptoms are associated with asexual erythrocytic schizgony and include “malaria attacks” consisting of a cold stage (shivering), a hot stage (fevers, headaches, vomiting and seizures in children) and a sweating stage (with malaise and body aches following). These attacks classically occur every 2nd day (48 hours) in P.falciparum infection, which is a “tertian” parasite. Severe malaria and mortality is associated with complications such as cerebral malaria, severe hemolytic anemia, adult respiratory distress syndrome, coagulopathy and organ failure. Adults living in areas of stable transmission that have been infected with malaria multiple times may acquire partially immunity.
Pregnant women and children are particularly susceptible to malaria due to altered and immature immunity respectively. Pregnancy can also reduce previously acquired anti-malarial immunity. The placenta sequesters parasites contributing to severe maternal anemia, intrauterine growth retardation, intra-uterine fetal demise, premature delivery and neonatal death. The severity of complications of malaria during pregnancy increases in HIV infected women and primi-gravidae, however increased severity can extend to second and third gravidae in low transmission areas. In endemic areas where women have acquired anti-malarial immunity, severe maternal anemia may be the only symptom of P.falciparum infection during pregnancy. In some cases, parasitemia may not be detected despite placental infection. Some of the histologic features of placental malaria are described above. Several classification systems have been proposed and generally categorize placental infection (i.e. active, active-chronic, past-chronic) based on the degree of placental changes; namely presence of perivillous fibrin deposits, intervillous macrophages and fibrinoid necrosis of chorionic villi, location of hemazoin pigment, cytotrophoblast proliferation, thickening of trophoblastic basement membranes and identification of infected RBCs. Although placental malaria is a prerequisite for congenital malaria, the frequency of vertical transmission is relatively low, with a ranges reported from 0-25%. Lower transmission risk has been attributed to passive immunization of maternal antibodies and conversely higher transmission risk is associated with non-immunity of mothers.
Discussion
It is suspected, due to high parasitemia with seemingly mild symptoms, that the patient presented above had acquired partial immunity to malaria. In addition, she likely experienced Malarone (Atovaquone-proguanil) failure after initial treatment prior to emigration. She responded well to oral Coartem (artemether-lumefantrine) with non-detectable parasitemia after the third day of treatment. Both infants’ thick and thin smears were negative for parasites.
References
Bulmer JN, Rasheed FN, Morrison L, Francis N, Greenwood BM. Placental malaria. I. Pathological classification. Histopathology. 1993;22:211–218.
Bulmer JN, Rasheed FN, Morrison L, Francis N, Greenwood BM. Placental malaria. II. A semi-quantitative investigation of the pathological features. Histopathology. 1993;22:219–226.
Newman RD, Robalo M, Quakyi I. Malaria during pregnancy: epidemiology, current prevention strategies, and future directions. Emerg Infect Dis [serial on the Internet]. 2004 November [March 7, 2016]. http://dx.doi.org/10.3201/eid1011.040624_09
Uneke CJ. Impact of Placental Plasmodium falciparum Malaria on Pregnancy and Perinatal Outcome in Sub-Saharan Africa: I: Introduction to Placental Malaria. The Yale Journal of Biology and Medicine. 2007;80(2):39-50.
Uneke CJ. Impact of Placental Plasmodium falciparum Malaria on Pregnancy and Perinatal Outcome in Sub-Saharan Africa: II: Effects of Placental Malaria on Perinatal Outcome; Malaria and HIV. The Yale Journal of Biology and Medicine. 2007;80(3):95-103.
Uneke CJ. Impact of Placental Plasmodium falciparum Malaria on Pregnancy and Perinatal Outcome in Sub-Saharan Africa: Part III: Placental Malaria, Maternal Health, and Public Health. The Yale Journal of Biology and Medicine. 2008;81(1):1-7.
-Petra Rahaman, M.D., 4th year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
“The test was developed by the reference laboratory business of Quest’s Focus Diagnostics, Inc., subsidiary. The proprietary molecular test is intended for the qualitative detection of RNA from the Zika virus in human serum specimens from certain individuals. Quest Diagnostics plans to make the new test broadly available to physicians for patient testing, including in Puerto Rico, early in the week of May 2.
“Zika Virus RNA Qualitative Real-Time RT-PCR test is a real-time RT-PCR test intended only for the qualitative detection of RNA from the Zika virus in human serum specimens from patients meeting Centers for Disease Control and Prevention (CDC) Zika virus clinical criteria (e.g., clinical signs and symptoms associated with Zika virus infection) and/or CDC Zika virus epidemiological criteria (e.g., history of residence in or travel to a geographic region with active Zika transmission at the time of travel, or other epidemiologic criteria for which Zika virus testing may be indicated ). Testing is limited to qualified laboratories designated by Focus Diagnostics, Inc.
“This test is intended for use by trained clinical laboratory personnel qualified by state and federal regulations who have received specific training on the use of the test in qualified laboratories designated by Focus Diagnostics, Inc., and, in the United States, certified under CLIA to perform high complexity tests.”