Successful healthcare systems rely on strong, efficient and reliable pathology and laboratory services. In developed countries like the United States, the role of pathology and the lab in service delivery cannot be overemphasized. Through multidisciplinary tumor board conferences, the central role of pathologists in patient management has become more critical. This reality was further emphasized for me during a tumor board conference, where an oncologist wanted clarification on the difference between invasive ductal carcinoma with mucinous differentiation vs. mucinous carcinoma of the breast. I later learned that the distinction was necessary because of different prognosis and treatment. As pathologists, we work in concert with treating physicians which makes for more efficient and reliable patient care.
However, the situation is not the same in low to middle income countries (LMIC) where the pathology and laboratory workforce is currently suboptimal. One reason that has been attributed to this situation is a lack of awareness of the central role of pathology and lab medicine in developing countries with fragile health care systems. This has led to ineffective policy decisions and inadequate budgetary allocations to the lab, with the attendant catastrophic effects on patient care and outcomes.1
West Africa for example has seen a steady decline in healthcare delivery standards, even though diseases such as Burkitt lymphoma were first described in Africa, followed by the growth of the first human lymphoma/leukemia cell line (the Raji cell line).2 In addition, ‘Cancer in Five Continents’, a publication of the International Agency on Cancer Research, used data from Ibadan-Nigeria and Uganda cancer registries in its early years of publication. Unfortunately, during the years the countries in these regions have not been able to keep up with technologic advances that have since reshaped healthcare service delivery and research.3 Several barriers to sustainable pathology and laboratory services in LMIC have been identified including an inadequate workforce, substandard infrastructure, inadequate education and training, and quality assurance problems.1
Despite these challenges, there are opportunities to improve healthcare delivery systems in LMIC through effective laboratory and pathology services. One area that needs to be prioritized is the education and training of qualified pathology and laboratory personnel. This can be achieved through cross-cultural competency training and the building of collaborative networks through short term visitor exchange programs. In addition, continuing medical education (CME) opportunities should be made available to training institutions in these countries so they can keep up with modern day standards.
Another opportunity for growth in pathology and lab services in LMIC is through the implementation of accreditation and regulatory programs. These accreditation services should set standards by which lab services operate in these countries to ensure reliable and consistent operations. Such efforts may improve health service deliveries and ultimately improve patient outcomes.
One factor that has been a huge problem in disease prevention in LMIC is lack of adequate screening programs for chronic diseases, including several cancers. In many countries, misplaced priorities, in addition to lack of adequate personnel has been the bane of the healthcare systems. Therefore, policies that promote screening programs in LMIC should be prioritized. This strategy if implemented properly could lead to significant improvements in the healthcare systems, which would ultimately have an impact on patient care.
Furthermore, collaborative healthcare should be prioritized. The care and management of patients should be done collaboratively through clinicians across different specialties with proper communication channels in place. There have been instances where a clinician treating a patient may not have access to laboratory results requested by another clinician, which ultimately impacts the outcome of patients.
The role of efficient and functional laboratory and pathology services in healthcare systems cannot be overemphasized. Systems which lack these services experience catastrophic patient outcomes and until local and international governments prioritize the labs in these low-resource settings, patient outcomes will continue to remain suboptimal.
References
Sayed S, Cherniak W, Lawler M, Tan SY, El Sadr W, Wolf N, Silkensen S, Brand N, Looi LM, Pai SA, Wilson ML, Milner D, Flanigan J, Fleming KA. Improving pathology and laboratory medicine in low-income and middle-income countries: roadmap to solutions. Lancet. 2018 May 12;391(10133):1939-1952. doi: 10.1016/S0140-6736(18)30459-8. Epub 2018 Mar 15. PMID: 29550027.
Pulvertaft JV. Cytology of Burkitt’s Tumour (African Lymphoma). Lancet. 1964 Feb 1;1(7327):238-40. doi: 10.1016/s0140-6736(64)92345-1. PMID: 14086209.
Adeyi OA. Pathology services in developing countries-the West African experience. Arch Pathol Lab Med. 2011 Feb;135(2):183-6. doi: 10.1043/2008-0432-CCR.1. PMID: 21284434.
-Evi Abada, MD, MS is a Resident Physician in anatomic and clinical pathology at the Wayne State University School of Medicine/Detroit Medical Center in Michigan. She earned her Masters of Science in International Health Policy and Management from Brandeis University in Massachusetts, and is a global health advocate. Dr. Abada has been appointed to serve on the ASCP’s Resident’s Council and was named one of ASCP’S 40 under Forty honorees for the year 2020. You can follow her on twitter @EviAbadaMD.
It’s a little deja-vu writing this title one year after a similar blog post on how to validate a COVID-19 assay at the start of the pandemic. In many ways, the challenges are similar: limited reagents/control material, and rising case counts. At least now, there is increasing support in the way of funding from the federal government that could help with monitoring and surveillance. I’m going to summarize the current methods available for detecting the Variants of Concern and emerging variants.
Whole Genome Sequencing
The principle method used by many is whole genome sequencing. It has the advantage of being able to comprehensively examine every letter (nucleotide) of the SARS-CoV-2 genome (30 kilobases long). At our institution, I’ve been working on the effort to sequence all of our positive specimens. While it is achievable, it is not simple nor feasible at most locations. Limitations include:
Financial: must already own expensive sequencers
Expertise: advanced molecular diagnostics personnel needed who perform NGS testing
Data Analytics: bioinformatics personnel needed to create pipelines, analyze data and report it in a digestible format.
Timing: the process usually takes a week at best and several weeks if there is a backlog or not enough samples for a sequencing run to be financially viable.
Sensitivity: the limit of detection for NGS is 30 CT cycles, which for us includes only about 1/2- 1/3 of all positive COVID19 specimens.
Bottom line: WGS is the best at detecting new/ emerging strains or mutations when cost/ time is not a concern.
Mutation Screening
Other institutions have begun efforts to screen for variants of concern by detecting characteristic mutations. For instance, the N501Y mutation in the spike protein is common to the major Variants of Concern (UK B.1.1.7, Brazil P.1, and S Africa B.1.351) and E484K is present in the Brazil (P.1), S Africa (B.1.351) and New York Variant (B.1.526). Thus, several institutions (listed below) took approaches to 1) screen for these mutations and then 2) perform WGS sequentially.
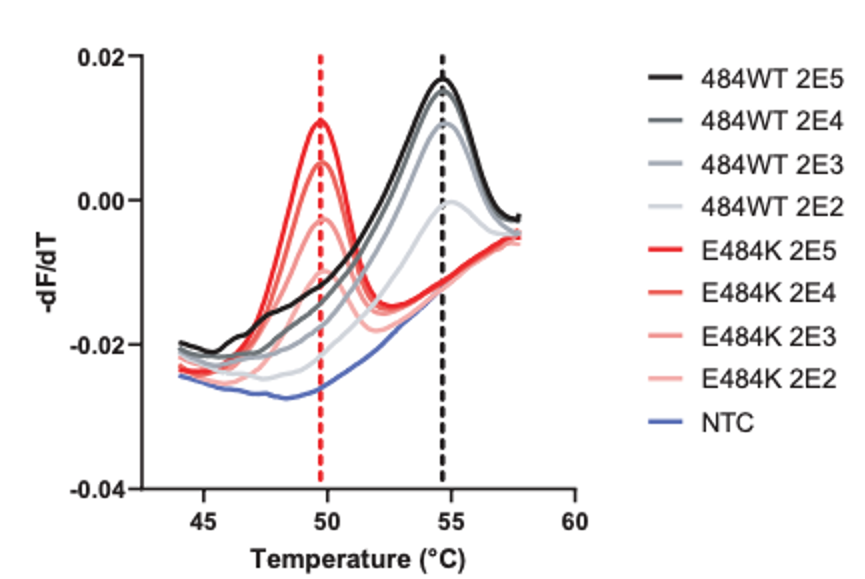
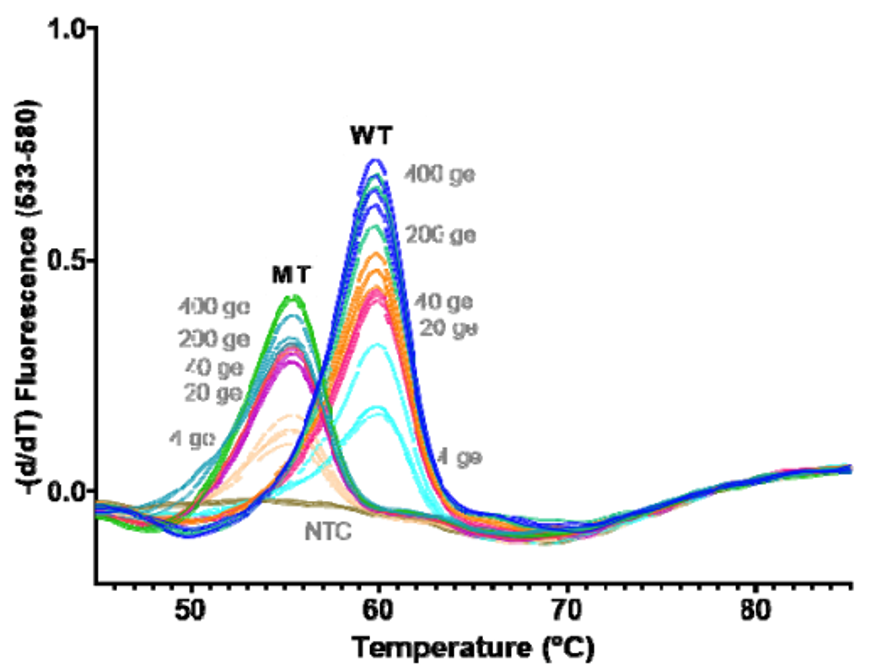
As you can see, HMH, Rutgers and Vancouver are using assays that use probes specific to characteristic alleles combined with melting temperature curves to detect a mutation induced change. Melting curve analysis is normally performed after qPCR to ensure that a single, correct PCR product is formed. This measure is calculated based on the change in fluorescence that occurs when the fluorescent marker is able to bind to its target DNA. Thus the Tm (melting temperature) is similar to the annealing temperature. In this case where a mutation is present in the probe (DNA fragment) binding site, binding is disrupted and occurs at lower a temperature as seen by the downward shift of 5 degrees Celsius in the graph below.
Figure 1. Schematic showing the melting temperature shift for the HMH designed probe binding normal and mutant (E484K variant) sequences at decreasing concentrations.Figure 2. Similar shift downward in melting temperature for the Rutgers assay when a wild type probe encounters a mutant vs. WT sequence.
These approaches are quick, but can only perform a 2-3 reactions per well and require much of the same expenses as diagnostic RT-qPCR assays. Most of the studies describe this method as a way of screening for samples to be NGS sequenced, however they will not be as good at detecting emerging strains. For example, the N501Y mutation is not present in the New York nor California variants.
Multiplex RT-qPCR can solve some of these problems. At Columbia and Yale, multiple targets are designed to detect B.1.1.7 (N501Y only at Columbia and S144del + ORF1A del at Yale) vs. Brazil/ S. Africa variants (N501Y & E484K at Columbia and ORF1A only at Yale). As new variants have arrived, we found the New York strain carrying both ORF1A deletion and the E484K mutation. It is now clear there are some hotspot areas for mutation within the SARS-CoV-2 genome, which can complicate interpretations. Therefore, these RT-PCR assays are still useful for screening, but do not replace the need for Whole Genome Sequencing.
Genotyping
Given the overlapping spectrum of mutations, it would be helpful to test several markers all at once in a single reaction. At a certain point, this would effectively “genotype” a variant as well as WGS. The assays above have been limited to 2 targets/ reaction due to limited light detection channels. Therefore, I’ve created a multiplex assay that can be scaled up to include 30-40 targets within a single reaction without the need for expensive probes. This method is multiplexPCR fragment analysis, which is traditionally used for forensic fingerprinting or bone marrow transplant tracking. In this method, DNA of different length is amplified by PCR, then separated by capillary electrophoresis-the same instrument that performs Sanger Sequencing.
Fragment analysis can be performed to detect deletion/ insertion mutations and single nucleotide polymorphisms (SNPs) by allele-specific primers or with restriction enzymes that only cut the WT or Mutant sequence.
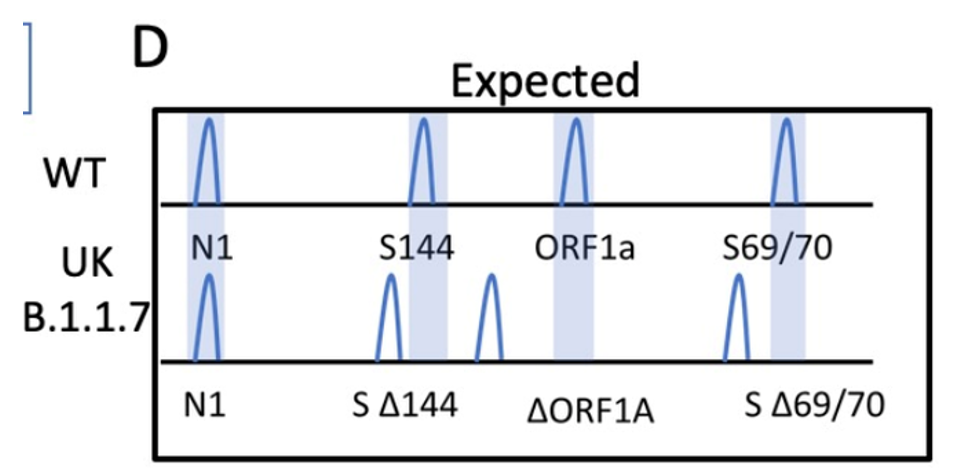
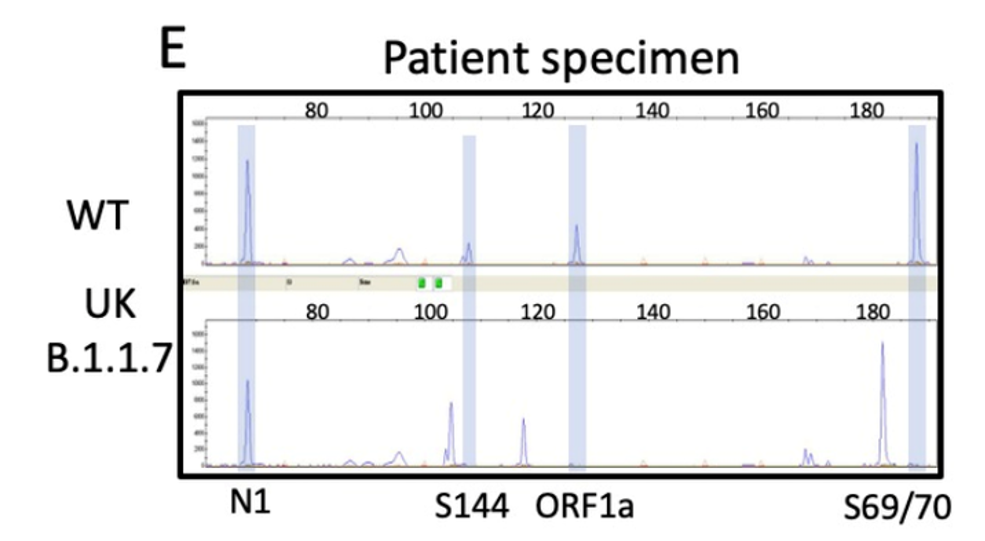
I designed the assay to target 3 deletion mutations in B.1.1.7: S:D69_70, S: D144, and ORF1A: D3675_3677. Each deletion has a specific length and if 3/3 mutations are present, then there is 95% specificity for the B.1.1.7 strain. Samples from December to present were tested and in the first batch, I detected the characteristic B.1.1.7 pattern (expected pattern and observed pattern below).
Theoretical picture of what the fragment analysis assay would look like for B.1.1.7. An actual patient sample results below, which showed the expected deletions exactly as predicted:
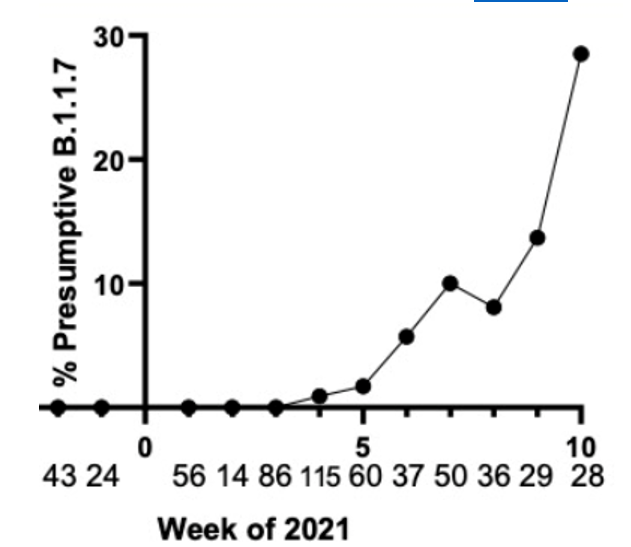
We have tested and sequenced over 500 positive specimens, and we found increasing levels of the B.1.1.7 strain prevalence up to nearly 30% by the middle of March. All screened B.1.1.7 specimens were validated by WGS. These results and the ability to detect the New York and California variants are detailed in our recent pre-print.
Weekly prevalence of isolates consistent with B.1.1.7 in North Texas.
Implications for future Variant Surveillance
As B.1.1.7 has become the dominant strain, and sequencing efforts are increasing. I would argue that assays should be used for what they are best at. For instance, it could be considered a waste of NGS time and resources to sequence all Variants when >50% are going to be B.1.1.7 if other tests can verify the strain faster for 10-20% of the cost. Instead, I think WGS should be focused on discovering emerging variants for which it is best suited. Across the US, case numbers have been decreasing and the number of specimens testable could be expanded by using a more sensitive PCR assay that could.
–Jeff SoRelle, MD is Assistant Instructor of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX working in the Next Generation Sequencing lab. His clinical research interests include understanding how lab medicine impacts transgender healthcare and improving genetic variant interpretation.Follow him on Twitter @Jeff_SoRelle.
One of my favorite things about working in Hematology is handling those “difficult” samples. You know the ones. The one that some techs put aside to work on “later,” or they might decide it’s time to take a break when they see them coming. I love investigating and working on these interesting but perhaps uncooperative samples. At times this involves running samples in different modes, making new slides or albumin smears, and diluting samples. At other times, we investigate a delta or unusual results by checking patient diagnosis and previous results or by calling the care provider for more information and clues to help us resolve the problem.
I’m sure you’ve all seen the sayings “Without the Lab, you’re only guessing” and “Laboratory Professionals get results.” Physicians rely on the lab every day for information used to help diagnose and treat patients. Therefore, our goal is to deliver to the care provider the best possible results in a timely manner. Which means that we don’t just report results because that’s the answer the instrument gave us. With today’s instruments and middleware, we get very accurate and precise results, and about 85% or more of hematology specimens autovalidate. This is important because it leaves us time to work on those specimens with flags, and discrepancies; the ones that need a little more time and attention.
When faced with unusual or conflicting results, we first need to ask ourselves if we are dealing with a spurious sample, interfering substances or true abnormal results. Many labs today use middleware that will give the operator alerts when a sample needs to be investigated. These alerts give us suggestions as to how to handle the specimen but are usually short phrases triggered by certain values or flags and cannot be all encompassing. Operator alerts cannot tell us all the steps we may need to follow to resolve, for example, deltas, platelet clumps, abnormal scattergrams or a possible cold agglutinin. The alerts are great guidelines but it is often necessary to do more. We may need to refer to procedure manuals for SOPS or check instrument manuals or technical bulletins to decide how to handle these specimens. Sometimes we need to be detectives to report the most accurate results. We must review results with a critical eye, use all that “stuff” we learned in school, and be able to make educated decisions based on this investigation.
In my experience, one of the most common troublesome and perhaps misunderstood specimens I see is the one with a “hemoglobin (Hgb) interference” flag. An instrument flag “suspect, turbidity /Hgb interference?” is generally initiated when the MCHC is above a certain value. In our hematology lab, we see this flag when the MCHC is above 37.5 g/dL. What this is telling us is that turbidity may be present in the diluted and lysed sample. This turbidity can interfere with the Hgb detection light path and falsely increase the Hgb. Because the MCH and MCHC are calculated using the Hgb, these parameters are also affected. BUT, an MCHC >37.5 g/dL is not always something that can be or that needs to be corrected. With any parameter 95% of normal values will fall within 2SD of the mean. This means that 5% of normal healthy individuals have MCHC results <32 g/dL or >36 g/dL, and a few may have an MCHC over 37.5 g/dL. An MCHC >37.5 g/dL therefore can indicate a normal specimen, such as in a healthy young male with a Hgb at the high end of the reference range. High MCHCs can also be seen routinely in specimens from patients with spherocytosis or hemoglobinopathies such as Hgb SS, Hgb SC or Hgb C disease. In these conditions the RBCs are hyperdense due to altered surface volume and this leads to a high MCHC.
On our instrument, an MCHC >37.5 g/dL will cause a Hgb/Turbidity flag. An asterisk (*) will appear next to the Hgb, MCH and MCHC. The middleware triggers an operator alert that says “MCHC >37.5. Incubate at 37C for 30 mins. Evaluate for lipemia, icterus, hemolysis, Plasma replacement if indicated, rerun”. So, what’s the first thing to do?? Incubate? Hold on…not so fast. This is one of those instances where hematology is not just black and white. This operator alert is giving us suggestions of how to handle a specimen, but techs need to evaluate the specimen before jumping on the ‘cold’ wagon. Incubating will usually help resolve a cold agglutinin, but won’t help with a sickle cell specimen, or resolve one that’s icteric or lipemic. A grossly hemolyzed sample can give a spurious high MCHC result and, if so, needs to be recollected, not warmed. Putting a specimen that’s hemolyzed or lipemic or icteric in the heating block for 30 or more minutes would only delay reporting of results. My first case example involves a 45 year old female. The MCHC on initial run was 38.1 and the specimen gave a Hgb turbidity flag. The sample was incubated and rerun several times. After 1 hour of incubation, the MCHC was reported as 37.1 with a comment “repeated after warming for 1 hour at 37C”. In this case the patient was a known sickle cell patient. Previous results show that this patient’s MCHC is typically high and previously reported results ranged from 36.1- 37.8 g/dL. When evaluating a specimen with a high MCHC it is important to check the pattern of results. In this case the MCHC was high but the MCV was low. This does not fit the pattern for a cold agglutinin. As noted above, super dense RBCs in sickle cell patients may cause a high MCHC. This specimen was warmed, and even though the MCHC was a bit lower after warming, it would have been acceptable to report the original run MCHC. Checking patient history and previous results, and reviewing the smear for morphology would have allowed these results to be reported in a timely fashion. The operator alert does say “incubate the specimen” but it also says to evaluate. Be sure to check the MCV and MCHC along with patient history before warming specimens that don’t fit the pattern of a cold agglutinin.
Table 1. Case 1 CBC. The patient is a 45 year old known sickle cell patient.
The second example is from a 75 year old male. The CBC flagged Hgb turbidity with an MCHC of 45.8 g/dL. The MCHC >37.5 operator alert triggered Checking the pattern of results for the indicies, the MCHC was very high and the MCV was low. In a specimen with a low or normal MCV and a high MCHC, lipemia, icterus, abnormal proteins or severe leukocytosis can be affecting the Hgb. On evaluation, this sample’s Hgb and Hct did not meet the ‘rule of 3’. The rules of 3 are now generally recognized to be valid only for samples when the RBCs are normal, but the * here is telling us that there is an interference affecting the Hgb. In these cases it is valuable to know what the interference is so we know how to handle the specimen. By spinning down a small aliquot, (or asking chemistry!) we can investigate for lipemia or icterus. The specimen was found to be grossly lipemic. Flagging guidelines for lipemic specimens suggest diluting the specimen 1:5 and rerunning. Alternately, with severely lipemic or icteric samples, plasma replacement procedure may be necessary to correct the results. In this case, a plasma replacement was performed. After a plasma replacement, the WBC, RBC, Hct, MCV and platelet count are reported from the original run. The Hgb interference is what was causing the problem. Thus, when you correct the Hgb you must always correct any indicies that are calculated with the Hgb. The Hgb from the plasma replacement sample is used and the MCH and MCHC are recalculated. Notice that the new lower Hgb value now matches the Hct.
Table 2. Case 2, a 75 year old male with lipemic specimen. Plasma replacement performed. WBC, RBC, Hct, MCV, and Plt were reported from original run. Hgb was reported from plasma replacement sample. MCH and MCHC were recalculated.
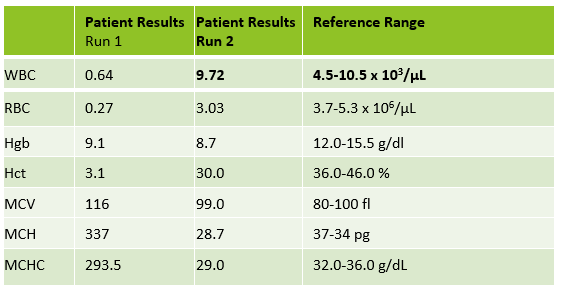
Case 3 is a sample from an 80 year old woman. This was an interesting sample because there were multiple things going on here. This patient had an initial result with a high MCHC and MCH, with decreased RBC and Hct. In this patient the initial WBC was 0.64 and the RBC was 0.31. The Hgb of 9.1 /dL was less than the Hct of 3.1 %. MCV was 116 fl and the MCHC was 293.5 g/dL! In specimens with a high MCV and high MCHC we can suspect a cold agglutinin. When the MCV is very high it is because the RBCs are going through the aperture as one big bunch and this is measured as the size of one RBC. Often the Hct is less than the Hgb. Sometimes the RBC and Hct are so low that it causes the MCV to be appear within normal range. On our instrument, a RBC count of <0.5 x106/μL will give a flag “abnormal RBC scattergram” but no other indicies related flags are generated, so we didn’t even get an operator alert to evaluate the MCHC. But, it’s clear there is something very wrong with these results. Warming the sample is used to loosen clumping of RBCs, which lowers the MCV and allows the RBCs to be counted. Make a smear to examine for RBC clumping and look at the sample tube. Many cold agglutinin samples will appear to be ‘grainy’ or have agglutination along the side of the tube. This is the time when we want to incubate the sample. To resolve a cold agglutinin, warming the sample is necessary. Sometime 30 minutes is enough, sometime they need to be incubated longer. Some cold agglutinins are so strong that after incubation a dilution or plasma replacement still needs to be done. Warming this sample did not lower the MCHC. After incubating, I diluted this sample, and also did a plasma replacement to see how results would compare. The new results matched. This sample took a bit more time than others but the cold agglutinin was resolved and we were able to report valid results.
Table 3. CBC results from 80 year old woman with cold agglutinin. Image 1. Tube from cold agglutinin specimen. Note agglutination in sample along sides of tube.
There are other factors that can affect the Hct or Hgb and cause a high MCHC. Icteric specimens act much like lipemic ones and the Hgb can be corrected with dilution or a plasma replacement. An electrolyte balance can affect the Hct. Abnormal proteins and severe leukocytosis can affect the Hgb. Grossly hemolyzed samples can have a high MCHC. It is important to evaluate the indicies in these samples and correlate the values with previous results and patient history. What concerns me is that I have seen samples being warmed that do not match the indicies patterns for cold agglutinins. I have seen samples from sickle cell patients signed out with a comment “warmed at 37C. Possible cold agglutinin.” I have seen lipemic or icteric samples that are reported out with high MCHCs, erroneously high Hgb or parameters that are not reported at all. While warming these samples may actually lower the MCHC a bit, it still usually remains on the high side and does not give us the clean results that dilution or plasma replacement will. A little extra time looking at the indicies can give us important clues as to how to handle these samples. Doctors use our results every day to make patient care decisions. We need to make sure that we are making decisions every day to give them the best possible results so that patients can get the best care possible.
Table 4. Evaluating high MCHC specimens.
References
Costa, B. M. B., Vellés, M. C., Viana, M. M. F. B., & Rebelo, C. I. M. (2018). Interference of cold agglutinin autoantibodies in erythrogram interpretation: a case report and literature review. Jornal Brasileiro De Patologia e MedicinaLaboratorial, 54(4). doi: 10.5935/1676-2444.20180043
Sysmex USA. XN-Series Flagging Interpretation Guide. Document Number: 1166-LSS, Rev. 6, March 2021
It’s not Black and White: Unraveling the puzzles of Hematology. Becky Socha MS, BB, MLS(ASCP) Mercy Medical Center, Baltimore, MD
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A 59 year old female initially presented with DCIS, treated by mastectomy and 5 years of adjuvant tamoxifen at another institution. 4 years later, she presented to another hospital with an adrenal mass, uterine fibroids, and an ovarian cyst, where a biopsy and right-sided adrenalectomy confirmed a 10.5 centimeter adrenocortical neoplasm. Margins were close, but negative at <0.1 cm. Microscopically there were areas of necrosis, high nuclear grade, a diffuse growth pattern, and clear cells representing less than 25% of the tumor. A malignancy was favored, but lack of metastasis could not confirm the diagnosis. She presented to the cancer center with stage II adrenal cancer, T2N0M0 and mitotane-induced adrenal insufficiency. Multiple hepatic and pulmonary metastases were subsequently identified and treated with extensive surgery, including a VATS wedge resection, right nephrectomy, hepatic mobilization, lysis of adhesions, dissection of the adrenal vein and vena cava with repair, and resection of an ileal mass.
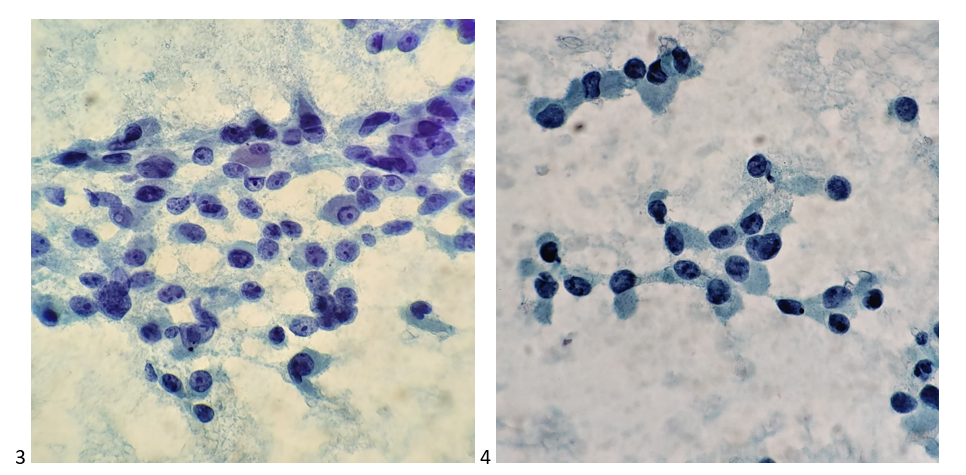
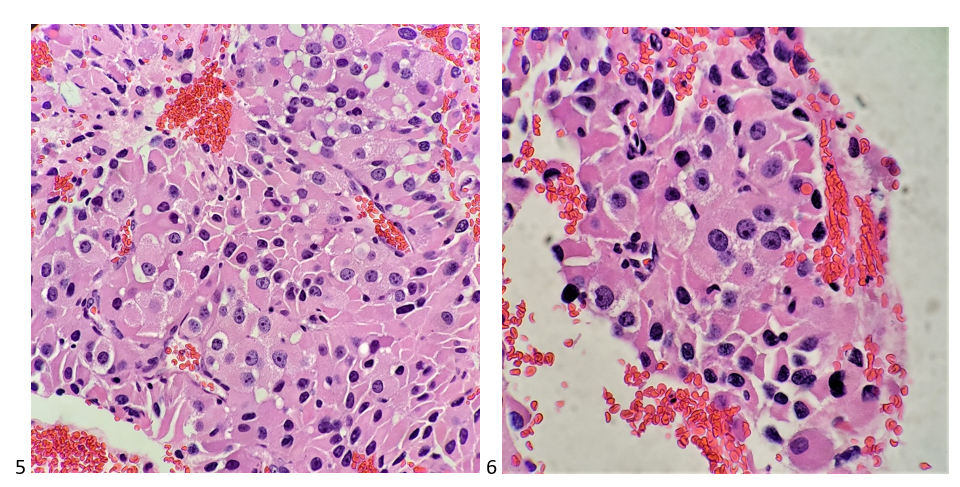
Palliative radiation therapy targeted the remaining lung nodules, and six cycles of chemotherapy were administered. A CT scan-guided fine need aspiration biopsy was obtained of a 4 centimeter retroperitoneal mass that was suspicious for recurrence on imaging, which cytopathology then confirmed. Taking into consideration the history, my additional differentials included renal cell carcinoma, hepatocellular carcinoma, and plasmacytoma, with metastatic breast cancer as the least likely differential.
Images 1-2. Retroperitoneal mass, right side, FNA-DQ stained smears. Images 3-4. Retroperitoneal mass, right side, FNA-Pap stained smears. Images 5-6, Retroperitoneal mass, right side, FNA-H&E cell block sections.
Palliative radiation therapy was then administered to the retroperitoneal and psoas masses, and microwave ablation targeted the segment 3 and segment 6 liver lesions, reducing pain and stabilizing growth, respectively. However, disease continued to slowly progress, so the oncology team sent the retroperitoneal metastasis tissue for molecular testing to assess for potential next lines of therapy. Testing revealed a variant of undetermined significance in MSH6, indeterminate tumor mutational burden, stable MSI, and negative for PDL1. When the case was brought to tumor board, the team recommended ongoing surveillance and palliative therapy (when needed) given the patient’s slowly progressing disease. Often thought of as a rare disease, I’ve examined a fair share of primary and metastatic adrenocortical carcinomas through working at a cancer center. These tiny triangular glands that sit on top of the kidneys have SO much power. Producing and regulating cortisol, aldosterone, and androgenic hormones, the adrenal cortex is an active outer layer. Whether hormonal or neoplastic, it truly is fascinating how a tiny gland could wreak so much large-scale havoc on the human body.
-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
A 55 year old male with a 43-pack-year smoking history was transferred to our hospital for evaluation of new onset neurologic deficits including slurred speech, aphasia, and right upper extremity diminished dexterity and neglect. CT chest was remarkable for a mass in the superior segment of the left lower lobe. Needle core biopsy of the lung mass revealed poorly differentiated non-small cell carcinoma. Head MRI demonstrated an enhancing mass in the left frontoparietal junction that was concerning for metastasis from a lung primary. The patient was started on chemotherapy as an outpatient. Follow-up imaging showed growth of the brain mass. A biopsy of the brain mass showed no evidence of metastasis, only “reactive brain with foci of dense mixed inflammation and filamentous bacteria consistent with abscess.”
Image 1. Head MRI demonstrating left frontoparietal mass.
Laboratory Findings
A portion of the brain biopsy was submitted for bacterial smear and culture. The aerobic culture grew chalky white colonies that, when stained with modified acid-fast stain, showed modified acid-fast positive filamentous bacteria, suspicious for Nocardia spp. Bacteria of similar morphology were also seen in the surgical pathology specimen when stained for modified AFB and with GMS.
Image 2. Blood agar plate growing chalky white colonies. Image 3. Modified acid-fast positive filamentous bacteria at 1000x.
Disscussion
Nocardia is a genus of aerobic, catalase positive, saprophytic bacteria often found in the environment, but that can also be considered as normal flora on skin and in the respiratory tract. Nocardia species are variably acid-fast; for proper identification they must be stained with a modified acid-fast procedure (Fite, Kinyuon), using a weaker decolorizing acid. Nocardia will be negative by traditional acid-fast staining procedures (Ziehl–Neelsen). When Gram stained, Nocardia will appear as branching filamentous gram-positive bacilli with a “beaded” staining pattern (as if a string of beads).
Multiple species are considered human pathogens, including N. asteroides, N. brasiliensis, N. cyriacigeorgica, N. farcinica, and N. nova. These organisms can cause disease in immunocompromised patients if inhaled or inoculated via trauma. If there is an established pulmonary infection, Nocardia may spread hematogenously, often infecting the brain.
Central nervous system nocardiosis may occur in any region in the brain and can present with mass effect symptoms without typical infectious symptoms, as in our patient. Prognosis varies based on the extent of disease and the cause of a patient’s immunosuppression. Treatment of CNS nocardiosis usually begins with an induction phase of intravenous TMP-SMX and imipenem for 3-6 weeks or until there is clinical improvement. Once the patient improves, they can be switched to oral therapy with a sulfonamide and/or minocycline and/or amoxicillin-clavulanate.
References
Beaman BL. Nocardia Species : Host-Parasite Relationships. 1994;7(2):213-264.
Spelman D. Clinical manifestations and diagnosis of nocardiosis. In: Sexton DJ, Mitty J, eds. UpToDate. UpToDate, Inc.
Spelman D. Microbiology, epidemiology and pathogenesis of nocardiosis. In: Sexton DJ, Mitty J, eds. UpToDate. UpToDate, Inc.
Spelman D. Treatment of Nocardiosis. In: Sexton DJ, Mitty J, eds. UpToDate. UpToDate, Inc.
-Michael Madrid, MD is a 1st year Anatomic and Clinical Pathology Resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
Many years ago I worked in a lab that often received dry ice in boxes with our blood product deliveries. The habit in the lab was to dump the excess frozen carbon dioxide into one of our stainless steel sinks. The staff would get excited each time there was a delivery because they liked to run tap water onto the ice to make a “waterfall” of smoke flow onto the floor when they were bored. Before too long, this repeated incorrect placement of dry ice resulted in severe damage to the sink and pipes below. The stainless steel basin cracked and the sink fell down onto the broken pipes below. That particular plumbing is not designed to handle such a low temperature, and the repair was not cheap. Luckily, no one was injured. I thought this was a long-dead practice in labs, but even today I get questions about proper dry ice disposal and am asked whether or not the sink is a good spot for that.
Dry ice sublimates at room temperature. That means it transforms from a solid state directly into a gas. Too much of this gas in a small space will reduce the normal oxygen levels in the area, potentially causing dizziness and asphyxiation. Letting dry ice sublimate in the work place can be a dangerous practice. If you have dry ice to dispose of, the best practice is to set it outside (where other could not have access to it) so it can dissipate into the open air.
Dry ice is often used in the transport of specimens, blood products, and certain lab reagents. The Department of Transportation considers it a dangerous good, and it must be used and labeled specifically if it is to be shipped by land or by air. If dry ice is used in shipping, an additional Class 9 miscellaneous hazard label also must go to the right of the Class 6.2 infectious substance label. In addition to the Class 9 label, the outer box must be labeled with the net quantity of dry ice used.
Another common use of dry ice is with the transport of outreach or clinic lab samples in courier vehicles. Certain samples must be kept frozen for testing, and the use of dry ice provides a convenient method for maintaining the necessary temperatures. Dry ice is placed in a cooler in the courier vehicle, and samples are placed until delivery to the reference laboratory. With that, there are specific safety practices that should be adhered to when using dry ice for this purpose. Couriers are often overlooked when considering safety training, but they are an important piece of the lab sample and testing process. Be sure couriers have complete safety training, including training for the proper handling of dry ice.
Couriers should limit the amount of dry ice placed inside the cooler that will rest in the vehicle. No more than three pounds of dry ice should ever be placed in that cooler. The cooler should never be completely sealed (remember the ice sublimates to gas, and the volume of the gas in the cooler will expand). Also, if dry ice is kept inside of a vehicle, the windows should be left opened, even a tiny bit. There have been incidents where too much dry ice in a closed vehicle has caused a driver to become dizzy or even become unconscious. Obviously, this is a potentially dangerous or even deadly situation and should be avoided completely.
In recent years, the College of American Pathologists (CAP) added new regulations for labs that handle dry ice. These safety rules include the use of appropriate (insulated or cryogenic) gloves and a face shield when handling dry ice. Safety Data Sheets should be available and staff who use dry ice must have documented training. CAP also discusses the need for using dry ice only in well-ventilated areas.
In the laboratory or outreach settings, employees are asked to work with many dangerous substances, bloodborne pathogens, chemicals, and sometimes dry ice. Inherently, these departments are not safe, but OSHA requires that employees be able to work safely in those places, and it can be done. Proper training and oversight of safety are the keys to ensuring your employees can collect, transport, and process lab samples in such a way in which all involved in these processes are kept safe.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
The current pandemic has highlighted the importance of the laboratory in the delivery of healthcare. Patients and families depend on the laboratory to delivery accurate and timely results. Regulations have been written to ensure laboratories meet society’s expectations. Medical laboratories are one of the most highly regulated industries requiring biennial inspections by accrediting agencies. Despite operating under the COVID-19 testing pressures, laboratories still need to be inspection-ready.
New Inspection Process
As a result of social-distancing mandates and state-level restrictions, laboratories need to adjust to a new inspection environment. The College of American Pathologists (CAP) is temporarily allowing virtual inspections and has created information on its website about a few laboratories’ experiences with the virtual inspection process.
The CAP has also shared some expectations laboratories should be aware of when discussing inspection aspects.
Currently, in states where there are travel restrictions with quarantine requirements, a greater than 5% positivity rate, or where the institutions have travel/visitor restrictions, the laboratory medical director may choose to have a virtual inspection. However, the laboratory should be aware that they will still be required to have an in-person on-site inspection within 4-6 months if virtually inspected.
In addition, the laboratory director and the inspection team must both agree to perform a virtual inspection.
Virtual Aspects
Laboratories should take into consideration some of the aspects of a virtual inspection. In-person inspections for many small to medium laboratories often consist of inspectors being on-site for only one day. Conversely, virtual inspections can be weeks or even a month in duration depending on the laboratory’s size, the number of specialties, and the inspectors’ availability.
Virtual inspections also require a lot of document handling. Laboratories utilizing manual worksheets, quality control and troubleshooting logs will need to upload these documents for review. The CAP has created a secure website for this purpose, but it still requires personnel to scan each document individually.
Technical Priorities
There is also the risk of technical issues hampering the virtual process. Laboratories must have reliable Wi-Fi, electronic communication devices (laptops, tablets, cameras) and have personnel comfortable with the challenges inherent in managing multiple requests simultaneously. Having a dedicated IT person for an inspection is a great but difficult to get asset.
Mult-day Inspection
If there are no limiting COVID restrictions, laboratories may still opt for an in-person inspection.
Some inspection teams (in agreement with the laboratory medical director) have modified the in-person inspection process so that it is conducted over a 3-4 day time period. In this process, only a few inspectors come on each day to inspect specific disciplines. Usually, one inspector will return the next day to provide some continuity to the inspection process.
Instead of an intense one-day process, spreading an in-person inspection out to 3-4 days allows the team and facility to practice social distancing, reduces the level of stress, and gives the laboratory more time to provide evidence or have a deficiency changed to “corrected on-site.”
Competency Note
Laboratories need to be reminded that regardless of COVID, the requirements for competency still apply. New hires must still have semi-annual competencies performed at the required frequencies, and the laboratory must be able to provide competency documentation during an inspection. There are no exceptions to the competency mandate.
Conclusion
It is expected laboratory administrators and managers may have a bit of angst regarding the uncertainty that comes with a new inspection process affecting the entire laboratory. Amid the COVID crises, the laboratory has been tasked to deliver high-quality results efficiently. Laboratories across the nation have met the COVID challenge and are able to adapt to the demands inspections require. Virtual inspections are just another example of the laboratory adapting to meet its regulatory and accrediting requirements.
-Darryl Elzie, PsyD, MHA, MT(ASCP), CQA(ASQ), has been an ASCP Medical Technologist for over 30 years and has been performing CAP inspections for 15+ years. Dr. Elzie provides laboratory quality oversight for four hospitals, one ambulatory care center, and supports laboratory quality initiatives throughout the Sentara Healthcare system.
Laboratorians struggled through 2020 but successfully navigated a difficult situation while maintaining and improving our high-quality service to our patients. By laboratorian, I mean all of us—medical, public health, research, industry, etc.—because, across all sectors, anyone working in a laboratory (our family) was pushed to the limits to do more with less, work harder with fewer people, provide results with challenging procedure standard, and save lives while risking our own. It is quite easy to go into a clinical laboratory that is providing COVID-19 testing and find heroes that were there before, excelled during this pandemic, and will be there tomorrow. But there were heroes in every laboratory. Our public health laboratorians spent tireless hours trying to provide testing, coordinate testing, disseminate information, and relay the best current epidemiology to leadership to keep the country running. Our research laboratorians developed and delivered data, new information, novel biology, and potential interventions for the novel coronavirus. Our industry laboratorians were crucial components to vaccine development and delivery. And, unlike most of the country, our laboratorians were not able to “work from home” because, well, there are laws against having certain things in your house that might escape and kill your neighbors. It is good to be essential, but it has it pain points. Our laboratorians have felt that pain by still commuting to their benches to get the work done every day. But they did it and did it well! And what is often forgotten is that every single one of these laboratorians already had a “day job” in delivering a full catalog of laboratory-based services to which they added a successful COVID-19 response. If you see a laboratorian after you read this blog, you should want to hug them and say thank you.
Vaccination is spreading and will overtake and conquer this virus in parallel with our continued social distancing, hand washing, and mask wearing. In the background, testing will continue and will drive how our leaders make decisions more than anything else. We can see an end to this bedlam and are now facing, perhaps, one of the most difficult questions we have ever faced as a global laboratory community: “What do we do now?”
Our pathologists, long awaiting the day when digital telepathology was the norm, were thrust headfirst into that practice during the pandemic under emergency conditions. Many of them had already started (sometimes in a big way) but others were pushing glass routinely. Many of us have leapfrogged to a place from which we cannot return. We need to evaluate the virtual practice of the past year to determine the error rates and see if it is comparable (or better) than our routine glass slide practice. Is eBay or LetGo going to be overwhelmed with microscopes while high resolution monitors go into backorder? We must still contend with the requirement of “presence” and the moniker of “CLIA”, which was temporarily separated from a pathologist’s role in care during the pandemic. These new digital practices may address our long-standing workforce shortages. Working from home was not a possibility but a requirement for much of the last year. Care continued and work was done. What evidence would argue that working in an office is “better” than working from home when we consider the practice of pathologists? The financial implications of cost per square foot of overhead when taking up space in an academic medical facility is more than sufficient for a CFO to argue that pathologists working from home is great. But this is assuming that the workstation, the workflow, and the outputs were optimized. Not all pathology laboratories went fully digital and there was a great deal of slide shipping/couriering. On the other side of this pandemic, much like the 6 to 10 different platforms found in a clinical lab to perform a COVID-19 test, we will find that many practices are not sustainable, can be replaced and optimized, and will require more upheaval and pivot from our pathologists. To clarify, before COVID-19, pathologists practiced basically the same anywhere in the world; namely, review of glass slides in slide folders with a connected case file. During COVID-19, a whole new set of options emerged for how we would do that routine work that were uncontrolled and ad hoc. Now on the other side, we must separate the practices that are best for patient care from those that got the work done in a crisis to find our way forward. If the optimal model is (and I am not saying that it is) digital telepathology from anywhere, we must work hard to define “anywhere” for the sake of our patient’s care and safety. Monitor or other devices standards, which have long been the bane of the telepathology community, are still not standards. CLIA is specific about what constitutes a laboratory and its four walls. Accreditation teams do not inspect people’s home offices. On the other side of this pandemic, how do we find a common, best practice in a virtual age? We must return to a state of highest possible quality for our patients without giving up the advances we made in this crisis.
I once wrote up a laboratory revision plan for a firm that had 9 hospitals. Each had its own pathology laboratory employing 1 to 3 pathologist and similar staff for grossing, histology, and admin. Each laboratory had a volume of less than 3000 samples per year (and referred complex cases to a tertiary care center out of network). Based on our revision, in formalin concentration and recycling alone, the system would save $100,000. With a centralized laboratory (easily capable of handling 30,000 samples per year) and a digital pathology strategy, the work could be done by half the number of pathologists. Most importantly, the reagent/supply savings from having one laboratory rather than 9 was astronomical. The bottom line was an increase in revenue of nearly $1,000,000 with a cost savings of more than 75%. The key element of this plan that is important here is the digital telepathology component that reduces the number of staff needed and the office space needed which, at the time of the revision proposal, was “innovative” but thought too new to be reasonable. COVID-19 has tested that one aspect of the model and found it to be more than reasonable. More importantly, laboratory management and organizational leadership has had to take a hard look at costs, cost centers, and fixed expenses in such a way that the model above now becomes not lucrative but essential to staying in operation. We are trained in the laboratory to always be working on quality improvement, but COVID-19 has pushed us to always be working on fiscal improvement as well.
As we return to our “new normal” after COVID-19, the lessons we learned from this pandemic are going to translate into mergers, acquisitions, consolidations, closings, and restructurings of all types of businesses and services with the laboratory being no exception. The concept of surge capacity, for example, for testing of a new infectious agent that has emerged, has been a trial by fire, and there are many important lessons to learn from this as well. Should our approach to the next pandemic be to divert our staff from regular laboratory operations and bring into our facilities 6 to 10 new platforms for testing? Perhaps we should consider using temporary warehouse space offsite from our existing laboratory as well as backfill or relocating staffing for this crisis management to prevent complete disruption of our workflow and our policies. This is the type of solution that can exist when contingency planning is a routine part of operations. Those many facilities that were forced to bring in extra platforms are going to be facing a different crisis as test volumes crash; namely, what to do with the equipment. The firms that produce and sell that equipment have a similar challenge of expanding their platform beyond COVID-19 testing and making it relevant and competitive for the laboratories that have their extra platforms. Although I am not sure eBay or LetGo will be full of microscopes just yet, I am sure you are going to be able to pick up some nifty analyzers for an incredibly low price very soon. Will the memorial to the half-a-million we have lost in this country to COVID-19 be the useless bodies of laboratory devices that we so desperately needed in 2020? I think we owe them a lot more than that. Let us actively rethink our strategies in the laboratory and across our healthcare system so that such memorials are never needed again.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
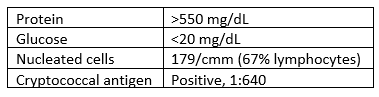
A 53 year old male with a past medical history significant for dermatomyositis, antisynthetase syndrome, and atrial fibrillation with rapid ventricular response presented with a chief complaint of worsening confusion, auditory hallucinations, and hearing loss. Pertinent medications included prednisone and mycophenolate. Head MRI demonstrated leptomeningeal enhancement and hydrocephalus. A lumbar puncture was performed, with CSF results as follows:
Laboratory Findings
CSF was sent to the microbiology lab for bacterial and fungal smears and cultures. No organisms were seen on the Gram stain.
Within 3 days, however, rare colonies of yeast were growing on both the bacterial and fungal media. The yeast was identified as Cryptococcus neoformans using the in-house MALDI-TOF mass spectrometry instrument.
Image 1. Budding C. neoformans at 1000x. Image 2. Colonies of C. neoformans on potato flake agar.
Discussion
Cryptococcus neoformans is an environmental saprophytic yeast that can be found around the world, although it is often associated with avian droppings.1 The cell is surrounded by a polysaccharide capsule that protects it from environmental hazards and, once within the host, from phagocytosis.2 Additionally, the cell wall of C. neoformans contains melanin due to the presence of the phenol oxidase enzyme, which assists in the formation of melanin from various phenolic substrates.1 Both the polysaccharide capsule and the melanin-containing cell wall can be helpful in the laboratory identification of C. neoformans.
If inhaled, Cryptococcus neoformans can cause disease (cryptococcosis) in immunocompromised patients. The most significant risk factor is AIDS, however any cause of immunodeficiency can be a risk factor, including long-term steroid therapy, organ transplantation, malignancy, and liver disease.1 Once inhaled, the organism spreads hematogenously and tends to favor the central nervous system, causing cryptococcal meningoencephalitis.1
Prognosis for patients with cryptococcosis can vary widely. In AIDS-associated CNS cryptococcosis, predictors of mortality include abnormal mental status, cerebrospinal fluid antigen titer >1:1024 by latex agglutination or >1:4000 by lateral flow assay, and CSF white blood cell count <20/µL.1 The prognosis for patients who are immunocompromised for other reasons depends on the cause of their immunosuppression.1
Treatment of patients with cryptococcal meningoencephalitis consists of an induction phase with amphotericin B and flucytosine followed by a consolidation phase with fluconazole then a long-term maintenance phase with a smaller dose of fluconazole.3
References
Jobson M. Microbiology and epidemiology of Cryptococcus neoformans infection. In: Post T, ed. UpToDate. UpToDate, Inc. Accessed March 13, 2021. https://www.uptodate.com
Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2010;50(3):291-322. doi:10.1086/649858
-Michael Madrid, MD is a 1st year Anatomic and Clinical Pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.