“It was the best of times, it was the worst of times.” In the blood bank, some of the best days can come from some of the worst days. When we come together as a team to work on a puzzling antibody problem, or to respond to a trauma, we can take pride in our work and know we have done our best to help the patient. In the blood bank we are constantly being called upon to learn and to be “disease detectives.” These are the best times. I tell my students that antibody panels are like puzzles and ABO discrepancies are mysteries to solve. Of course, when the Emergency Room is calling for blood for a trauma, or the Operating Room has an emergency surgery on a patient not previously type and crossed, any “problem” to solve can be a bit stressful.
ABO discrepancies are one challenge we face in blood banking. These are generally not clinical problems, but are serologic problems encountered by the blood bank technologists. Some discrepancies are easier to resolve than others, but still usually require a bit of investigation, and time. We don’t see these every day, so they can set us back a step when we do come across them.
One such situation that I recall was a young man in the ER who arrived by ambulance after a motor cycle accident. My trauma beeper went off and I called the ER to see if they wanted blood right away. Typically in these cases we bring them O blood in a cooler, and continue to use type O until we have a blood sample and current type, (performed twice if no prior history) and an antibody screen. In this case we were fortunate in that we got a sample almost immediately, before they started any transfusions. The type and screen was put on our Provue, but the instrument flagged an error on the type. When looking at the gel card, I could see mixed field reactions. Serology results are shown.
Anti-A
Anti-B
Anti-D
Rh cont
A cells
B cells
ABO/Rh
2+mf
0
2+
0
0
4+
?
ABO discrepancies occur when unexpected reactions occur in the forward or reverse grouping or the forward typing does not match the reverse typing. In general, RBC and serum grouping reactions are very strong; therefore reactions less than 3+ usually represent the discrepancy. In this case, testing patient cells with anti-A gave a 2+ mixed field reaction and patient cells and anti-D was only a 2+ reaction. The first step was repeating the test with the same sample. The repeat tube typing gave the same results. Additional steps included testing a new sample, completing the antibody screen, which was negative, and reviewing the patient history. At this time, we did have a positive identification on the patient and a medical record number. The patient had no previous Blood Bank history. However, reviewing the ER admission notes, it was noted that the patient had received 2 units of O negative packed cells in the ambulance en route to the hospital. Viewing the anti-A and the anti-D tubes under the microscope confirmed presence of mixed field agglutination.
Mixed field agglutination describes the presence of two populations of red cells. Mixed field agglutination is seen as small or large agglutinates in a field of many unagglutinated cells. In this case, we observed mixed field agglutination with the patient’s own circulating type A positive red blood cells agglutinating with the anti-A antisera, and the type O donor cells he received remaining unagglutinated. Patients can show mixed field reactions after recent out of group transfusions of as few as 1 or 2 units of packed cells. As well, when group O packed RBCs are transfused to a group A, B or AB recipient, there is always a small amount of plasma transfused. Thus, anti-A, anti-B and anti-A,B are almost always passively transferred. Even though it is unlikely that the passively acquired ABO antibodies will cause in vivo hemolysis, it would be recommended to continue transfusing O blood instead of type specific blood for the duration of the immediate episode and until anti-A antibodies are no longer detectable in the patient’s serum.
This case is an example of an artificial chimerism. Chimerism is the presence of 2 cell populations in a single individual and, in this case, was easily explained by the recent out of group transfusions. This patient was sent to surgery and continued receiving several more units of group O RBCs during and after surgery. The patient’s blood type continued to appear as a mixed cell population during his hospital admission.
There are a number of other scenarios in which mixed field reactions could cause a discrepancy in a patient’s ABO/Rh typing. Some weak subgroups of A (A3) are known for giving mixed field reactions. Mixed field reactions can also be seen in other artificial chimera cases, such as are seen with transplanted bone marrow or peripheral blood stem cells of a different blood type. If mixed field reactions are present, review the patient’s transfusion history to determine if the patient has been transfused with non-group specific RBC components in the past 3 months or received an ABO-mismatched stem cell or bone marrow transplant. More uncommon and unusual are cases of true chimerism, which can occur with fraternal twins. Stay tuned for my next transfusion medicine blog for a discussion of chimerism!
A few key tips to remember when encountering an ABO discrepancy:
Retest the sample first, using a different method, if available
Check for technical or clerical errors
Remember that the weakest reactions are usually the ones that are in doubt
Complete the antibody screen and note positive reactions
Check the patient diagnosis
Check Blood Bank history
Most of all, take a deep breath and relax. You can solve this!
References
Charles Dickens. A Tale of Two Cities. 1859
George Garratty. Problems Associated With Passively Transfused Blood Group Alloantibodies. AJCP, June 1998
Denise M. Harmening, Modern Blood banking and Transfusion Practices, Sixth edition, 2012.
Christopher Sharpe, et al. Mixed field reactions in ABO and Rh typing chimerism likely resulting from twin haematopoiesis. Blood Transfus. 2014 Oct; 12(4): 608–610.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
My last two posts have focused on the WHO Essential Diagnostics List (EDL). The EDL, modeled after the Essential Medicines List, is meant to serve as a model guide for countries to use in the development of laboratory services for diagnosis, treatment, and monitoring of common diseases. The EDL is meant to be tailored to an individual nations disease burden, and India is on track to be the first country with a country-specific EDL. I think this is a tremendous step forward for the field of laboratory medicine worldwide, but I do wonder how this will roll out Low or Middle Income Countries (LMIC). How we will got from a list (actually a draft of a list) to real-time diagnostics in the developing world? Let’s take a step back and look at what access to laboratory testing really looks like, and then discuss some innovative diagnostics that might help increase access to useful diagnostics.
In the US, we have many labs tests available – so much so that laboratory utilization has become a very real area of study with groups like Choosing Wisely, PLUGS, and Preventing Overdiagnosis dedicated to helping guide appropriate use of in-vitro diagnostics (IVDs). The US has over 250,000 accredited laboratories, and 18,000 clinical pathologists. That’s about 5.7 pathologists per 100,000 people. In contrast, the continent of Africa has about 1 million people per pathologist, and some African countries have over 5 million people per pathologist. It’s difficult to find a number of laboratories in LMICS, because many are mom and pop type shops that aren’t registered with the Ministry/Department of Health. Test menus are often limited to cell counts and rapid testing, and proficiency testing or quality control is not practiced.
Challenges to building laboratory capacity in LMICs are environment, economics, and education. Environmental challenges include extreme temperatures, limited electricity, and limited access to water. Some point of care options that might be able to work in these environments just aren’t affordable. Many people in LMICS make around $2 USD a day and a $10 iStat/Piccolo/your favorite POC chemistry device cartridge is just out of reach especially if the testing needs to be repeated frequently for monitoring disease progression. Lastly, education remains a challenge as laboratory medicine including not not only technical skills but also the use and interpretation of lab tests is not frequently taught in LMICS.
However, there are many different innovative diagnostics being debuted or in development with these challenges in mind. There are definitely trends in the area of new diagnostics for the developing world. The most distinctive trends are: smartphone imaging, smartphone spectrophotometers, transdermal testing, and paper based sample collection. In my next few posts, I’ll take us through examples of each of these, and I’ll start now with smartphone imaging.
Smartphone imaging is essentially using light boxes, cameras, or apps, to turn a smartphone into an imaging device. Smartphones are even being used as simple ultrasounds! A smartphone microscope can be useful in diagnosing tropical infectious diseases. A good example is the LoaScope, developed by the Fletcher Lab at UC Berkeley. Dr. Daniel Fletcher is known as the “father of the cell phone microscope”. The LoaScope is a mobile phone based microscopy platform plus an app-based algorithm for the detection of L. Loa. The device is elegantly simple: a 3D printed case with a rest of the mobile phone. The case contains a USB port, bluetooth controller board, and LED array, and a carriage for a capillary slide. Blood is introduced to the capillary slide and imaged by the phone. A 5 sec video is captured by the phone, and then analyzed via app that uses a algorithm based on the the wiggling motion of the loa worm. The algorithm actually distinguishes the movement of blood cells as the loa worms move between them! The interpretation of the video lets the user know if the parasite is present or not present. Another bonus the device is that a georeference is captured with every video, which is great for epidemiological studies. In 2017, the LoaScope was used by the NIAID to testing over 16,000 subjects in Cameroon. Because of the LoaScope, over 15,000 subjects were successfully treated with ivermectin without serious complications.
There are some key elements to the LoaScope that are common across the new, innovative diagnostics for the developing world. First, the 3D printed case. 3D printing seems to really be helping this field jump ahead by decreasing the costs associated with creating the physical structure of the devices. Secondly, the device does not require special specimen preparation, nor does it need reagents. Lastly, a simple read-out is a available to the user in real time.
In summary, the EDL is great for telling us what test are, well, essential. Innovative diagnostics are going to help us get to those hard-to-reach places. I look forward to continuing to investigate these with you!
–Sarah Riley, PhD, DABCC, is an Assistant Professor of Pediatrics and Pathology and Immunology at Washington University in St. Louis School of Medicine. She is passionate about bringing the lab out of the basement and into the forefront of global health.
When you put your money into a vending machine, there is always a gamble. There is a risk of the machine not working- it will take your money but not dispense any products, or the item might just get stuck inside the machine and no amount of banging or tipping will help. As humans, though, we take that risk, and the “danger” is only the loss of some money.
The potential danger for a patient in the hospital can be higher. For years, healthcare organizations have been working with other agencies to improve patient safety. Two professions that often serve as the gold standards of safety culture are the airline and nuclear industries. I have seen many speakers over the years from those agencies give amazing speeches on attaining such high safety ratings. On my more cynical days, I often think that hospital caregivers will probably never reach the same level of safety that is seen in the nuclear and airline industries, and I feel there is a “logical” reason for that. If a pilot or an employee at a nuclear plant makes an error, it potentially places his or her own life at risk, so more attention is paid and fewer errors are made. If an employee makes a mistake when treating patients, the error affects the patient and not the employee, so paying constant attention may not seem as urgent to the worker (I told you these were cynical thoughts).
Now let’s go back to the vending machine. There is some risk to take when putting money into the machine, but once the money is accepted, we feel free to make our selection. Now, if you’ve ever watched someone make such a selection, you may notice that they will not risk making a mistake- they will check, double-check, and even triple-check to make sure they press the right button combination so they get the correct item. The outcome of any mistake made here directly affects the person craving that specific soda or candy bar, so the caution taken to ensure a proper selection is greater. Is that just human behavior? Do we make safer choices if the risk directly affects us?
If that theory is true, then laboratory employees should always work safely. They should always wear proper PPE, they should never eat or drink in the labs, and they would never use their cell phones in the department. Yet many lab safety professionals know that these unsafe behaviors still exist, even in today’s world where we handle highly infectious organisms and deal with bloodborne pathogens daily. If unsafe behaviors lead to exposure- to harm that directly affects the employee- why do these behaviors remain? What’s missing from the picture? I believe the answer lies somewhere between complacency and education, but I also believe both can be handled with increased safety awareness.
Staff who have been in the lab for many years can lose their respect for the chemicals and samples they handle every day. They know that they have worked with them for many years with no negative outcomes, and older lab employees remember the days when all of those unsafe behaviors ran rampantly. Ask a mature lab tech about smoking in the lab, placing party casseroles in the microbiology incubator to keep it warm for the party, and even mouth pipetting. Many laboratory employees worked in environments like that and came out unscathed. But not everyone did.
The reason OSHA and other lab accrediting agencies put forth more stringent safety regulations over the years is because so many lab employees were infected, injured, or killed as a direct result of those unsafe actions. Even in the span of my ten years in lab safety, I can tell a different horror story to each person who says they are fine not paying attention to safety rules. It’s important to do that. Injuries and exposures occur every day in labs, and if they happen in your lab, it is vital the story is told to other staff. Transparency and discussing methods of prevention with staff makes an impact because it makes the danger real and more personal. If you’re in a lab where accidents are rare, that’s great- but make sure you continually raise awareness of the inherent dangers in the lab work place by finding stories of events in other labs and talking about them. Tell stories of near miss events as well. It is good to discuss events that were averted through solid safety practices as well.
Lab safety education, both initial and on-going, are key to helping staff understand the environments in which they work. Safety competencies, drills, and tests are good tools to keep awareness of the lab’s safety issues on the minds of employees every day. Telling safety stories and sharing incidents are other actions that can also reduce safety complacency. Every day our employees come to work, and the potential dangerous possibilities are always there in the lab “vending machine.” Help them to be careful to make the correct selection so they can remain healthy and happy with the career choice they have made.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Welcome to a new series where I’ll explore the role of lab medicine in the care of transgender patients! Many of you may be asking yourself, “Why should I care? I’m in the lab far separated from these dicey patient care issues.” However, the lab plays important roles as the patient moves through the healthcare setting. Everywhere from name confirmation by phlebotomists and before blood transfusion to sex-specific reference intervals, the lab interacts with the healthcare of transgender patients in important ways. With more transgender patients presenting for clinical management, and more clinicians armed with hormone therapy guidelines created and endorsed by the Endocrine Society, it will be expected for laboratory professionals to know how to manage these patients too.
For me, my first encounter with transgender healthcare through the laboratory was during my clinical chemistry rotation when the lab paged me about a very high estradiol value 10 times higher than the upper limit of normal. I found that the patient was a transgender woman taking excessive hormone doses. Their doctor counseled them and persuaded them to stick with their prescribed dose, because the risks of supraphysiologic estrogen is not known. While we were glad the patient didn’t have an estrogen secreting tumor, I wondered how this hormone therapy may affect other aspects of their health and physiology as reflected by lab values.
After a literature review, I found there were few studies that addressed changes in lab values with hormone therapy. Those papers I found had limited numbers of patients, so I decided to find the answers for myself. Subsequently, I (along with two medical students) studied a large number of patients attending transgender specific clinics. I’ll discuss our findings as a part of this series.
For now, I’ll go over terminology so everyone can be on the same page. Many of us are likely unfamiliar with the experiences of transgender individuals and don’t realize how what appears to be a verbal misstep can be offensive. The first distinction to make is the difference between sex assigned at birth and gender. Sex is assigned at birth to a child, often based on external anatomy. Gender is the set of behaviors and roles that society or culture assigns to a person that ranges from masculine to feminine. However, gender identity is a deeply held internal sense of whether you consider yourself male, female, both or neither. This is distinct from sexual orientation, which one colleague explains: “orientation is who you go to bed with, gender expression is what you go to bed wearing, and gender is who you go to bed as.” When one’s gender identity is concordant with their sex assigned at birth, they are called cisgender; whereas, discordance between sex assigned at birth and gender identity is termed transgender (I think of cis and trans stereochemistry in organic chemistry). The process of using medical or surgical interventions to transition is referred to as gender-affirming hormone therapy or gender-affirming surgery.
The easiest way to address someone whose preferred name doesn’t match their sex in their record is to address them as they appear: use female pronouns if they are dressed as a woman and male pronouns if they are dressed as a man. And if you’re not comfortable with that, a simple “How would you like to be addressed?” is appreciated. I will go into the importance and challenges of legal sex/name and pronouns in the electronic health record in a later discussion.
To round out the topic of terminology, I’d also like to mention a few terms that should be avoided. “Transgendered” adds an unnecessary “-ed” as transgender is already an adjective. It is further confusing, because it makes the word sound past tense (we wouldn’t say “lesbianed,” for example). Rather, a person undergoes gender transition as they accept and express their gender identity through a set of social, physical, medical or legal changes (sometimes call gender affirmation process). Using terms like pre-op/ post-op/ sex change overly emphasizes the role of surgery in the process, and thus gender transition is more inclusive. Similarly, asking for someone’s “real name” overly emphasizes their legal name and there are limited situations where that would be necessary to use. Derogatory terms include tranny, hermaphrodite, or transvestite and shouldn’t be used even when referring to people who are intersex or wear clothes of the opposite sex.
Thanks for making it all the way through this first post, I look forward to hearing any questions you have and exploring this topic together further!
References
Goldstein Z, Corneil TA, Greene DN. When Gender Identity Doesn’t Equal Sex Recorded at Birth: The Role of the Laboratory in Providing Effective Healthcare to the Transgender Community. Clinical Chemistry 2017; 63(8):1342-1352.
Rosendale N, Goldman S, Ortiz GM et al. Acute Clinical Care of Transgender Patients. JAMA Intern Med. Published online August 27, 2018.
Roberts TK, Kraft CS, French D et al. Interpreting laboratory results in transgender patients on hormone therapy. Am J Med. 2014;127(2):159-62.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
Here comes the fun part. It’s taken a day for library prep, an overnight run for the clonal amplification; the next day includes loading the chip with the ISPs and then running the chip on the sequencer. After the chip has run on the sequencer, the data is pushed from the sequencer (the PGM) to the server connected to the sequencer. This aspect of NGS surprised me – the size of the files is amazing – for one 316 chip, the file that includes all of the raw data averages about 100GB. To deal with this amount of data, the server attached to the sequencer is 12TB, and even still we have to have a procedure to deal with removing files off that sequencer to keep space for future runs.
Anyway, the raw data is pushed to the server and the data analysis begins. The Torrent Suite Software first analyzes the ISP info, as shown in the graphic below. It gives a “heat map” of the chip (the football shape) in which red means the wells in those areas were full with ISPs. Yellow means there are fewer ISPs and blue means there are none. So, you can see below, there is a small area of blue within the football shape – this area did not have any ISPs in it. 92% of the wells on this chip were filled, however, which is about the max a chip can be loaded.
These ISPs are then broken down into categories. First, how many of the wells had ISPs in them – here, 92.5% of the 6,337,389 wells contained ISPs. Of those ISPs, 99.8% of them have product on them that can be sequenced (Live ISPs). Of those Live ISPs, 0.4% of them contain control Test Fragments and 99.6% of them contain actual patient sample library amplicons. The Test Fragments are spiked in prior to sequencing and act as a control to evaluate how the sequencing run performed. Lastly, the ISPs that contain patient sample library amplicons are analyzed. Those ISPs that contain more than one amplicon (say it has an amplicon of EGFR Exon 19 and another specimen’s amplicon of KRAS Exon 2) give mixed signals and cannot be analyzed, so they are thrown out of the data analysis and into a bin called “polyclonal”. Low quality ISPs are also thrown out – anything that did not pass the thresholds for quality. And lastly, ISPs that only contain adapter dimers are thrown out. For a run of AmpliSeq Cancer Hotspot Panel v2 specimens, most of which come from FFPE specimens that are low quality to start with, a run that contains over 50% Final Library ISPs is actually a very good run, interestingly enough. The 316v2 chips are rated to sequence 1 million reads (each ISP yields one read), and on this example run, over 3 million reads were sequenced, so this is a successful run.
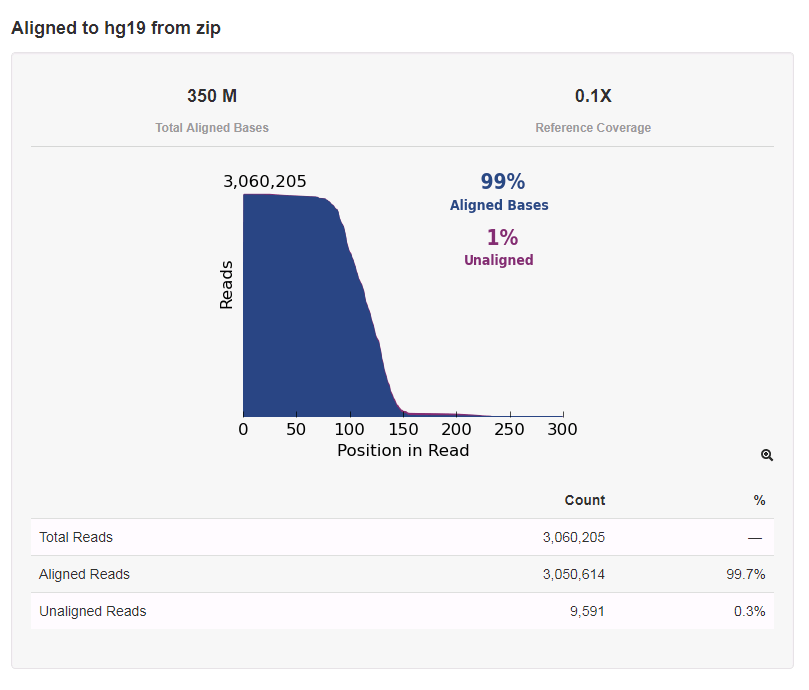
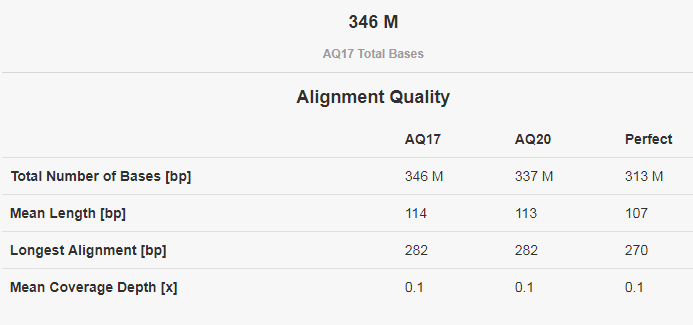
After the ISPs are analyzed and the high quality ones are kept, the analysis goes on. The Torrent Suite software then calls the bases based on the raw flow data. These bases are then aligned to a reference, in our case hg19, a commonly used human genome reference. Quality scores are assigned at this point. A Phred-based quality score is used for NGS, shown in the table below.
Lastly, the reads are put into bins based on the barcode that was used for each patient specimen – remember the small part of the adapter that was added in library prep so that the specimens could be mixed together? The software reads that adapter sequence then assigns each read based on those sequences. The specimens should all have approximately the same number of reads since they were normalized to the same concentration at the end of library prep, but there may be some variability due to specimen quality, as you can see below.
In next quarter’s post, we will dive into the individual specimen results!
-Sharleen Rapp, BS, MB (ASCP)CM is a Molecular Diagnostics Coordinator in the Molecular Diagnostics Laboratory at Nebraska Medicine.
Recently, Lablogatory interviewed R. Marshall Austin, MD, PhD, in regards to the benefits of using both liquid-based cytology and HPV testing to screen for cervical cancer. The interview below has been lightly edited for brevity and clarity.
Hi, Dr. Austin. Thanks for joining us today. Can you tells us a bit about your background?
I consider myself a gynecological pathologist, which includes surgical pathology and cytology. I’ve been involved with cervical screening issues for quite some time. Going back to the 90s, and even before that with CLIA ’88. My PhD is in virology, which is relevant now with the all the HPV issues. I did my subspecialty training in GYN and breast pathology and cytology at the armed forces institute of pathology.
Over your career you’ve authored or co-authored over 80 papers relating to cervical cancer screening. What made you so interested in this field of study?
It was an area that became a hot topic with CLIA ’88. CLIA ’88 was precipitated by a Wall Street Journal expose on Pap smear screening in the United States, which was ironic because the Pap smear has been the most effective cancer screening test in the history of medicine. This drew me in, since it was my subspecialty area of interest. There had been technological advances in the field even though the Pap smear itself hadn’t changed that much since it was introduced during World War II. Computer-assisted screening, liquid-based cytology, HPV testing all really have dramatically changed the field.
What was your initial reaction when the US preventative services task force released their draft document on cervical cancer screening recommendation in September of 2017?
I thought it was a mistake. I wrote a letter why I thought so, and apparently a lot of other people did, too.
How integral was the pathology and medical community’s reaction to this draft document in changing the USPSTF’s recommendations to include co-testing?
I’m sure that the feedback had a cumulative impact. I’ve heard different views on what components were most instrumental.
I had read online at the end of last year a pre-publication paper published by the Journal of the National Cancer Institute. I had seen their figures presented by Walter Kinney as early as October at a meeting in Amsterdam. I asked him where these figures available, and he said they were going to be published. I thought their results were probably different than what we would have seen in our own lab. So I thought we really need to look at our own data in the exact same format as the data presented in the JNCI. We were able to do that by about March.
Wow! That seems really fast, considering how large your data set is.
We have kind of an unusual set up here because I work with two information scientists here at the University of Pittsburg. We automatically have all of our data being taken from our LIS into a cervical screening model which we call the Pittsburgh Cervical Cancer Screening Model and we have over 13 years of data. So we’re in kind of a unique position to very quickly put our data into different types of formats. Agnieszka Onisko, the information scientist on the publication, was able to quickly look at our data and get it into the same format as the paper from Kaiser. Once I saw how different our results actually were, my goal was to get the paper out before the USPSTF report came out. We had our tables and figures by March and I submitted the manuscript to AJCP in early May.
Let’s talk a little bit about the benefits of cotesting, and some of the downsides.
Well, the reason I always tell people, the reason that women get screened is because they don’t want to get cancer and they don’t want to die of cancer. Getting screened isn’t a pleasant experience, necessarily, but women don’t get screened because they’re worried about dysplasia or some other condition. They’re worried about cancer. The other thing that’s always been misunderstood is the limitations of screening. Screening was effectively sold to the American public by the American Cancer Society and the National Cancer Institute, and while it was an effective campaign, it basically left women with the impression that if they get screened, they won’t get cancer. Although cervical cancer screening has been the most effective cancer screening program ever, it’s never been perfect. A paper out of England in 2016 had a sophisticated analysis about the effects of cytology screening on cancer rates in England. It estimated that about 70% of cancer mortality was being eliminated with screening, and could potentially be as high as 83%, which still isn’t 100%. So when women get cancer, they get upset. My general philosophy has always been that we should do as much as we can to minimize cancer in the screened population because that’s what the public wants and expects.
The disadvantages of cotesting is one, it adds costs. Two tests cost more than one, after all. And also, cotesting adds the potential for more red flags that require potential investigation that can increase the number of procedures. Having said that, and having been involved in a number of years especially in cases where litigation is involved the public wants and expects the most protection possible. So, to me, the extra cost is still in line with what the public wants: the maximal possible protection.
A 50 year old female was admitted for acute renal failure on CKD stage IV, present with gross hematuria, anemia (due to blood loss) and hypertension. The patient has a significant history of unresolved cryoglobulinemic vasculitis initially diagnosed in 2016 and has been treated by several rounds of rituximab. Other medical histories include Sjogren’s syndrome, MGUS with monoclonal IgM Kappa, coagulopathy (protein S deficiency, on anticoagulant), hyperviscosity, myalgia, deep vein thrombosis, leg edema with superficial ulcer, pulmonary embolus and membranoproliferative glomerulonephritis (MPGN). Kidney biopsy revealed intraglomerular hyaline thrombi consistent with cryoglobulinemic glomerulopathy, interstitial fibrosis tubular atrophy, arterial sclerosis, suggestive thrombotic microangiopathy. Immunohistochemistry was positive for C3, IgM, Kappa, Lambda and CD68. Bone marrow biopsy shown dyserythropoesis without malignancy. Blood testing shown negative hepatitis panel and undetectable C4.
We observed unusual cryoprecipitate test results from this patient: gelatinous appearance precipitate which accounts for more than 40% of volume was observed in both plasma and serum and cannot be cleared at 37C° after several hours of incubation. Further testing shown incubation at 56°C for 30min cleared up the serum but not the plasma. After checking the test history, we found that there was a similar situation for the patient’s cryoprecipitate test a few months back earlier in 2018, and was reported negative for cryoglobulins due to the heat-insoluble nature of the precipitate. Patient was transfused for anemia. No plasmapheresis was done. Due to the patient’s incomplete response to rituximab, Cytoxan was also added to help improve the symptoms.
Cryoprecipitate
Definition: Cryoprecipitates (or cryoproteins) are blood proteins that form precipitates or gels at temperatures lower than 37°C and typically re-dissolve after warming up to 37°C. There are two types:
Cryoglobulin (CG): precipitate from both serum and plasma; either immunoglobulins or a mixture of immunoglobulins and complement components
Cryofibrinogen (CF): precipitate from plasma only; typically composed of a mixture of fibrinogen, fibrin, fibronectin, and fibrin split products
Lab Testing done in our hospital:
Blood are collected in two pre-warmed tubes (one serum, one EDTA plasma) and kept in warm water (37°C) until the serum tube clots.
The plasma and serum are extracted at room temperature, and then stored in refrigerator for 72 hours.
If cryoprotein is present, a precipitate or gel will be seen. An aliquot of the serum is rewarmed at 37°C to verify the cryo-nature.
The precipitate as a percentage of the original serum volume is measured in an ESR tube to determine the cryocrit.
Immunofixation is ordered per pathologist to identify the immunoglobulin compositions of the cryoglobulin.
Cryoglobulinemia
Classification
Strictly speaking, cryoglobulinemia refers to the presence of cryoglobulin (CG) in a patient’s serum, which could be either asymptomatic or present with apparent clinic syndromes (i.e. cryoglobulinemic vasculitis). Cryoglobulinemia can be classified into three types (see table below [1]), with mixed cryoglobulinemia (type II and type III) representing 80% of the cases.
Clinical Manifestations
Type I cryoglobulinemia is frequently asymptomatic, while mixed cryoglobulinemia manifests clinically by a classical triad of purpura, weakness and arthralgias, as well as some other conditions including MPGN, chronic hepatitis, peripheral neuropathy, lymphoma, Raynaud’s, Sjogren’s syndrome, etc.
The presence of heat-insoluble cryoglobulins is rare, and its pathogenesis is poorly understood. On the other side, it may indicate sever clinical consequence as seen in our case and some others as mentioned above.
Essential type II cryoglobulinemia with cryoglobulin-occlusive MPGN and MGUS (Clin Chim Acta. 2009 Aug;406(1-2):170-3):79 y.o. female admitted due to edema and renal failure, cryoglobulin re-dissolved at 56°C, composed of monoclonal IgG-Kappa and polyclonal IgM.
HCV associated thrombotic microangiopathy and cryoglobulin-occlusive MPGN (Am J Med Sci. 2013 Oct;346(4):345-8):57 y.o. female, cryoglobulin re-dissolved at 47°C, composed of monoclonal IgM-Kappa and polyclonal IgG. Symptoms only partially resolved upon treatment of plasmapheresis, corticosteroids and antiviral therapy of peginterferon plus ribavirin.
Essential type I cryoglobulinemia with massive cryoglobulin-occlusive glomerulonephritis (Am J Kidney Dis. 1995 Oct;26(4):654-7):54 y.o. male progressed to ESRD prior to the detection of cryoglobulin. Cryoglobulin with white gelatinous appearance re-dissolved at 54°C, composed of monoclonal IgG-Kappa.
Primary Sjogren’s syndrome with type II cryoglobulinemia and mesangiocapillary glomerulonephritis (Nephrol Dial Transplant. 2000 Jun;15(6):917-8):82 y.o. patient with IgM-MGUS, negative BM, deposition of IgG, IgM and C3 on kidney biopsy, decreased complement levels, negative HCVAb, HBsAb, HBsAg. cryoglobulin re-dissolved at 47°C, composed of monoclonal IgM-Kappa and polyclonal IgG-Kappa.
-Rongrong Huang, PhD is a first year clinical chemistry fellow at Houston Methodist Hospital. Her interests include general clinical chemistry, genetic biochemistry and applications of mass spectrometry in clinical laboratories.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
This month I think it’s important to take a step back from clinical pearls, developing our interpersonal skills, and interdisciplinary dynamics and go back to what I started writing about here on Lablogatory: public health and shaping policy. (Sorry, no Transformers, Simpsons, or Star Trek this time.)
Now, you may or may not have heard in recent news that the United States Preventive Services Task Force (USPSTF) updated their long-standing guidelines for screening women for cervical cancer. Normally I wouldn’t file this away under “exciting must-read,” but I was piqued when I also read that ASCP along with the College of American Pathology (CAP), American Society of Cytopathology (ASC), American Society for Colposcopy and Cervical Pathology (ASCCP), the Society of Gynecologic Oncology, the American College of Physicians (ACP), the American Society for Cytotechnology (ASCT), the American Cancer Society (ACS) the Papanicolaou Society of Cytopathology, as well as the American College of Gynecologists (ACOG) and other professional institutions and individuals voiced concerns over the changes to the USPSTF standard.
This is a topic that can be discussed for days, but I’ll do my best to give you the readers’ digest and present the main contentions regarding this standard of patient care and laboratory methodology.
Woah. What’s going on?
Basically, because of some new research and recommendations, the USPSTF—a body which publishes the standard of care for nearly every conceivable aspect of preventive care in the US—rolled back on the algorithms for screening women for HPV and cervical cancer. It all comes down to the utilization of co-testing (doing both Pap smear cytology and HPV testing for certain age demographics) as a point of contention. Under a banner of addressing keywords like “cost” and “harm,” these new recommendations have left clinicians both in and out of the lab in stirrups—sorry, couldn’t resist that one. But don’t worry, I wouldn’t be able to track these changes or even understand them without some sort of visualization. When it comes to recommendations, standards, and guidelines I’m about as proficient as a broken manual diff counter…
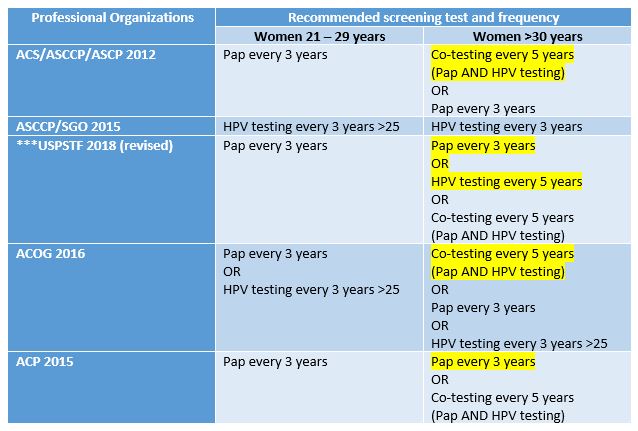
Figure 1. These are the guidelines as they stand from each of the major professional organizations concerned with cervical cancer screenings. Dissenting/recommended opinions are highlighted. To the untrained eye this is very unexciting. The bottom line is that the USPSTF no longer recommends co-testing for screening. Source: adapted from UpToDate
Slow down. Explain co-testing and primary testing? What exactly do the old and new recommendations mean?
Okay. When women undergo routine cervical cancer screening they receive Pap smears (cytologic examinations) every three years. This testing has been the standard for a number of years and is adequately sensitive for women up to the age of 30. Often times, these younger women may have slight intraepithelial changes (LGIL) which are considered low grade and remiss on their own. After that age it has become standard practice to add the additional test (while collecting the Pap specimen) of HPV DNA testing. This adds an increased level of sensitivity/specificity and is called co-testing. The new recommendations depart from this co-testing model, citing that there are increased harms (in the form of false positives) which ultimately lead to waste and unnecessary testing for women after the age of 30. Primary testing would mean only screening with HPV DNA assays after 30. According to the National Cancer Institute, all available literature on the subject of HPV and cervical cancer testing adequately demonstrates that co-testing is the best option. A number of studies were compiled to address the harm vs. benefit of Pap and HPV testing. Together, however, these tests decrease the incidence of cervical cancer. New guidelines were made based off mathematical projections and cost-benefit analyses which try and minimize losses for screening. Dr. J. Kim, a public health researcher at Harvard, was integral in contributing models which projected the cost/benefit of changing HPV guidelines. Essentially, the study projected that, when considering “harm” (i.e. colposcopy/false negative) abandoning co-testing changed the mortality rate from 0.3-0.76 per 1000 women with co-testing, to 0.23-0.29 per 1000 women with primary HPV testing. An impressive and significant statistical advantage. However, the total number of unscreened women with mortality rates was between 1-2%. This study was a microsimulation done from historical data within rates of cytologic detection and retrospective testing data on women, projected for a future hypothetical 5 year interval. Fascinated by this study, I tried to reach out to Dr. Kim to discuss limitations in using models and simulations and public health evidence to change practices, but I’m sure she is busy and could not respond in time.
So, to co-test or not to co-test, that’s the question. Right?
In its simplest sense, yes. The major medical professional societies also publish their most current recommendations for practice standards—and the issue is that the USPSTF took a departure from what most of the professional societies recommend regarding co-testing. Late last year, the CAP, ASC, ASCT, ASCP, and the PSC issued a statement under their independent collaboration called the Cytopathology Education and Technology Consortium (or CETC). In this response to the USPSTF guideline changes, they discussed their concerns. Specifically, their objections center around the fact that without co-testing for screening, cancer prevention might be impacted negatively. The CETC claimed that sensitivity is already maximized with previously recommended co-testing guidelines. They also cite that there is only one FDA approved HPV primary screening test available—and not all labs have it! More so, CETC discussed the need to keep morphological testing continuous for women who have histories of Pap smears, the potential to overwhelm colposcopy services for screening all positive HPV patients, and the honest reality that not all clinicians would be compliant with the way the USPSTF recommends testing. The bottom line from this consortium:
Cytology and high-risk HPV co-testing should be kept as the standard screening for women aged 30-65
Primary HPV screening should only be done with validated, FDA approved testing methodologies
HPV screening methods should continue their current schedule until longitudinal data can offer new evidence for changes
So, what’s the current technological climate for how we test for HPV?
Currently, most clinicians do co-testing. The standard for Pap smears utilizes a physical tool to collect epithelial cells from the cervix at vaginal, ectocervical, and endocervical sites. The swabs are prepped on 1-2 slides, fixed with alcohol or other spray cell-preservatives and sent to labs for cytologic examination. The basic Papanicolaou staining procedure uses hematoxylin for nuclear staining, and two cytoplasmic counterstains. This is essentially a modified H&E stain to clearly visualize morphology. Staining is rarely done manually and some instruments offer stain/prep combination capability. I couldn’t find too much information on this, but I remember there not being too many official FDA approved prep machines for Pap specimens. Cytotechs and pathologists read the slides and issue sign outs on morphology according to the Bethesda system—very heavy read, don’t bother; essentially it has three main categories of normal, benign changes, and abnormal. According to ASC “for squamous lesions, TBS terminology includes atypical squamous cells of undetermined significance (ASCUS), low grade intraepithelial lesion (LGSIL or LSIL), high grade intraepithelial lesion (HGSIL or HSIL) and squamous cell carcinoma. Some laboratories also incorporate other terminologies of dysplasia and/or cervical intraepithelial neoplasia (CIN) into their reports. For glandular lesions, TBS terminology includes atypical glandular cells of undetermined significance (AGUS) and adenocarcinoma.”
As of now FDA approval for HPV primary testing for high-risk strains is limited to the Roche Cobas hrHPV test. I could link you to their website, but you’ll be sold right away. They tout the future of HPV screening is HPV primary testing and to do away with the Pap! Their graphs and figures are impressive (just like their price tag!) and there’s no doubt that sensitivity is something that real-time PCR provides more than cytologic examination. But, as always, more assays will be approved, and advancements will tweak the sensitivity and specificity higher and higher.
Got it. So, technology and lab tests are always advancing, why can’t we make this change?
It’s not so easy to change the method or assay we use to screen or diagnose patients in the lab. If you recall, I talked about how the hospital I’m currently rotating in is leading the region in advancing the new high-sensitivity troponin assays. It’s still a hard sell to many even though the data and projections seem to all point to a green light. But that’s a paradigm shift that involves side-stepping from one immunochemical assay to a more sensitive immunochemical assay. It’s the same stuff, just sharper and with more clinical data to interpret with regards to acute coronary symptoms and clinical risk stratification. Swapping an old car for a new car. This conversation is a bit more complex. The recommendations for cervical cancer screening suggest that we should move away from mostly morphologically-driven, human-based cytology interpretation and move toward PCR-based assays for detection. Literally apples to oranges. We might think we know which one is better right now, but longitudinal studies are the only way to really tease out if this change in practice to improve patient outcomes in the long run.
Where do we go from here?
Ultimately, I think a few things need to happen for this recommendation to become standard practice. First, professional societies in every discipline from gynecology to cytology need to come to an agreement. It remains to be seen whether certain agencies will adopt and recommend the USPSTF guidelines, and statements from groups like CETC reveal a vote of no confidence in this current climate. Ultimately, because of numerous objections (including the ones from ASCP and the CETC) the USPSTF does say that co-testing is still optional between patient and provider, so we’re not really in crisis mode. But what happens when the advancements and the recommendations catch up to our ability to abandon the cytologic contributions of a future useless Dr. Papanicolou? We could probably deal with that when it comes to fruition, but until then we have a real discussion about what “harm” really is. Is colposcopy flat out harm? Or are the false positives that reflex to further testing? Is the current practice a safety-net for populations across socio-economic tiers with varying access to screening in the United States? When compared to other countries, HPV prevention, vaccination, and screening is much more easily facilitated. Is this a contributing factor for our messy guidelines? Will there be more options for FDA approved methodology in the near future? There remain a number of good questions which require examining cross-sections of data and patient outcomes. And, I believe, we may see change soon—but not quite yet.
What are your thoughts? What have you experienced in your lab or clinic? Leave your comments below!
Kim, J. 2017. Screening for Cervical Cancer in Primary Care. Journal of the American Medical Association (JAMA). 2018;320(7):706-714. Doi:10.1001/jama.2017.19872
Lerman, L. 2018. Screening for Cervical Cancer – New Tools and Opportunities. Journal of the American Medical Association (JAMA) – Opinion, Editorial. Vol. 320(7):647-649
Nayar, R. 2017. Primary HPV Cervical Cancer Screening in the United States: Are We Ready? Journal of the American Society of Cytopathology (2017) 7, 50e55
Sawaya, G. 2018. Cervical Cancer Screening—Moving from the Value of Evidence to the Evidence of Value. Journal of the American Medical Association (JAMA), Internal Medicine. doi:10.1001/jamainternmed.2018.4282
USPSTF. 2018. Screening for Cervical Cancer, US Preventive Task Force Recommendation Statement. US Preventive Task Force. Journal of the American Medical Association (JAMA) 2018;320(7):674-686. Doi:10.1001/jama/2018.10897
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
The patient is a 48 year old male who presented after a motorcycle crash where he slide sideways into a ditch. He did not lose consciousness. At presentation he complained of pain across the abdomen, right wrist and left shoulder. He also had shortness of breath and chest wall pain. He denied hitting his head and was helmeted. He underwent exploratory laparotomy with repair of traumatic diaphragmatic hernia and left chest tube placement with post-operative course complicated by significant leukocytosis and bandemia on post-operative day 5 which triggered CT re-imaging of the chest/abdomen/pelvis. This study demonstrated intraperitoneal free air that prompted repeat exploratory laparotomy with subtotal colectomy with the abdomen open and wound vac in place. On post-operative day 9 the patient had an increasing white count that prompted return to OR with bowel staple line demonstrating leak, which prompted a small bowel resection, and ileostomy formation. After leaving the OR, the patient experienced worsening septic shock. Aggressive antibiotic therapy and IV fluid resuscitation was continued. Blood cultures taken on post-operative day 9 grew a large Gram positive rod. Growth of this organism was seen both aerobic and anaerobically.
Laboratory Identification
Image 1. Gram stain of the anaerobic blood culture bottle showing gram positive/variable rods.
Image 2. Aerobic blood agar plate showing small clear colonies.
Blood cultures showed box shaped gram positive/ variable rods that were growing on blood agar plates both aerobe and anaerobically. It was motile, indole and catalase negative, and esculin positive, and was identified by the MALDI to be Clostridium tertium.
Discussion
Clostridium tertium is an aerotolerant gram positive rod that is widely distributed in the soil and can also be found the GI tract of animals and humans (1). C. tertium is non-toxin producing and produces terminal spores in anaerobic conditions (2). Infection with C. tertium is uncommon though it has been increasing in frequency as a cause of bacteremia, especially in patients with neutropenia, the immunocompromised, those with hematologic malignancy, those with inflammatory bowel disease, and in people with abdominal trauma or who have undergone abdominal surgery. Less commonly, C. tertium can be isolated in spontaneous bacterial peritonitis, enterocolitis, meningitis, septic arthritis, necrotizing fasciitis, post-traumatic brain abscess, and complicated pneumonia in mono- or polymicrobial infections (1). Additionally there has been a link between C. tertium infection and attempted suicide with the herbicides containing Glyphosate, as it causes GI toxicity which alters the gut environment (2). As with Clostridium difficile, the use of broad-spectrum antibiotics such as third-generation cephalosporins might predispose to intestinal colonization with C. tertium (1).
Increases in the diagnosis of C. tertium may be related to better diagnostic equipment such as the MALDI as it can easily be confused with a facultative anaerobic Bacillus or Lactobacillus species due to its gram variable appearance and ability to grow in aerobic conditions. A distinguishing feature between Bacillus species and C. tertium is negatively of the catalase reaction as Bacillus should be positive. Lactobacillus can still be a challenge as they are also catalase negative.
The treatment of C. tertium infection is complicated due to resistance to various antibiotics, including various beta-lactam antibiotics (such as third- and fourth-generation cephalosporins), clindamycin, daptomycin, and cotrimoxazole. Older reports state resistance to metronidazole, but this has not been confirmed in more recent publications. Available data indicate sensitivity to vancomycin, carbapenems, and quinolones (1)(3).
References
Salvador F, Porte L, Durán, L, Marcotti A, Pérez J, Thompson L, Noriega LM, Lois V, Weitzel T. Breakthrough bacteremia due to Clostridium tertium in a patient with neutropenic fever, and identification by MALDI-TOF mass spectrometry. International Journal of Infection Disease. 2013;17:11 (1062-1063). https://doi.org/10.1016/j.ijid.2013.03.005
You M-J, Shin G-W, Lee C-S. Clostridium tertium Bacteremia in a Patient with Glyphosate Ingestion. The American Journal of Case Reports. 2015;16:4-7. doi:10.12659/AJCR.891287.
Miller D, Brazer S, Murdoch D, Reller LB, Corey, GR. Significance of Clostridium tertium Bacteremia in Neutropenic and Nonneutropenic Patients: Review of 32 Cases. Clinical Infectious Diseases. 2001; 32:975–8
-Casey Rankins, DO, is a 1st year Anatomic and Clinical Pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
The newest generation, Generation Z, is born in the 21st century. The oldest are now 18, which means that some have started entering the work force in entry-level positions. This generation is even more comfortable with technology than Millennials, as they grew up with computers, laptops, cellphones, internet and social media all around them.
The older Gen Zers are aware of the financial crisis that occurred, which created a strong focus on saving money. This generation was brought up with a sense of “Stranger Danger” so they are concerned with their own and public safety. They have a strong family orientation and consider themselves global citizens. They are characterized by an entrepreneurial spirit, the idea that anyone can be famous, are open-minded, and care deeply about the environment.
Because of the rising cost of education, many are worried about the price of college and about saving money for their parents. It is a little too early to tell because this generation is still young, but they could have feelings of unsettlement and insecurity due to the state of the economy, environment, and world. They are very loyal, compassionate and independent and have friends around the world, even if they have never traveled abroad themselves.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
I think we’re embarking on an incredible generation. I interviewed someone from each of our generations about how they observed, interacted with, learned from the Generation Zs. Here are their thoughts.
The Traditionalist: Ned the Grandpa
As the grandpa of two Gen Z grandsons, Ned found them to have an expanded knowledge base of the entire world. They are sophisticated in their analysis and critical thinking because of their exposure to information that their phones and computers provide them.
Lastly, they value human diversity far more than his own generation.
The Baby-boomer: Donna the Grandma
Donna is a “Grandma Boomer” and finds the Gen Z grandchildren’s vocabulary amazing. She says they are obsessed with the mechanical stuff and are used to doing 2-3 things at the same time. They still love sports, however, it’s like a class that they study. They attend practices but still play with their friends on their computers or phones. However, they “only” text. They don’t talk on the phone.
The Gen Z’s are far more sophisticated than the Boomers, yet they can’t write or spell as well as other generations. They don’t know cursive, and the first question they ask when going somewhere is, “do they have WIFI?” Oh, and “do you have a charger?”
Another Boomer: Susan the Grandma
Susan’s greatest concern was that many high-schoolers were being treated for levels of anxiety. Why? There’s no “turn off switch” with the world. They are almost required to stay tuned to respond or react to friends 24/7. Life is all about them from Instagram to Twitter, and Snapchat and tracking the number of followers.
The GenXer, Kim the Aunt
Her nephews are definitely focused on technology. They do not like talking on the phone and prefer to only text. They have incredible access to information, but they still like to play family games because they value tradition. Her nephews are great travelers and most comfortable with airports, planes and trains, Vs. just cars or bicycles. This is attributed to their expanded world. So what’s their greatest fear? A dead battery!
Maddie the Millennial
Maddie was shocked when she noticed that her sister, who is a Gen Z, was communicating via texting with her friend who was in the same room!
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.