A 54 year old male former smoker and alcohol user presented to the Emergency Department with a five day history of nausea, vomiting, diarrhea, weakness, fever with chills, breaking out in sweats, and abdominal discomfort. He denied recent sick contacts, travel or exposure to potentially contaminated foods. He had a past medical history that was significant for Chronic Obstructive Pulmonary Disease (COPD), mitral valve regurgitation and ST elevation myocardial infarction (STEMI). Some of his medications are inhaled Fluticasone, Advair Diskus, Furosemide and Spironolactone. He has also had a mitral valve replacement.
His initial laboratory tests revealed leukocytosis with neutrophilia, non-specific electrolyte derangements and negative stool tests for enteric bacterial pathogens. His symptoms progressed within the first 24 hours of admission, with a decrease in oxygen saturation (SPO2) and dyspnea so further investigations were carried out. Subsequently, a chest X-Ray was done, which showed pneumonia. The patient had a bronchoscopy and bronchoalveolar lavage (BAL) fluid was sent to the laboratory for aerobic, fungal, and acid fast bacilli culture, as well as Legionella spp. and Pneumocystis jiroveci direct fluorescent antigen testing.
Discussion
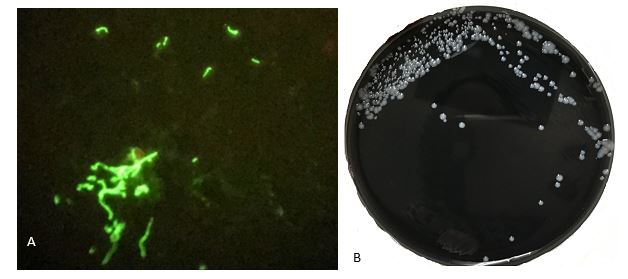
The presence of pneumonia and diarrhea in the patient raised suspicion for Legionnaires’ Disease, so the patient’s specimens including BAL fluid and bronchial washings were tested by direct fluorescent antigen (Image 1A) which confirmed Legionnaires’ Disease as the diagnosis.
Legionnaires’ Disease (LD), is a form of pneumonia caused by Legionella species, most commonly Legionella pneumophilia. Legionella spp.are motile, obligate aerobic, facultative intracellular and weakly gram negative rods. They are also nutritionally fastidious, requiring specific nutrients such as L-cysteine, and iron. They live in amoebas or in biofilms all over the world and are seen in high concentrations in warm waters plumbing systems, water heaters, warm water spas and cooling towers, and in very low concentrations in freely flowing cold water and biocide-treated waters.1 They are disseminated by devices that aerosolize water such as cooling units, hot tubs, water fountains and showers and cause disease when this contaminated aerosolized water is inhaled. The inhaled bacteria then enter the bacteria-killing macrophages in the lungs. Once in, they hijack the intracellular mechanism of the macrophages, feed off them, multiply within them, and then kill the macrophages, releasing more bacteria into the surrounding tissues.1
The incubation period of Legionella infections is 2 to 14 days, with a median of 4 days. In humans, Legionella spp. causes Legionellosis which comprises two separate diseases. These are Pontiac fever, a mild, self-limited flu-like illness, and LD, an atypical form of pneumonia which affects multiple organs. LD can range from mild to fatal in severity and about 12% of patients die from the disease.1 In most cases, LD begins with fever and symptoms of gastrointestinal infection including diarrhea and vomiting before patients develop respiratory symptoms such as cough and difficulty in breathing. However, LD also involves other organs/systems, causing renal failure and cardiogenic shock. LD occurs world-wide and all-year round but most cases occur between late fall and early spring.1
Although LD is relatively rare in the US, it is believed to be underdiagnosed due to failure to test for Legionella infection, poor sensitivity of test methods used to detect the disease, and failure to report all diagnosed cases.1 However, the rate of reported cases in the US has increased by about 5.5 times in the past 20 years to 7,500 reported cases in 20172, which may be partially attributed to increased and improved testing.
LD is more likely to occur in people with a suppressed immune system – particularly those on high-dose corticosteroids like Fluticasone, people with chronic lung, heart or kidney diseases, people who smoke or smoked in the past, people who travel, especially overnight travel, people who have received solid organ transplants, and people who use certain medications such as anti-tumor necrosis factor drugs.1 LD is often fatal and survival depends on how severe the pneumonia when treatment starts, the presence or absence of other serious comorbidities, and how early specific treatment for the disease is commenced.1 Therefore, prompt diagnosis is very important to survive LD.
Unfortunately, LD patients often present with nonspecific symptoms as well as chest X-ray, biochemical and hematological laboratory tests results. Therefore microbiological investigations which identify Legionella spp. are crucial in the management of these cases. The most commonly used test method is the Urinary Antigen test which detects the most common cause of Legionnaires’ disease, L. pneumophila serogroup 1. But, it does not detect other potentially pathogenic Legionella species and serogroups. Legionella spp. can also be cultured and identified, but this requires the use of Buffered Charcoal Yeast Extract [BCYE] agar which provides the specific growth requirements of Legionella spp.Common specimens for culture include lower respiratory secretions such as BAL and bronchial washings, lung tissue and pleural fluid. Other methods used to diagnose LD include polymerase chain reaction (PCR), direct fluorescence antibody (DFA), and paired serology. However, the Centers for Disease Prevention and Control, CDC recommends testing with culture and urinary antigen test in combination.2
LD is treated with Azithromycin or Levofloxacin. 95 to 99% of cases can be cured if they are otherwise healthy but treatment is started early.1
References
- Edelstein, Paul H. and Lück, Christian. “Legionella.” In Manual of Clinical Microbiology, Eleventh Edition, pp. 887-904. American Society of Microbiology, 2015.
- Centers for Disease Control and Prevention. Legionella (Legionnaires’ Disease and Pontiac Fever). https://www.cdc.gov/legionella/clinicians.html. April 30, 2018

–Adesola Akinyemi, M.D., MPH, is a first year anatomic and clinical pathology resident at University of Chicago (NorthShore). He is interested in most areas of pathology including surgical pathology, cytopathology and neuropathology–and is enjoying it all. He is also passionate about health outcomes improvement through systems thinking and design, and other aspects of healthcare management. Find him on Twitter: @AkinyemiDesola

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
