Clinical presentation
An elementary school age child presented to the pediatric emergency department with an acute onset of abdominal pain. According to the parents, the patient recently had an ear infection and completed a course of amoxicillin. They noted the patient was more tired than usual, but did not have a fever. They reported no recent sick contacts or travel. Past medical history was significant for constipation, but normal bowel movements were noted over the past few days. On physical exam, the abdomen was soft and non-distended with diffuse mild tenderness noted on the right side. No masses were noted. Laboratory testing was unremarkable and the WBC count, liver & pancreas enzymes, and alpha fetal protein were within normal limits. An abdominal CT scan revealed a mass with central necrosis in the liver concerning for an abscess. The patient was started on ceftriaxone & metronidazole and underwent a surgical procedure to drain the lesion.
Laboratory Identification
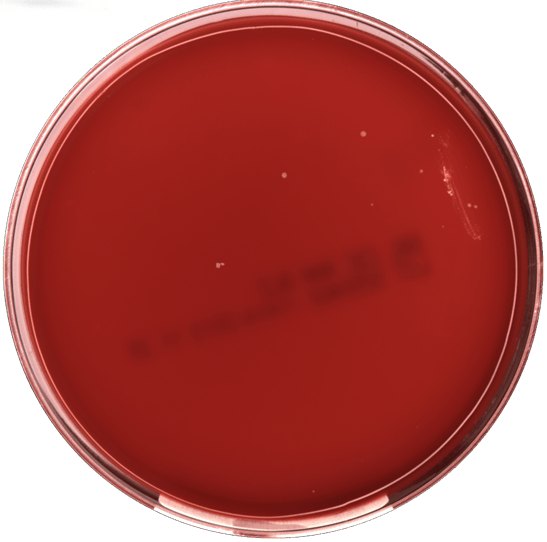
No bacterial growth was observed on blood or chocolate agars incubated at 35°C in CO2. MALDI-TOF mass spectrometry identified the isolate as a viridans groups streptococci, Streptococcus intermedius. The organism was susceptible to penicillin, ceftriaxone, and vancomycin by broth microdilution. Blood cultures were not collected for this patient.
Discussion
Streptococcus intermedius is a viridans group streptococci that belongs to the S. anginosus group. The S. anginosus group also includes S. anginosus and S. constellatus. This group of viridans streptococci composes the normal flora of the oropharynx, urogenital, and gastrointestinal tracts. These organisms are known for causing peritonitis and abscesses, particularly in the brain, breast, liver, and oral cavity.
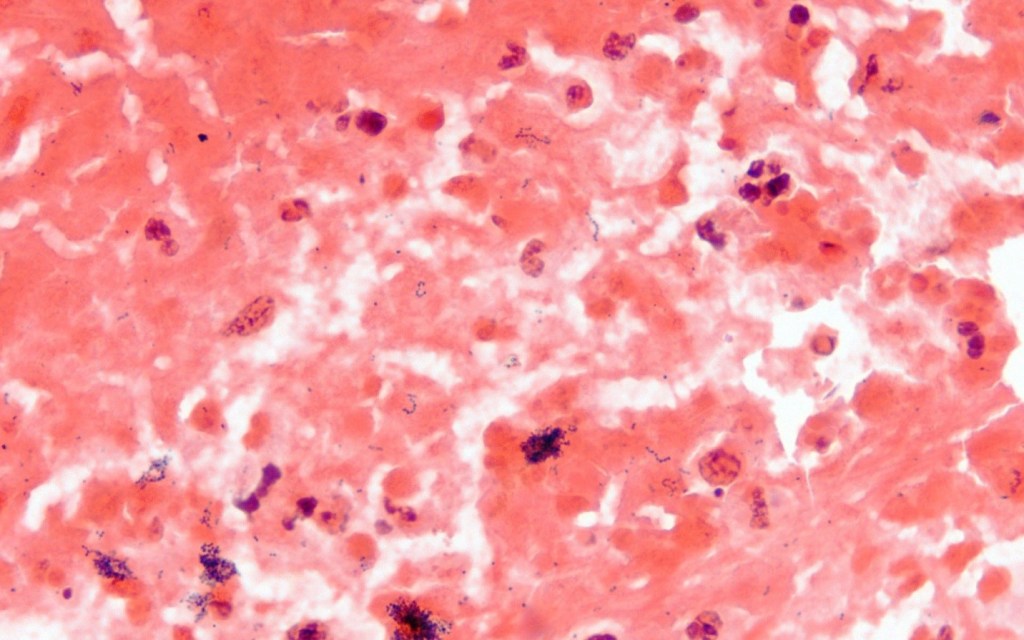
Similar to other streptococci, S. intermedius is a gram positive cocci that grows in chains and is catalase negative. The anginosus group are facultative anaerobes and grow as pinpoint colonies (<0.5 mm) on blood agar. This is in contrast to pyogenic, beta-hemolytic streptococci which are greater than 0.5 mm in size after the same incubation period. The anginosus group streptococci can exhibit a variety of hemolysis patterns, including alpha, beta, or gamma hemolysis. A distinct butterscotch or caramel odor is noted on examination. The anginosus group can possess Lancefield antigens A, C, F, G, or be non-groupable, so it is important not to misidentify them as other streptococci that also have these antigens.
Historically, further identification of viridans group streptococci was challenging; however, the advent of automated systems and MALDI-TOF mass spectrometry has been useful in providing species level identifications for more common isolates. Molecular sequencing methods using sodA gene can be helpful as well for the most reliable results. While penicillin resistance is becoming more frequent in viridians group streptococci, it is still rare in the S. anginosus group.
In the case of our patient, an echocardiogram was performed and found to be negative for endocarditis. The patient’s symptoms improved and they were discharged home on ceftriaxone and metronidazole. A follow up CT scan to confirm resolution of the abscess was scheduled.

-Lisa Stempak, MD is the System Director of Clinical Pathology at University Hospitals Cleveland Medical Center in Cleveland, Ohio. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Her interests include infectious disease histology, process and quality improvement, and resident education.
