2019 marked a very special year for me as I had the incredible opportunity to interview some of the most remarkable laboratory medicine specialists in the field of Pathology about their involvement in global health. Although their roles ranged from everything between medical technician, to PA, to medical student, to practicing pathologist, to the CEO of a major pathology organization, they all had one thing in common – they actively take the time to better their global community and contribute to improving pathology services in resource limited settings.
Now that the year is winding to a close, I’d like to take the opportunity to highlight all of these wonderful efforts and hopefully inspire you to take similar initiatives where applicable to your abilities and interest. Read on for a summary of each interview.
Dr. Kumarasen Cooper not only volunteers bi-annually in Botswana’s only academic pathology department as a way to give back to his native Africa, he has also worked to create an opportunity for residents at UPenn pathology to be involved too. Because of his efforts, the UPenn residents can accompany him and work together on the departments’ shared initiatives using official institutional elective time. This is a rare opportunity in pathology training, and is a model of how academic institutions can engage their trainees in global health initiatives.
Julie Papango, a medical technologist, has worked with Doctors without Borders/ Médecins Sans Frontières (MSF) to bring laboratory medicine to the world’s most remote places. She was one of MSF’s very few volunteers with laboratory experience and therefore has played a crucial role in projects ranging from addressing the infectious disease outbreaks in a Sudanese refugee camp, to helping the Cambodian Ministry of Health to improve their national tuberculosis detection program.
Dr. Ann Nelson is an expert in infectious disease pathology and has worked in many parts of Africa for more than 30 years. The focus of her work has been in HIV/AIDS pathology in the US and in sub-Saharan Africa. Currently she works on educational projects and capacity building in anatomic pathology, and linking anatomic pathology to ongoing clinical and epidemiologic research. She finds ways to be helpful in any new setting by just showing an open and willing attitude. “I went and built partnerships with everyone I could. You have to just go and talk to people, and ask them “What can we do?” With this approach, she’s been able to find countless ways to contribute her expertise to the world. She’s also spent innumerable hours in studying and publishing the issues affecting pathology services in Africa. Notably, she worked to conduct a landmark survey of African pathologists to determine the status of pathology resources in Sub-Saharan Africa.
Dr. Blair Holladay and Dr. Dan Milner have worked in global health most of their professional careers and now lead the American Society for Clinical Pathology’s efforts in improving laboratories worldwide. They are working with governments and local agencies to make sustainable changes in the neglected pathology and laboratory medicine landscape in low and middle income countries (LMICs). They are responding to the urgent need to improve pathology services to address the rapid increase in global non-communicable disease (NCD) incidence. As Dr. Holladay points out “Compared to the scale of the HIV crisis, NCDs are the health threat that gone unchecked, will go far beyond in affecting huge proportions of the global population.” In response to addressing this problem, Dr. Milner points out that the lab is the cornerstone to the solution: “In the field of cancer, which is a major problem in LMICs, you cannot treat the patient without a diagnosis – and the diagnosis must come from the laboratory.”
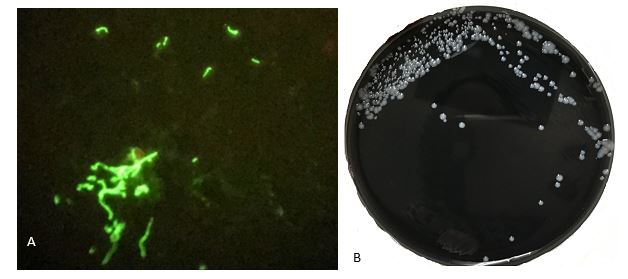
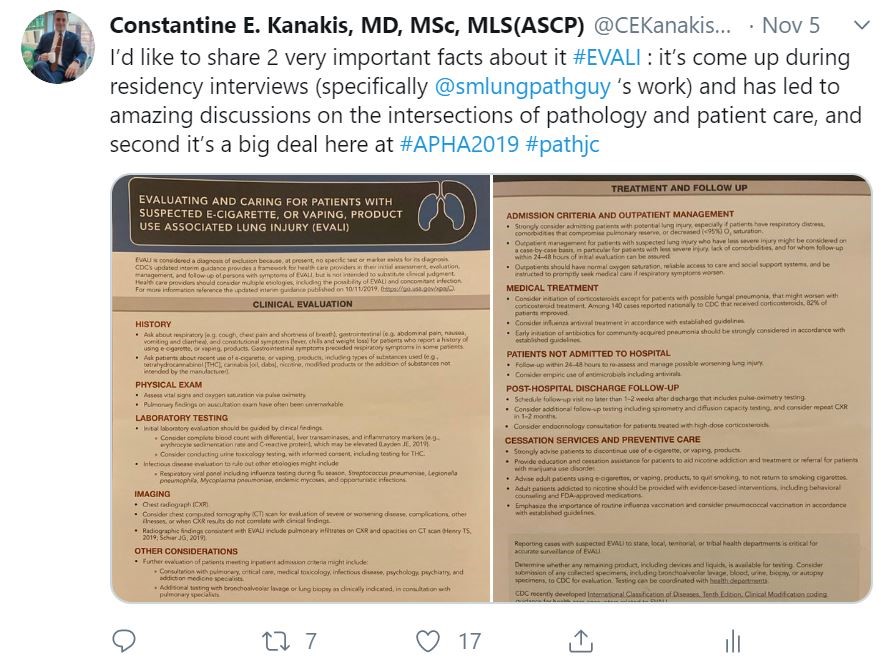
Dr. Constantine Kanakis is a medical student who decided to be an active part of the community of Sint Maarten while living there attending medical school. The community was facing multiple mosquito-borne infectious disease epidemics that includes Zika virus. In response, Dr. Kanakis took a service-learning elective course in medical school that focused on community outreach. He led the way to create an outreach program that has now been incorporated into the nation’s Ministry of Health Collective Prevention Services program. Dr. Kanakis encourages everyone to “Start by looking around at your immediate surroundings and take an assessment of the issues affecting the community. Anyone can do this, whether you are a physician, scientist, or a community member.”
Dr. Adebowale Adeniran, a cytopathologist, frequently works with the USCAP group “Friends of Africa” in which he speaks at the annual meetings, is involved in the group planning activities, and participates in educational initiatives and conferences in Africa. He encourages all academic institutions to engage in global health, stating “Academic institutions in the US can offer ways of enhancing training opportunities for African pathologists and trainees by offering short- or long-term exchange programs. This helps to bridge the gap between practiced based learning in resource limited vs. US institutions.”
Nichole Baker is a pathologist’s assistant that heard of a lab in Uganda that needed outside pathology help due to being severely understaffed. So Nichole decided to go visit the lab and see where she could help. One of the main issues was that the lab lacked an electronic medical record (EMR) system and keeping track of cases and patient reports was a real challenge. With no background in computer science, Nichole resourcefully reached out to her personal network to find someone that could help her build a free EMR and now the laboratory can track specimens, issue electronic reports, and has reduced their turnaround time as a result.
Dr. Drucilla Roberts is one of the world experts in perinatal pathology and has been working in Africa for over ten years with a focus on capacity building. Besides offering her surgical subspecialty expertise, she is also partnering with local pathologists to participate in ground breaking research on topics specific to low resource settings. She’s written widely on the need for pathology services in Africa. She says that one of the biggest problems in improving pathology services in Africa is that “there are not enough pathologists. You can help improve things in individual labs to a point, but for long term there has to be more pathologists working in Africa.” Dr. Roberts actively engages in solving this problem by helping train African pathology residents and by recruiting other pathologists to do the same.
Dr. Von Samedi, a cytopathologist, has worked with ASCP’s Center for Global Health at their partner sites all around the world. Dr. Samedi started working with ASCP as a resident, using his unique ability to speak French and Creole to assist ASCP in Haiti following the devastating 2010 earthquake. He has since worked on improving laboratory services in a vast array of ways, with everything from mentoring and local laboratorian training to running workshops on HIV related testing services. Volunteering gives Dr. Samedi a sense of purpose and he states that he “also benefits from interacting with my global colleagues and learning from them.”
There are so many more laboratory medicine specialists working in global health that I would have loved to feature on Lablogatory – but there are so many that I cannot capture all of their stories to share here. I hope that you have gained a snapshot of the potential ways that you can get involved, the possibilities are truly endless!
If you’ve been following this series, know that I am extremely grateful for your time and attention to this important matter. This will be my last post with Lablogatory for the time being, as I will be taking a break from writing to welcome my first child into the world! Wish me luck! J
If you want to find out more about volunteering in global pathology efforts, please visit my webpage that I have written in collaboration with Dr. Jerad Gardner: https://pathinfo.fandom.com/wiki/Global_Health_Opportunities_for_Pathologists
Please also take a moment to fill out this survey (https://www.surveymonkey.com/r/K7YK8LW) so that we can learn more about your interest and experience in global health and you can enter to win a global pathology prize pack!

-Dana Razzano, MD is a former Chief Resident in her fourth year in anatomic and clinical pathology at New York Medical College at Westchester Medical Center and will be starting her fellowship in Cytopathology at Yale University in 2020. She is passionate about global health and bringing pathology and laboratory medicine services to low and middle income countries. She was a top 5 honoree in ASCP’s Forty Under 40 in 2018 and was named to The Pathologist’s Power List of 2018 and 2019. Follow Dr. Razzano on twitter @Dr_DR_Cells.