A 51 year old patient presented to the emergency room with abdominal pain and fever. Fever was associated with diaphoresis, chills and headaches. Patient was in Tanzania for 3 months. She was admitted to the hospital while she was there for some unknown infection, details of which are not available.
CBC done revealed normocytic normochromic anemia with a hemoglobin of 9.2 g/dl and thrombocytopenia. Platelet count was 100 K/uL. On review of peripheral blood revealed presence of malarial parasite (ring forms).
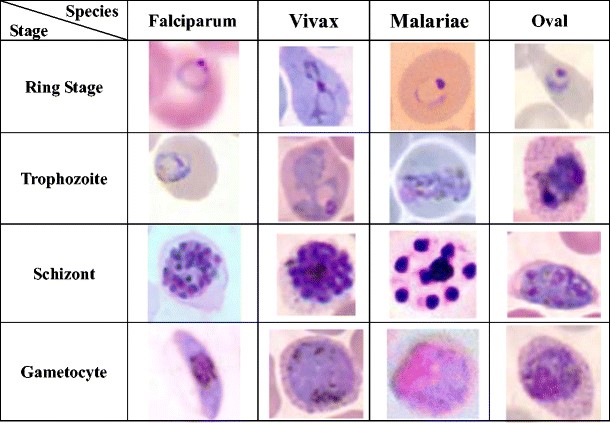
Malaria is an infectious disease caused by Plasmodium parasites. These parasites are primarily spread by the bite of infected female Anopheles mosquitos. There are four main types of Plasmodium (P) species that infect humans:
Plasmodium vivax and Plasmodium ovale, which cause a relapsing form of the disease, and
Plasmodium malariae and Plasmodium falciparum, which do not cause relapses.
Malaria must be recognized promptly in order to treat the patient in time.
Microscopy (morphologic analysis) continues to be the “gold standard” for malaria diagnosis. Parasites may be visualized on both thick and thin blood smears stained with Giemsa, Wright, or Wright-Giemsa stains. Giemsa is the preferred stain, as it allows for detection of certain morphologic features (e.g. Schüffner’s dots, Maurer’s clefts, etc.) that may not be seen with the other two. Ideally, the thick smears are used to detect the presence of parasites while the thin smears are used for species-level identification. Quantification may be done on both thick and thin smears.
Various antigen kits are available to detect antigens derived from malarial parasites. These rapid diagnostic tests (RDT) offer a useful alternative to microscopy in situations where reliable microscopic diagnosis is not available.
-Neerja Vajpayee, MD, is the director of Clinical Pathology at Oneida Health Center in Oneida, New York and is actively involved in signing out surgical pathology and cytology cases in a community setting. Previously, she was on the faculty at SUNY Upstate for several years ( 2002-2016) where she was involved in diagnostic work and medical student/resident teaching.
A 26 year-old G1P0A0 female at 35 weeks 2 days twin gestation presented with contractions and was found to have oligohydramnios and decelerations of both twins. She reported a subjective fever two days prior and the morning of admission, associated with a mild frontal headache, both of which resolved prior to presentation. At the time of admission she was afebrile, however pancytopenic with WBC 4.17 x 109/L, platelets 105 x 109/L of and hemoglobin 7 g/dL with laboratory evidence of hemolysis; haptoglobin <5 mg/dL, reticulocyte 143 x 109/L (6.5%), lactate dehydrogenase 460 units/L and total bilirubin 2.4 mg/dL. Upon further questioning, the patient reported that she recently emigrated from Central Africa where she was found to be anemic and treated for malaria approximately one month prior to presentation. She reported taking oral medication with no follow-up. A malaria workup, including thick and thin smears (Figure 1), was initiated for the patient and her newborn twins after a successful urgent Caesarian section. The placenta was submitted for standard histopathology (Figure 2) according to protocol due to pre-term birth, multiple gestation and fetal distress.
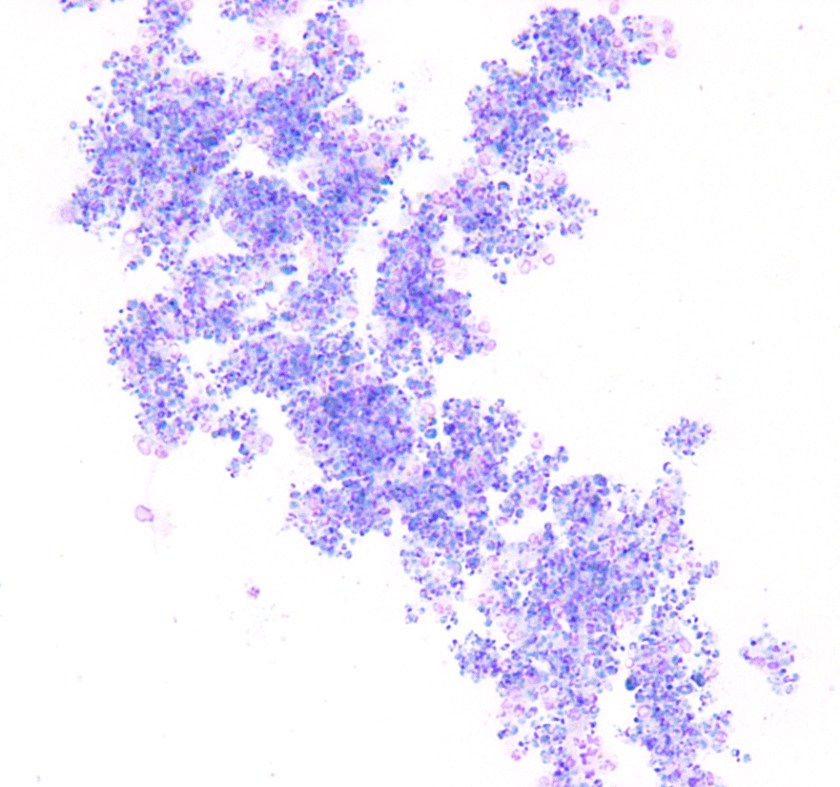
Figure 1. Compilation of several images of Wright Geimsa-stained thin smears of the patient’s peripheral blood, showing numerous and often multiple intra-cellular delicate ring forms, including appliqué forms. Occasional extra-cellular forms were also identified.Figure 2. Wright Geimsa stain of a thick smear showing numerous aggregated ring forms.Figure 3. Hematoxilin and eosin (H&E) stain of formalin-fixed paraffin embedded (FFPE) placental tissue, showing A. intervillous macrophages and hemazoin and B. infected red blood cells (RBCs) in the intervillous (maternal) spaces containing ring forms, sometimes appearing as black, refractile dots (inset).
Peripheral blood findings
Geimsa-stained thin smears of the patient’s peripheral blood showed numerous infected RBCs and several individual RBCs infected with multiple trophozoites (ring forms). Occasional extra-cellular ring forms were also identified. The rings were small (<1/3 size of RBC) and delicate with 1 or sometimes 2 chromatin dots that give the appearance of headphones. Some of the ring forms were marginalized at the RBC membrane; the so-called appliqué, accollé or marginal forms. Gametocytes were not identified. Parasitemia was calculated to be 10% prior to initiation of treatment. Thick smears showed numerous aggregated ring forms. These features are consistent with Plasmosdium falciparum.
Placenta findings
H&E stained sections of FFPE placental tissue, showed focally increased intervillous macrophages associated with mild perivillous fibrin deposits. Malaria pigment (hemazoin) was scattered throughout the specimen; both intracellular pigment within macrophages and extracellular pigment entrapped in fibrin deposits and in the cytoplasm of trophoblasts was identified. Infected red blood cells, containing ring forms, were only identified in the intervillous (maternal) spaces, sometimes appearing as black, refractile dots (inset).
P. falciparum is a blood parasite transmitted by female Anopheles mosquitos found in the tropics and subtropics worldwide with the highest transmission rates in Sub-Saharan Africa and parts of Oceania. Sporozoites are injected into the bloodstream during a blood meal and travel to the liver to proliferate during the exo-erythrocytic cycle. Schizonts mature in hepatocytes and then rupture releasing merozoites into the blood. Unlike P. ovale and P. vivax, P. falciparum does not have a dormant liver stage (hypnozoites). The erythrocytic cycle begins when merozoites infect RBCs at any stage and undergo asexual multiplication (erythrocyte schizogony) producing ring forms (trophozoites) that mature into schizonts which eventually rupture and release more merozoites into the blood. Some trophozoites mature into gametocytes that can undergo sexual (sporogonic) lifecyles within the mosquito vector when consumed by a female Anopheles mosquito. Banana shaped gametocytes can be found in the peripheral blood in late P. falciparum infection. Stages other than trophozoites and gametocytes are rarely found in peripheral blood during P. falciparum infection due to sequestration in the capillaries and venules of organs.
The diagnosis of malaria is typically made by morphologic examination of 2-3 thick and thin smears over a 24 hour period. Exclusion of malaria can only be made after examination of at least 100 oil immersion fields on thick smears or 300 fields on thin smears to achieve a sensitivity of 5 parasites/μL. Flow cytometric, rapid diagnostic antigen, serologic and molecular (PCR) methods have also been developed, however are not widely available, particularly in endemic areas. The degree of parasitemia (percent infected red cells) is an important prognostic factor in P. falciparum infection, with >2% parasitemia considered severe.
Clinical symptoms are associated with asexual erythrocytic schizgony and include “malaria attacks” consisting of a cold stage (shivering), a hot stage (fevers, headaches, vomiting and seizures in children) and a sweating stage (with malaise and body aches following). These attacks classically occur every 2nd day (48 hours) in P.falciparum infection, which is a “tertian” parasite. Severe malaria and mortality is associated with complications such as cerebral malaria, severe hemolytic anemia, adult respiratory distress syndrome, coagulopathy and organ failure. Adults living in areas of stable transmission that have been infected with malaria multiple times may acquire partially immunity.
Pregnant women and children are particularly susceptible to malaria due to altered and immature immunity respectively. Pregnancy can also reduce previously acquired anti-malarial immunity. The placenta sequesters parasites contributing to severe maternal anemia, intrauterine growth retardation, intra-uterine fetal demise, premature delivery and neonatal death. The severity of complications of malaria during pregnancy increases in HIV infected women and primi-gravidae, however increased severity can extend to second and third gravidae in low transmission areas. In endemic areas where women have acquired anti-malarial immunity, severe maternal anemia may be the only symptom of P.falciparum infection during pregnancy. In some cases, parasitemia may not be detected despite placental infection. Some of the histologic features of placental malaria are described above. Several classification systems have been proposed and generally categorize placental infection (i.e. active, active-chronic, past-chronic) based on the degree of placental changes; namely presence of perivillous fibrin deposits, intervillous macrophages and fibrinoid necrosis of chorionic villi, location of hemazoin pigment, cytotrophoblast proliferation, thickening of trophoblastic basement membranes and identification of infected RBCs. Although placental malaria is a prerequisite for congenital malaria, the frequency of vertical transmission is relatively low, with a ranges reported from 0-25%. Lower transmission risk has been attributed to passive immunization of maternal antibodies and conversely higher transmission risk is associated with non-immunity of mothers.
Discussion
It is suspected, due to high parasitemia with seemingly mild symptoms, that the patient presented above had acquired partial immunity to malaria. In addition, she likely experienced Malarone (Atovaquone-proguanil) failure after initial treatment prior to emigration. She responded well to oral Coartem (artemether-lumefantrine) with non-detectable parasitemia after the third day of treatment. Both infants’ thick and thin smears were negative for parasites.
References
Bulmer JN, Rasheed FN, Morrison L, Francis N, Greenwood BM. Placental malaria. I. Pathological classification. Histopathology. 1993;22:211–218.
Bulmer JN, Rasheed FN, Morrison L, Francis N, Greenwood BM. Placental malaria. II. A semi-quantitative investigation of the pathological features. Histopathology. 1993;22:219–226.
Newman RD, Robalo M, Quakyi I. Malaria during pregnancy: epidemiology, current prevention strategies, and future directions. Emerg Infect Dis [serial on the Internet]. 2004 November [March 7, 2016]. http://dx.doi.org/10.3201/eid1011.040624_09
Uneke CJ. Impact of Placental Plasmodium falciparum Malaria on Pregnancy and Perinatal Outcome in Sub-Saharan Africa: I: Introduction to Placental Malaria. The Yale Journal of Biology and Medicine. 2007;80(2):39-50.
Uneke CJ. Impact of Placental Plasmodium falciparum Malaria on Pregnancy and Perinatal Outcome in Sub-Saharan Africa: II: Effects of Placental Malaria on Perinatal Outcome; Malaria and HIV. The Yale Journal of Biology and Medicine. 2007;80(3):95-103.
Uneke CJ. Impact of Placental Plasmodium falciparum Malaria on Pregnancy and Perinatal Outcome in Sub-Saharan Africa: Part III: Placental Malaria, Maternal Health, and Public Health. The Yale Journal of Biology and Medicine. 2008;81(1):1-7.
-Petra Rahaman, M.D., 4th year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
In recent months it seems that the only news stories about sub-Saharan Africa presented by western media are about Ebola. There are some bright spots in that news, but in general it is scary and saddening. Lost in the Ebola shuffle, however, is some good news about the fight against malaria. A recently released report from the WHO Global Malaria Programme states that worldwide the malarial mortality rate fell by 47% between 2000 and 2013 and currently 55 countries are on track to reduce their malarial burden by 75% by 2015. Those are exciting numbers. The report attributes these improvements to increased use of insecticide treated bed nets, accurate diagnostic testing, and increasingly effective drug therapies.
Accurate diagnostic testing means that the lab is playing a crucial role in the fight against malaria. Data from 2013 shows an increase in the use of diagnostic tests in sub-Saharan Africa. This supports additional data that shows there has been a shift from presumptive treatment to diagnostic treatment.
As a public health community, however, we cannot become complacent. The WHO report states that, in Africa, over 43,000 children die from malaria each year, 15 million pregnant women do not have access to preventative treatment, and over 200 million people live in households without access to insecticide treated bed nets. Drug and insecticide resistance is a serious concern (thus underscoring the importance of accurate diagnostic testing to prevent presumptive treatment that can contribute to drug resistance). In the West African countries hit by the Ebola outbreak, health care resources have all been directed towards the fight against Ebola leaving them vulnerable to increases in other disease occurrence. If nothing else, however, the Ebola outbreak has provided a reason and impetus for discussions surrounding the importance of health systems strengthening. Strengthening that will not only fight future outbreaks of diseases such as Ebola, but will improve health care networks for every day care and treatment.
Thus, in the spirit of the holidays, let’s celebrate this good news. But while doing so, let’s also continue the fight and keep up the good work.