Case:
A 25 year old male presents to the Emergency Department with a right sided sore throat for the past 3 days which radiates to the right ear. Upon arrival, he was experiencing spasms in his jaw muscles and was unable to open his mouth fully. His past medical history is significant for recurrent peritonsillar abscesses (x5) and sexually transmitted infections (N. gonorrhea and C. trachomatis). He is a current smoker and is sexually active with male partners. Review of systems shows a 10/10 sharp, right sided throat pain, difficulty swallowing, ear pain and shortness of breath. He denies fever, chills, rhinorrhea, neck pain, voice changes and cough. He is currently afebrile and all vitals are within normal limits. His right tonsil is swollen and erythematous, though no petechiae or exudates are seen. His uvula is midline and there is no drooling or “hot potato” voice. Tender cervical lymphadenopathy is present. A rapid strep and HIV testing are negative. A neck CT scan demonstrates a 2.2 cm peritonsillar abscess. An incision and drainage is performed by ENT. Three milliliters of purulent fluid was collected and sent to the Microbiology laboratory for Gram stain and bacterial culture.
Laboratory identification:
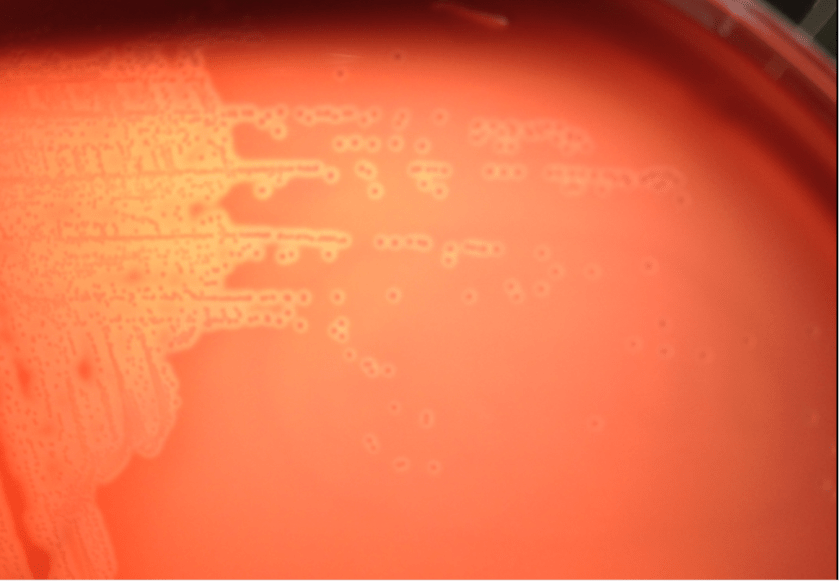
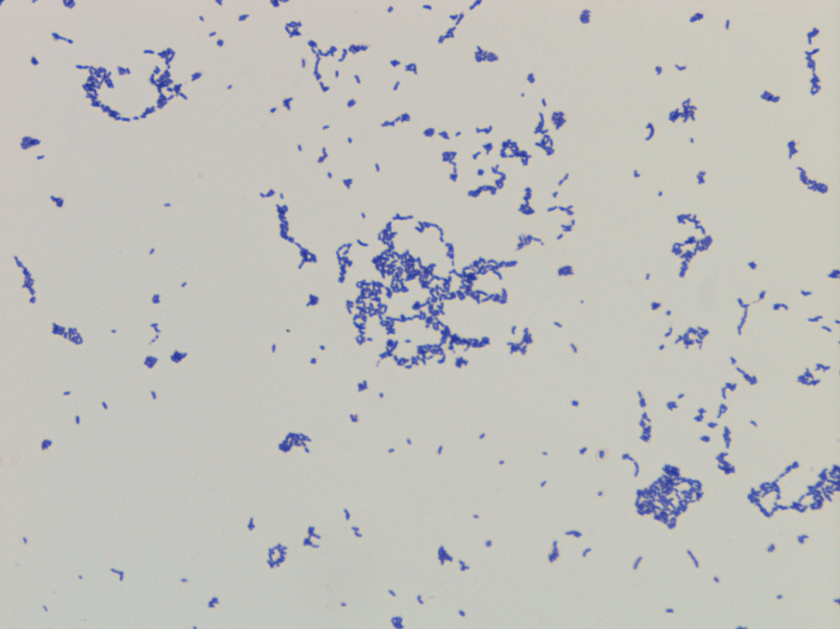
Bacterial culture of the purulent fluid grew small, beta hemolytic colonies after 48 hours of incubation at 35°C. A Gram stain of the colonies showed small Gram positive rods. Biochemical reactions were negative for both catalase and PYR. Arcanobacterium haemolyticum was identified by MALDI-TOF and confirmed with an API Coryne strip. The Streptococcus DNA probe, which is performed on all negative rapid strep results, was also appropriately negative.
Discussion:
Arcanobacterium haemolyticum is a facultative Gram positive bacillus, formerly known as Corynebacterium haemolyticum, which was first characterized in 1946 after being isolated from U.S. service members serving in the South Pacific who developed pharyngitis and a skin rash. A. haemolyticum is most commonly implicated in acute pharyngitis in humans where it is accompanied by cervical lymphadenopathy, tonsillitis, and a rash on the extremities and truck that may be confused with the rash of scarlet fever in 20-25% of cases. The infection usually occurs in patients between 15 and 30 years old. Other infections in which A. haemolyticum has also been implicated include wound & soft-tissue infections, sinusitis, and rarely in cases of osteomyelitis, endocarditis, and meningitis.
A. haemolyticum can be recovered in the clinical laboratory, but it may be missed on throat culture specimens if they are not held for 48 hours or the subtle hemolysis in the first or second quadrants of the culture plate is not observed after overnight incubation. It can also be easily misclassified as non-group A streptococcal species unless close attention is paid to the Gram stain and biochemical test results. Similar to Group A Streptococcus, A. haemolyticum is catalase negative. However, on examination of the Gram stain, A. haemolyticum is a Gram positive rod and the PYR reaction is negative whereas the Gram stain of Streptococcus pyogenes is Gram positive cocci arranged in pairs and chains and PYR positive. Another helpful test in the identification of A. haemolyticum is that it is reverse CAMP test positive. This feature is exhibited due to the fact the phospholipase in A. haemolyticum inhibits the effect of the beta hemolysin of Staphylococcus aureus when they are arranged perpendicular to each other in streaks.
In general, A. haemolyticum is susceptible to penicillin, cephalosporins and vancomycin. Resistance to trimethoprim-sulfamethoxazole is common and rare cases of resistance to tetracyclines, macrolides, clindamycin and ciprofloxacin have been described. As for our patient, he was discharged home on a ten day course of Augmentin and scheduled for tonsillectomy due to his history of recurrent peritonsillar abscesses.

-David Marbury, MD, is a 2nd year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.

This is very educative and informative, thanks
thank you very much, this is resourceful study especially for us in Zimbabwe
Excellent study case and very confusing with beta hemolytic strep