Case History
A 73 year old patient with a medical history significant for diabetes and diabetic foot ulcers presented to an outpatient orthopedic clinic complaining of right foot pain and fevers. Physical exam findings were significant for a right metatarsal ulceration that extended to the bone which prompted admission to a local hospital. Tissue from debridement of this ulcer was sent for routine bacterial culture and blood cultures were also collected. The patient was started on empiric antibiotics.
Laboratory Findings
The tissue culture gram stain showed mixed gram negative and gram positive bacteria. Two days after admission, an anaerobic blood culture bottle flagged positive with gram negative rods which could not be identified by Verigene nucleic acid detection test. It was plated on routine anaerobic and aerobic culture plates for further identification. Four days after admission, another blood culture set flagged positive with staphylococci which was identified on the Verigene as methicillin susceptible Staphylococcus aureus in the aerobic bottle. Seven days after admission, the gram negative organism grew and was identified by MALDI-TOF mass spectrometry as Campylobacter ureolyticus. The tissue culture grew mixed gram positive and negative bacteria including Staphylococcus aureus, Bacterodies fragilis group, and Trueperella bernardiae. The patient’s antibiotic therapy was tailored to cover the MSSA and Campylobacter and they were successfully discharged.
Discussion
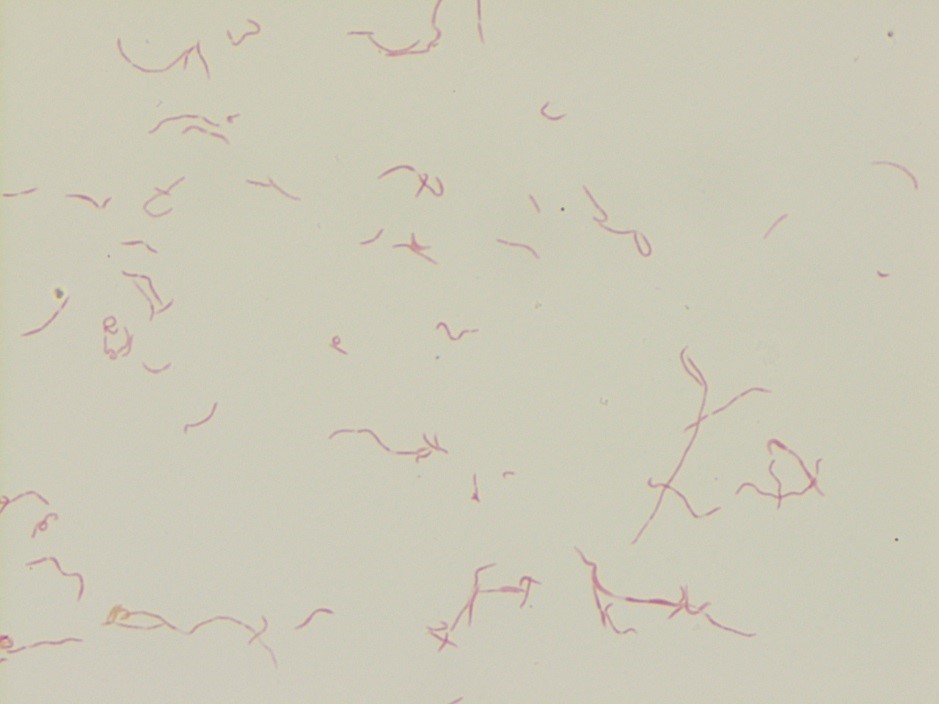
The Campylobacter genus has 24 species of bacteria including C. jejuni and C. coli which are the most frequent cases of campylobacteriosis, a diarrheal illness which is described below. Other less frequent pathogenic species include C. fetus, C. upsaliensis, C. lari, and C. ureolyticus. Campylobacter species appear as a curved S-shaped spiral rods and are gram negative on gram stain, are nonspore forming, and motile, with the exception of C. ureolyticus, which is aflagellate. Because Campylobacter is difficult to culture, rapid detection tests have been developed including antigen detection tests, however, these lack specificity. Several FDA approved nucleic acid amplification tests for Campylobacter exist, such as the BD MAX enteric bacterial panel that can detect C jejuni/C coli (speciation requires a reference lab).
Campylobacter grows best under microaerophilic conditions and at 42o C (closer to the body temperature of chickens). C. ureolyticus is unique as it grow anaerobically. Media that is selective and differential for Campylobacter, including charcoal cefoperazone deoxycholate agar (CCD) and charcoal based selective medium (CSM), is often used for stool specimens. Campylobacter appears as flat grey colonies that tend to spread along streak lines. Identification of Campylobacter includes a characteristic gram morphology, growth microaerophilically (expect for C. ureolyticus), and oxidase positivity. C. jejuni are hippurate hydrolysis positive. C. coli are hippurate hydrolysis negative, however, there are C. jejuni that are hippurate hydrolysis negative, making this test non-specific.
Clinical and Laboratory Standards Institute (CLSI) recommends antibiotic susceptibility testing for C. jejuni and C. coli and includes testing for ciprofloxacin, erythromycin, and tetracycline resistance which requires microaerophilic conditions.
Campylobacter is mainly a zoonotic disease acquired from poultry, cattle, sheep, pigs, and domestic pets. C. ureolyticus, is thought to be transmitted most frequently form cattle, however, more research is needed in this area. A common cause of Campylobacter is consumption of undercooked meat, especially poultry due to the high prevalence of Campylobacter in US retail poultry. In 2015, 5,000 US retail poultry samples were tested for Campylobacter with 12% of samples testing positive; 24% of chicken breast samples tested positive and 0.2 % of ground turkey samples tested positive. The majority of isolates were C. jejuni and C. coli (65% and 34% respectively). In 2004, 60% of chicken samples tested positive in the US (1). Campylobacter most frequently infects young children ages 1-5 as well as adolescents and young adults and is most frequently seen between the months on June and August (1).
C. ureolyticus is a less studied species of Campylobacter, however there is evidence that this species can cause diarrheal disease and extra –intestinal infections. Some studies of fecal specimens from patients presenting with diarrhea illness in Ireland revealed 24% of Campylobacter positive stools were C. ureolyticus species (4). C. ureolyticus has also been isolated skin and soft tissue abscesses, however, C. ureolyticus is rarely the sole bacteria isolated, raising the questions of whether it a true soft tissue pathogen. The most frequent soft tissue site of infection is the perianal region (4).
Campylobacter usually presents as a diarrheal illness, causing fever, diarrhea (can be bloody or non-bloody), and abdominal cramping with symptoms lasting days to weeks. The disease is usually self- limited, but in 10-15% of cases patients are admitted to hospitals (1). Generally, patients will clear campylobacter enteritis without the need for antibiotics. Indications for antibiotics include severe bloody diarrhea, relapsed cases, high fever, greater than 1 week course, and extraintestinal infections or immunocompromised status. Interestingly, presentations of C. jejuni/C. coli can mimic appendicitis and lead to unnecessary appendectomies. Extra-intestinal infections include bacteremia, septic arthritis, abscess formation, meningitis, peritonitis, prostatitis, urinary tract infections, and neonatal sepsis. Guilian-barre syndrome can be seen after C. jejuni infections, especially the heat stable serotypes HS19 and HS41, which is medicated by antibodies that develop against ganglioside-like epitopes in the bacterial cell wall LPS region which cross react with peripheral nerve gangliosides. C. jejuni/C. coli can also induce reactive arthritis and rarely have been implicated in inciting inflammatory bowel disease exacerbations and celiac disease (1-2).
In severe infections or extraintestinal infections, azithromycin is the preferred antibiotic as fluoroquinolone resistance is rising in the US. In 2014, 27% of C. jejuni and 36% of C. coli isolates were resistant to ciprofloxacin, and 2% of C. jejuni and 10% of C. coli isolates were resistant to azithromycin (1-2). In an Italian cohort of patients, greater than 60% of Campylobacter strains were ciprofloxacin or tetracycline resistant, while 29% of C. coli isolates were resistant to tetracycline, fluoroquinolones, and macrolides (3). Interestingly, use of these antibiotics in animal feed has been directly associated with the occurrence of antibiotic resistant Campylobacter stains (1-3). Antibiotic resistance and guidelines for the management of C. ureolyticus infections is largely unknown.
Overall, Campylobacter usually presents as a self-limiting diarrheal illness, however, less frequently extra-intestinal infections can occur such as in this patient’s case. The most common pathogenic species include C. jejuni and C. coli, while other Campylobacter species are seen less frequently. In this patient’s case, C. ureolyticus was isolated from the blood after the patient developed a right metatarsal ulcer. While we were unable to culture Campylobacter from the patient’s wound culture, this is the most likely source of their blood stream infection.
References
- Whitehouse CA, Young S, Li C, Hsu CH, Martin G, Zhao S. Use of whole-genome sequencing for Campylobacter surveillance from NARMS retail poultry in the United States in 2015. Food Microbiol. 2018;73:122-128.
- Tack DM, Marder EP, Griffin PM, et al. Preliminary incidence and trends of infections with pathogens transmitted commonly through food – Foodborne Diseases Active Surveillance Network, 10 U.S. sites, 2015-2018. Am J Transplant. 2019;19(6):1859-1863.
- Garcia-Fernandez A, Dilonisi AM, Arena S, Iglesias-Torrens Y, et al. Human Campylobacteriosis in Italy: Emergence of Multi-Drug Resistance to Ciprofloxacin, Tetracycline, and Erythromycin. Front Microbiol. 2018 Aug 22;9:1906. doi: 10.3389/fmicb.2018.01906. eCollection 2018.
- O’donovan D, Corcoran GD, Lucey B, Sleator RD. Campylobacter ureolyticus: a portrait of the pathogen. Virulence. 2014;5(4):498-506.
-Liam Donnelly, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
