The Centers for Medicare & Medicaid Services (CMS) think so.
Recently, the American Society for Clinical Pathology (ASCP) alerted its members to this action. From the email:
“On April 1, CMS announced that “an associate’s or bachelor’s degree in nursing is equivalent to an associate’s or bachelor’s degree, respectively, in biological science”—seemingly declaring that individuals with a nursing degree are potentially as qualified to perform advanced testing as certified laboratory professionals. It also appears that CMS’s position could allow individuals with as little as a bachelor’s degree in nursing to direct a CLIA moderate complexity laboratory and/or serve in senior supervisory roles within a CLIA high complexity laboratory. Since the Clinical Laboratory Improvement Amendments (CLIA) of 1988 doesn’t specifically require clinical training of individuals with a degree in biological sciences, CMS’s new policy exempts individuals with a bachelor’s degree in nursing from any specific training requirement prior to performing high complexity testing for diagnostic purposes.”
ASCP is urging the laboratory community to ask CMS to reconsider its position that nursing is a biological science for purposes of performing laboratory testing by signing this petition.
Transfusion-associated graft-versus-host disease (TA-GVHD) is a rare complication that develops 4 to 30 days after the transfusion of cellular blood products (i.e. red blood cells, platelets, granulocytes). It can occur in both immunocompromised and immunocompetent patients, and recognition is often delayed because the nonspecific symptoms are attributed to the patient’s underlying diagnosis. TA-GVHD affects the transfusion recipient’s bone marrow and is nearly universally fatal, making prevention absolutely essential.
TA-GVHD is mediated by viable mature immunocompetent donor lymphocytes against the recipient’s antigen presenting cells. TA-GVHD does not occur after most transfusions because the donor lymphocytes are destroyed by the recipient’s immune system before they can mount a response against the host. However, this protective response does not occur in certain settings. One is profound cell-mediated (T cell) immune deficiency, resulting from congenital, acquired, or iatrogenic causes. Another occurs when there is a specific type of partial Human Leukocyte Antigen (HLA) matching between the donor and recipient. HLA molecules are the primary means of distinction between self and non-self. If the donor HLA phenotype is homozygous and the recipient expresses the same HLA haplotype, it may mask donor lymphocytes from the recipient. The end result is engraftment and proliferation of mature donor T cells in the recipient’s bone marrow.
The donor T cells are then activated by mismatched HLA class I major antigens. This immunologic assault typically manifests clinically with fever and an erythematous, maculopapular rash which often progresses to generalized erythroderma. In addition to skin dysfunction, liver, gastrointestinal tract, and bone marrow symptoms are also common. The main laboratory findings of TA-GVHD include pancytopenia due to hypocellular marrow, abnormal liver function tests, and electrolyte abnormalities induced by diarrhea.
The differential diagnosis of TA-GVHD is broad. A more definitive diagnosis is suggested from skin biopsy which classically reveals vacuolization of the basal layer and a histiocytic infiltrate, and occasionally shows an almost pathognomonic finding — satellite dyskeratosis, which is characterized by single, dyskeratotic cells accompanied by lymphocytes. The definitive diagnosis of TA-GVHD relies in demonstrating that circulating lymphocytes have a different HLA phenotype from recipient APCs, proving that they came from the donor.
As mentioned above, TA-GVHD portends a high mortality rate and is poorly responsive to the available therapies; therefore prevention is of primary importance. Current strategies include gamma irradiation or leukocyte inactivation (i.e. pathogen reduction technology) of the blood products prior to transfusion to disable donor lymphocytes. Some of the more common indications for patients requiring irradiated blood products include those who are immunosuppressed, who have received a hematopoietic cell transplant, who are receiving blood components from a related donor, or who are given HLA-matched platelets. There is also evidence that transfusing older products decreases the risk of TA-GVHD due to the shortened lifespan of T cells within the products. In summary, TA-GVHD can occur in both immunocompetent and immunocompromised recipients, is mediated by donor T lymphocytes, and is almost always fatal.
-Thomas S. Rogers, DO is a third-year resident at the University of Vermont Medical Center, a clinical instructor at the University of Vermont College of Medicine, and the assistant medical director of the Blood Bank and Transfusion Medicine service.
A 53 year old male presents to the emergency department with complaints of fatigue, night sweats, dyspnea, dry cough, and right knee swelling. He has multiple skin lesions including violaceous papules on his medial thigh, subcutaneous nodules on bilateral lower legs, and ulcerations on his right lateral leg. His past medical history is significant for psoriatic arthritis. Previously, he has taken adalimumab (Humira), etanercept (Enbrel), and golimumab (Simponi), but his current treatment regimen consists of methotrexate and prednisone. His recent travel history is significant for scuba diving in Thailand and honeymooning in the Caribbean. Dermatology was consulted and a punch biopsy was performed close to an ulcer on his right lateral leg and sent to surgical pathology. An additional biopsy specimen was sent to microbiology for bacterial, fungal and mycobacterial cultures.
Laboratory Identification
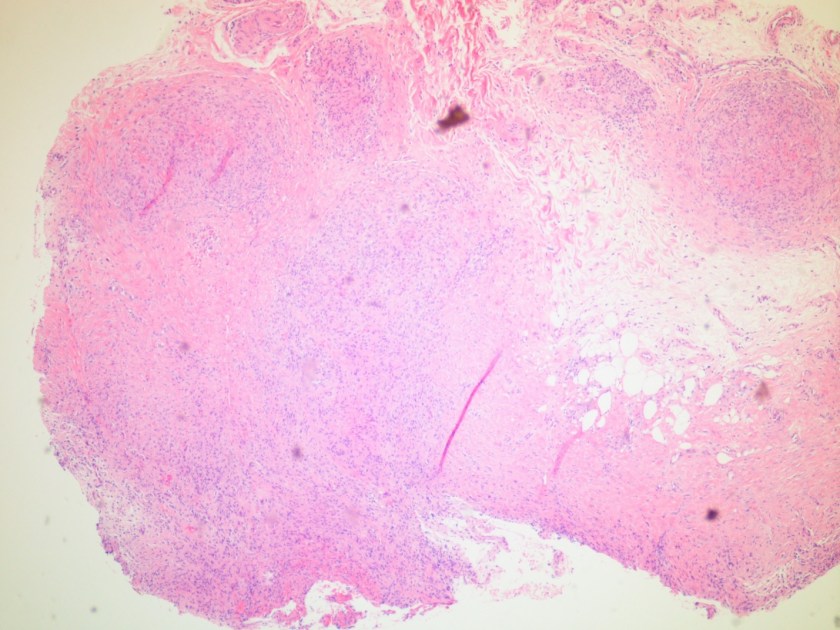
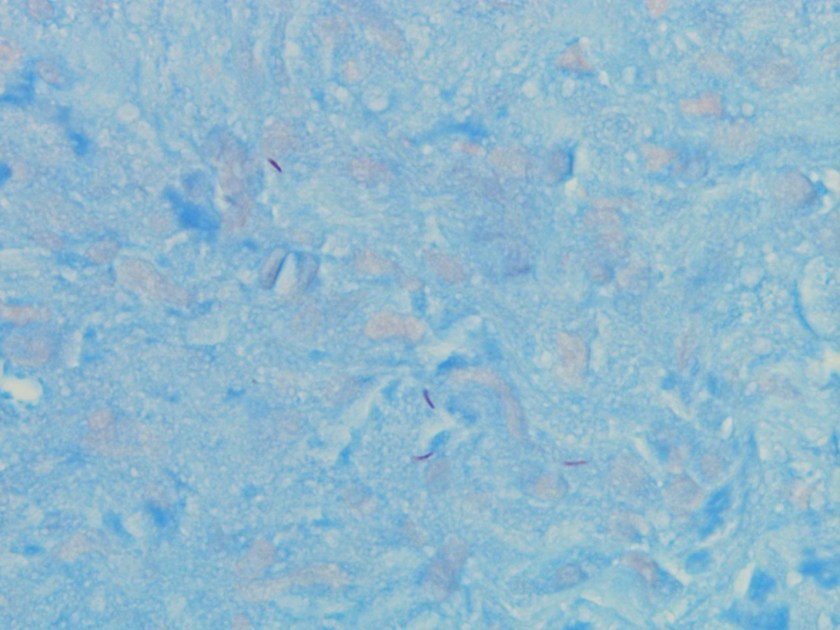
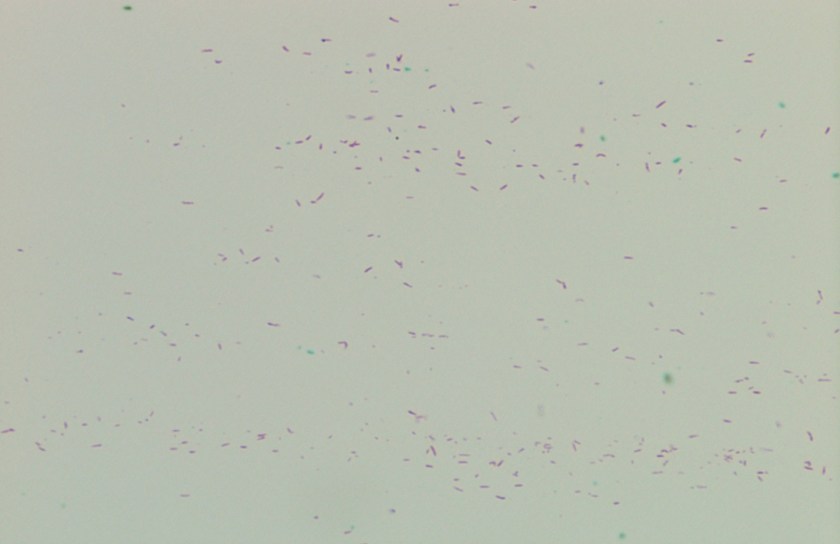
Figure 1. Histology sections of the punch biopsy near the patient’s right lateral leg ulcer. The epidermis and dermis appeared unremarkable. However, a non-caseating granuloma is seen in the deep subcutaneous tissue (H&E, 40x).Figure 2. Special stain highlighting the occasional acid fast organisms (Kinyoun, 1000x oil immersion).Figure 3. Smear from a positive mycobacteria growth indicator tube (MGIT) incubated at 32°C showing abundant acid fast bacilli (Ziehl-Neelsen, 500x oil immersion).
Microscopic examination of the punch biopsy skin specimen revealed a non-caseating granuloma in the deep subcutaneous tissue, with no involvement of the overlying dermis and epidermis (Figure 1). A Kinyoun stain of the tissue showed that the granuloma contained occasional acid-fast bacilli (Figure 2). The bacterial and fungal cultures sent to microbiology were negative. Portions of the specimen used to set up the mycobacterial cultures were incubated in MGITs at 32 and 37°C because the specimen source was skin. The 32°C tube, which was supplemented with hemin, gave a positive signal after 3 weeks of incubation. The Ziehl-Neelsen stain from this tube revealed numerous acid fast bacilli (Figure 3). DNA Gen-Probe analysis was negative for Mycobacterium tuberculosis complex and M. avium-intracellulare (MAI) complex. The organism was identified as M. haemophilum by pyrosequencing.
Discussion
Mycobacterium haemophilum was first identified in 1978 from an Israeli patient with Hodgkin lymphoma. It has a known predilection for infecting the skin and subcutaneous tissue in immunocompromised patients, especially those with lymphopenia as a result of acquired immune deficiency syndrome (AIDS), allogeneic bone marrow transplantation, and those on immunosuppressant therapies for rheumatologic conditions. The clinical presentation frequently consists of painful subcutaneous nodules and ulcers that can progress to abscesses and draining fistulas. Bone and joint infections have also been reported, which manifest as arthritis, tenosynovitis, and osteomyelitis. AIDS patients in particular are known to present with disseminated disease, with multiple cutaneous lesions, mainly involving the extremities. Relatively little is known about this infection and the optimal treatment is not standardized, but combinations of three or four of the following drugs have been used successfully: isoniazid, rifamycins, ciprofloxacin, amikacin, doxycycline, and clarithromycin.
Unlike the majority of mycobacteria, M. haemophilum does not grow well in culture at 37°C. Rather, it prefers lower temperatures, ideally between 28–32°C. This characteristic is shared by several other mycobacterial species that also characteristically infect the skin, including M. marinum, M. chelonae, M. abscessus, and M. ulcerans. A unique feature of M. haemophilum among the mycobacteria is that it requires hemin (X factor) to survive and will only grow in media enriched with this nutrient. Similar to Haemophilus influenzae, M. haemophilum can be cultured on chocolate agar, as well as on Middlebrook 7H10 agar incubated with an “X-factor strip” and on Lowenstein-Jensen medium containing 2% ammonium citrate.
Typically, colonies grow after 2-4 weeks of incubation at 32°C and have either a rough or smooth appearance. M. haemophilum is a non-photochromogen according to the Runyon classification system, and its colonies are buff colored and do not produce pigment in either light or dark conditions. M. haemophilum is chemically inert by traditional biochemical mycobacterial tests, with the exception of pyrazinamidase production. As illustrated by this case, DNA probe analysis is helpful with regard to the mycobacterial species it excludes, but not for speciation of less common organisms. At the present time, DNA probes exist only for M. tuberculosis complex, MAI complex, M. kansasii, and M. gordonae.
In the case of our patient, the species level identification was determined by pyrosequencing. He was treated with an extended course of 3 agents: rifabutin, clarithromycin, and moxifloxacin with good response.
–Vikas Nath, MD, is a 4th year resident in Anatomic and Clinical Pathology at the University of Mississippi Medical Center in Jackson, MS.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as in Medical Microbiology. Currently, she oversees testing performed in both the chemistry and microbiology laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
A 40 year old patient presented with macrocytic anemia.
CBC Results:
WBC: 8.6 K/uL Normal
RBC: 3.60 M/uL Decreased
Hb : 13.1 g/dl Normal
MCV: 111.3 fl Increased
MCH: 36.4 pg Increased
MCHC: 32.7 Normal
RDW: 15.5% Increased
Platelet: 360 K/uL Normal
Review of peripheral smear showed several stomatocytes (Figures 1-3).
Figure 1
Figure 2Figure 3
Serum vitamin B12 and folate levels were normal and serum iron studies were consistent with anemia of chronic disease. Typically anemia of chronic disease is normocytic normochromic. Based on presence of numerous stomatocytes and macrocytosis (which can be seen in patients with hereditary stomatocytosis) it was recommended that patient be investigated for hereditary stomatocytosis and acquired causes of stomatocytosis.
STOMATOCYTES
“Stomatocyte” describes the appearance of red blood cells (RBCs) on the peripheral blood smear. Stomatocytes (also called hydrocytes) contain a mouthlike or slitlike pattern that replaces the normal central zone of pallor.
Mechanism of stomatocyte formation — When the normal biconcave disc becomes a uniconcave cup red blood cell (RBC) will appear as a stomatocyte on the peripheral blood smear. There are several mechanisms by which this change can occur:
In hereditary stomatocytosis (HSt), the mechanism of stomatocyte formation often involves changes in cell volume caused by reduced intracellular ion content.
In most cases of acquired stomatocytosis and rare inherited conditions that affect lipid metabolism formation often involves either a decrease in RBC membrane surface area or qualitative changes in the composition of the membrane lipid bilayer.
DISORDERS WITH STOMATOCYTES ON PERIPHERAL BLOOD
Hereditary stomatocytosis (HSt) is an inherited autosomal dominant condition characterized by an excess of stomatocytes Patients have variable degrees of hemolysis and anemia. Hereditary stomatocytosis (HSt) is a rare disorder that presents with various degrees of hemolytic anemia and abnormal red blood cell (RBC) morphology. The genetic abnormalities responsible for these conditions remain incompletely characterized. Some of the defects associated with this condition involve membrane transporters such as Piezo1, Gardos, Rhesus antigen-associated glycoprotein, and the anion exchanger band 3.
Several rare inherited defects affecting membrane lipid composition have been reported to have stomatocytosis on the peripheral blood smear.
Tangier’s disease
Rh null disease
Phytosterolemia
Liver disease/medications. Stomatocytes can be seen with some acquired conditions such as chronic liver disease (most often due to alcoholism) or acute alcohol intoxication. The stomatocytosis with acute alcohol intoxication appears to be transient, and it may affect a significant proportion of RBCs. The mechanism is thought to be due to a reduction in RBC membrane surface area rather than an increase in RBC volume. Also, dministration of some medications can cause transient stomatocytosis. This was demonstrated in a study that demonstrated formation of stomatocytes upon exposure of RBCs to drugs like vinblastine and chlorpromazine. Intercalation of the drug into the inner half of the lipid bilayer may be responsible for creating the abnormal morphology.
In some healthy individuals, stomatocytes occasionally can be found on the peripheral blood smear. This is thought to be due to a drying artifact; hence, it is important to evaluate several different areas of the peripheral smear before determining that a patient has circulating stomatocytes.
Hereditary stomatocytosis (HSt)
HSt can be completely asymptomatic or can present with chronic hemolytic anemia of varying severity. The age of presentation depends on the specific gene mutation, presence of other inherited conditions, and other environmental factors. The increasingly routine use of the complete blood count (CBC) in asymptomatic individuals has resulted in earlier diagnosis in some individuals who otherwise might never have come to medical attention. There does not appear to be a relationship between the degree of peripheral stomatocytosis on the blood smear and the severity of hemolytic anemia
The diagnosis of HSt is made by demonstrating the presence of anemia associated with the characteristic changes in RBC morphology (stomatocytosis) in conjunction with altered RBC indices and osmotic fragility. Genetic testing for PIEZO1 or Gardos channel mutations is confirmatory but not required.
The evaluation for HSt includes review of the complete blood count (CBC) and peripheral blood smear, which may show stomatocytes.The blood smear should be reviewed closely to ensure there are no abnormalities of white blood cells (WBCs) or platelets. The RBC indices typically show an increased mean corpuscular volume (MCV) in the range of up to 140 femtoliters (fL) and abnormally low or high mean corpuscular hemoglobin concentration.
-Neerja Vajpayee, MD, is an Associate Professor of Pathology at the SUNY Upstate Medical University, Syracuse, NY. She enjoys teaching hematology to residents, fellows and laboratory technologists.
Transgender healthcare is a topic that doesn’t get a lot of attention. Healthcare providers receive little to no formal training in this area, and this population is one of the most under served groups in the United States. The authors of the recent Lab Medicine paper Challenges in Transgender Healthcare: The Pathology Perspective wrote a blog on this topic for Oxford University Press. Check out obstacles in transgender healthcare to learn some of the issues providers and patients face.
As I mentioned last month, a big part of my job has been to do daily rounds through the lab to seek out areas that need troubleshooting. One point I noticed was technologists don’t always see the impact of their work on patient care. I wanted to make sure they knew the importance of their work so I decided to incorporate education as a tool to highlight how their work directly affects patient care. Each section of the laboratory has their own ways of communicating so I have done something a little different in both labs.
In the microbiology section, I started a weekly “formal” microbiology rounds with the infectious disease doctors, the pharmacists, and the technologists. While I saw this rounding at both of my training institutions, there were held in different styles. In one, the infectious disease team rounded through the lab and asked the techs questions about their patients; in the other, the team discussed interesting case around a microscope. I decided to take a combined approach: we meet in the lab at the microscope so the techs can work if needed yet still be a part of the discussion. The techs save interesting cases that have come up over the last week or so and we show the rest of the team. It usually involves discussing organism identification methods as well as the disease process associated with the organism. This has given the techs the chance to ask the physicians and pharmacists questions about the patient isolates they have worked on directly. In addition, it has given them the opportunity to ask why physicians order certain tests. The pharmacists have added so much to these rounds and it has been nice to see a collaborative effort between multiple areas of the patient care team come together and talk about why things are done and the outcome of the patient based on laboratory results. It demonstrates to everyone that each member of team is passionate about patient care. In order to bring some of this knowledge to the second shift staff that performs microbiology processing, I save one or two interesting cases from rounds and present a quick rundown of what the bug is and how it is identified in the lab so they can see how their work is completed the next day.
For chemistry and immunology, the laboratory team has a monthly meeting. At each of these meetings, I run through a formal case presentation based off interesting cases the techs have come across or have had questions on specific disease processes related to the laboratory work they are performing. The topics have ranged from beer potamania (that got a lot of discussion!) to what polymerase chain reaction is. It has been another approach to show the technologists how their work directly impacts patient care and they have really enjoyed it. The goal is to bring clinicians into these discussions, as well, but that has not been as easy for these meetings. We have been able to bring a pharmacist in to discuss vancomycin trough levels and why draw times are so specific. It really helps having other departments reach out to the laboratory staff to let them see why policies are structured the way they are.
I really enjoy being in the lab and interacting with the technologists, however, one of the principal lessons I have learned this year is how important it is to get out of the laboratory as a clinical pathologist. The next couple of months I will talk about how I have gotten involved in other areas of the hospital. But for now, let’s hear from you, do you have any formal rounding or education that you offer your techs? What ideas have had the best responses from the technologists? I am looking forward to hearing more ideas on how to integrate education and interdisciplinary teamwork for our laboratory staff.
-Lori Racsa, DO, is the director of microbiology, immunology, and chemistry at Unity Point Health Methodist, and a Clinical Assistant Professor at the University Of Illinois College Of Medicine at Peoria. While microbiology is her passion, she has a keen interest in getting the laboratory involved as a key component of an interdisciplinary patient care team.
A 34 year old G3P3 woman presents with PPROM at 30+4 weeks gestational age. Her pregnancy had been complicated by fetal hydrops and intrauterine growth restriction with evidence of multiple fetal anomalies and placenta previa.
Prenatal infectious disease testing was significant for:
CMV IgG+/IgM+
Toxoplasmosis IgG+/IgM+
Parvovirus B19 IgM-/IgG+
HIV screen negative (ELISA)
HSV IgM-
syphilis screen negative (RPR)
rubella immune (IgG+)
negative serologies for Hepatitis A, B and C
Testing for VZV was not performed
Clinically, the fetal hydrops and IUGR were thought to be due to congenital CMV. She underwent caesarian section, and a fetus was delivered with APGAR 0/1/1/2/1, with eventual fetal demise at two hours of life. The placenta was sent to the laboratory for surgical pathology examination. The mother declined fetal autopsy.
Laboratory Work-Up:
Surgical pathology received a singleton placenta (13 x 13 x 4 cm) with attached umbilical cord and fetal membranes. The placental disc weighed 346 grams (<10th percentile for gestational age). Otherwise, the placental disc, umbilical cord and fetal membranes were negative for any gross abnormalities.
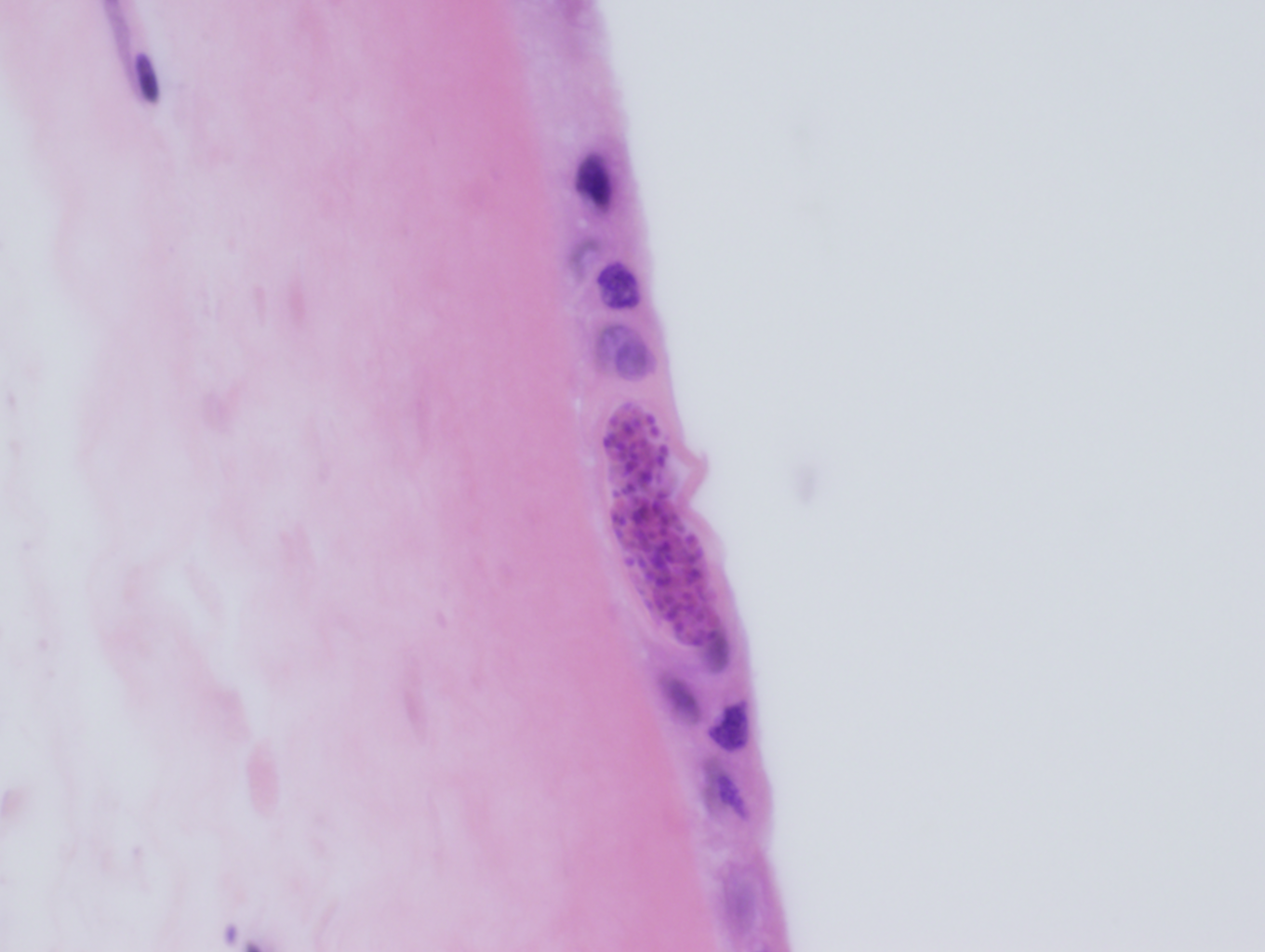
Routine microscopic sections demonstrated round to elongate cysts within the amnion of the fetal membranes (Figures 1a & 1b) and within the Wharton’s jelly of the umbilical cord (Figure 2). These cysts measured approximately 50 microns in diameter and had a thin, translucent cyst wall. Within the cysts were innumerable small round “dot-like” forms which could best be appreciated by focusing up and down through the plane of the section.
Tissue gram stain (Brown & Brenn) was negative for significant bacterial infiltrate, and immunohistochemistry for CMV was negative for CMV inclusions.
Figure 1a: Amnion of the fetal membrane: Round to elongate cysts measuring approximately 50 microns in diameter. There are innumerable small round “dot-like” structures within the cysts (H&E, 600X).Figure 1b: Amnion of the fetal membrane: Round to elongate cysts measuring approximately 50 microns in diameter. There are innumerable small round “dot-like” structures within the cysts (H&E, 600X).Figure 2: Wharton’s jelly of the umbilical cord: Round cyst measuring approximately 50 microns in diameter. There are innumerable small round “dot-like” structures within the cyst (H&E, 600X).
Discussion:
The histologic features are diagnostic of congenital Toxoplasmosis. The case was sent to the reference laboratory, where immunohistochemical staining for Toxoplasmosis demonstrated positive staining within the tissue cysts.
Toxoplasmosis is caused by the protozoa Toxoplasma gondii, a member of the protozoan subgroup coccidia, which also includes the GI pathogens Cryptosporidium, Isospora and Cyclospora. Cats of the family Felidae (including but not limited to domestic cats) are the only definitive host, while virtually any mammal can serve as an intermediate host. Humans can become incidentally infected in which case they act as “incidental” intermediate hosts.
The life cycle of Toxoplasma involves sexual reproduction in the definitive host (cats), as well as asexual reproduction in the intermediate host. Toxoplasma is “facultatively heteroxenous,” in that reproduction in the intermediate host is not necessary for completion of the life cycle. Unsporulated oocysts are shed in the cat feces and become infective after 1-5 days. Cats may ingest the infective oocysts, leading to sexual reproduction and completion of the life cycle within the intestinal epithelium. Alternatively, intermediate hosts such as rodents or birds ingest infective oocysts and subsequently develop infective tissue cysts. If the intermediate host is eaten by a cat, the infective tissue cysts are ingested, leading to sexual reproduction in the cat and completion of the life cycle.
The life cycle within the intermediate host involves two morphologically distinct stages, the tachyzoite and the bradyzoite. When infective oocysts are ingested by an intermediate host, they transform into tachyzoites, which are able to invade the intestinal epithelium and then widely distribute throughout the body. Tachyzoites are crescent-shaped, non-encysted and measure from 3-7 microns in length by 2-4 microns in diameter. They migrate preferentially to the muscle and neural tissues, where they eventually develop into tissue cysts, which are known as bradyzoites. Bradyzoites are much larger than tachyzoites (approximately 50 microns), are round to elongate and contain numerous “dot-like” parasitic forms encased within a thin cyst wall. Tachyzoites are eventually cleared following acute infection, but the intermediate host remains chronically infected with bradyzoites. If the host becomes immunocompromised, the bradyzoites differentiate into tachyzoites, which then recirculate through the body leading to reactivation of latent disease.
It is estimated that 10-20% of the U.S. population is chronically infected with Toxoplasma. Humans can become infected through one of five mechanisms: (1) ingestion of infective oocysts, either from cat feces or from infected water or other environmental sources, (2) ingestion of infective tissue cysts in undercooked meat, (3) vertical transmission to the fetus from a mother acutely infected with Toxoplasma, (4) through organ transplantation and (5) through blood transfusion. Epidemiologically, it is not clear whether the majority of infections occur through ingestion of infective oocysts or whether tissue cysts in undercooked meat are the major source of infection.
Vertical transmission from mother to fetus requires a first-time exposure during pregnancy. In primary/acute infection, tachyzoites widely disseminate and are able to invade the developing fetal tissues. By contrast pregnant women who are chronically infected with Toxoplasma harbor only tissue cysts (bradyzoites) and will not transmit infection to the fetus.
Acute infection is self-limited and usually asymptomatic, however some patients may have mild flu-like symptoms. A smaller subset of patients present with moderate to severe acute infection which can mimic mononucleosis: fever, sore throat, myalgias and cervical lymphadenopathy. Biopsy of inflamed lymph nodes reveals the classic histologic triad of follicular hyperplasia, monocytoid B-cell hyperplasia and epithelioid histiocytic aggregates. Once acute infection has passed, chronic infection is usually asymptomatic, unless the host becomes immunocompromised, in which case reactivation of latent disease can occur.
Treatment for immunocompetent patients in not indicated as acute infections are self-limited and chronic infection is asymptomatic. Immunosuppressed patients with CD4 counts <100 cells/mm3 should receive Toxoplasma prophylaxis with trimethoprim-sulfamethoxazole (TMP-SMX). Reactivation of latent disease can occur in immunosuppressed patients who are not taking prophylaxis, in which case first line treatment includes combination therapy with sulfadiazine and pyrimethamine.
-Javier De Luca-Johnson, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 2 year old female with a past medical history of spinal muscular atrophy type 1, trach/ventilator dependency presents to the hospital with complaints of desaturations at home. She has been hospitalized four times within the past year with an additional two visits to the emergency department. Patient has history of growing Pseudomonas aeruginosa from her lower respiratory tract culture. They began to work up causes of acute desaturations: mucus plug vs. viral illness vs. tracheitis vs. bacterial pneumonia. They sent tracheal aspirate and blood for cultures. The following organism was identified as the predominant organism from the tracheal aspirate.
Colony morphology on 5% sheep blood agar.Colony Gram stain.
Discussion
Chryseobacterium spp. are non-motile, oxidase positive, indole positive Gram-negative bacilli. While often considered low virulence environmental organisms, Chryseobacterium spp. can be pathogenic in immunocompromised patients and those less than six months of age. Chryseobacterium spp. and closely related bacteria are able to survive in chlorinated water and are intrinsically resistant to many antibiotics. They are often nosocomal pathogens that are selected for in immunocompromised patients who are treated with broad-spectrum antibiotics for long periods of time. Chryseobacterium spp. have been reported to cause blood stream infections, cellulitis, pneumonia, meningitis, pyomyositis and keratitis. The most common setting of Chryseobacterium infections is foreign bodies such as indwelling catheters or prosthetic joint materials. In the adult setting, Chryseobacterium indologenes has been associated with the history of colistin or tigecycline use. Due to its low pathogenicity, Chryseobacterium spp. are generally considered contaminants in otherwise healthy individuals.
Chryseobacterium spp. have a pair of interesting resistance mechanisms. They inherently have a Class A β-lactamase and a Class B-carbapenemase that function to hydrolyze β-lactamases. Due to these mechanisms, Chryseobacterium spp. are intrinsically resistant to carbapenems and cephalosporins. Common treatment options include: levofloxacin, sulfamethoxazole trimethoprim and piperacillin-tazobactam.
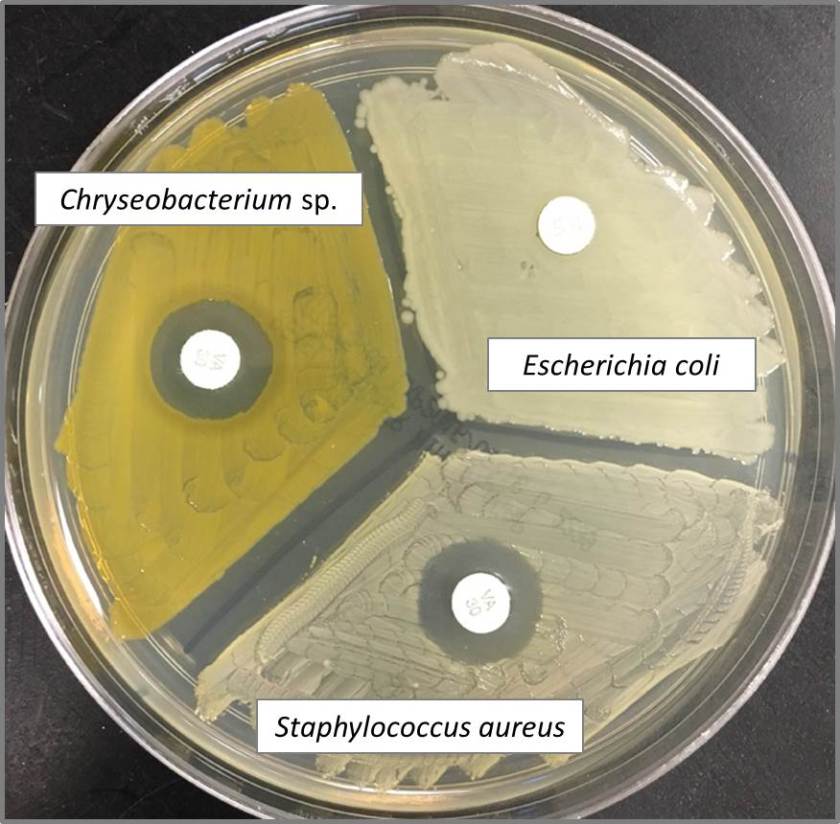
Chryseobacterium spp. have been shown to be susceptible to vancomycin in vitro (Image 3). This is a bizarre trait because they are Gram-negative bacteria, a group which is generally intrinsically resistant to vancomycin. The “susceptible” phenotype is based on Kirby Bauer disk diffusion testing, which was found not to correlate well with vancomycin MIC testing. In vitro studies found Chryseobacterium to be susceptible to vancomycin in 0 to 65% of isolates tested based on Gram-positive NCCLS or CLSI breakpoints. Due to this, vancomycin “susceptibility” can be used to aid in identification of the organism, but would not be an appropriate antibiotic for the treatment of Chryseobacterium spp.
Vancomycin disk diffusion profile for isolates of Chryseobacterium spp., E. coli, and S. aureus.
References
Chou DW, Wu SL, Lee CT, et al. Clinical Characteristics, Antimicrobial susceptibilities and outcomes of patients with Chryseobacterium indologenes bacteremia in an intensive care unit. J Infect Dis. 2011;64:520-524.
Fraser SL and Jorgensen JH. Reappraisal of the antimicobial susceptibilites of Chryseobacterium and Flavobacterium species and methods for reliable susceptibility testing. Antimicrobial agents and chemotherpy. 1997;41(12):2738-2741.
Nemli SA, Demirdal T, Ural S. A Case of healthcare associated pneumonia casued by Chryseobacterium indologenes in an immunocompetent patient. Case reports in infectious disease. 2015;2015:1-3.
Srinivasan G, Muthusamy S, Raveendran V, et al. Unforeseeable presentaiton of Chryseobacterium indologenes infection in a paediatric patient. BMC Res Notes. 2016;9:212-217.
Contributor
-Erin Waehner, Pharm.D. PGY2 Pediatric Pharmacy Resident, Children’s Health, Children’s Medical Center Dallas.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
I attended a work shop where different people were allowed to express their views on life from their generation’s perspective. One group representative said that members of the “Millennials” generation often acted as if entitled to things in life and don’t feel as if they have to work for it. A Millennial representative spoke up. She said that she did not feel entitled, but felt a victim of broken promises. She watched the generation before her live the good life- go to school, get a job, get married, buy a house, etc. – and now she was done with school, full of debt and still living at home. The economy and the world had changed, and the life she hoped for was not the one she now faced. Listening to a different perspective was truly eye-opening, and it reminded me about an important aspect of lab safety coaching.
In conversations with long-term lab safety professionals (or those lab managers, POCT supervisors and others who share the lab safety role), I often hear about the constant frustrations with lab safety compliance. Staff does not wear PPE, they don’t follow safe work practices, or they don’t think about chemical or bloodborne pathogen safety. Some who oversee lab safety have become so frustrated that they have given up on coaching or talking to the people they are assigned to keep safe. That is most definitely an incorrect approach, and if you find yourself in that situation, it may be necessary to take a step back, look in the mirror, and notice that the problem could be you.
That’s not meant to sound accusatory, but if your lab is suffering from a poor safety culture, the best place to begin with a solution is in your head, and understanding that can be powerful. First, remember that each time you are in the laboratory and you see a safety issue that you ignore, you are seriously damaging the culture. Few are scrutinized more than those who manage the safety program in the lab, and if ignoring safety regulations is witnessed by staff, they will know how unimportant safety is in the department, and they will act accordingly. If you are burned out from years of battling the culture, it may be time for someone else to enter the safety role so that the culture is not damaged further.
Next, if you plan to remain the safety role, it may be time to examine your approach to staff. Instead of becoming frustrated with people when the need to coach arises, try to change your perspective. How a safety coaching episode will play out is largely determined by what you (the coach) are thinking as you approach the situation. It is important to remember that each time a staff member does not act in a way you wish or expect as it relates to safety, there are several possible reasons or influences on the situation, and all should be considered before acting.
Janet is in chemistry handling specimens without gloves. This alone could generate a range of negative feelings when you see this- anger, frustration, or even apathy. What are the possibilities? She was not trained properly, there are no gloves that fit her, she is having a reaction to gloves and is embarrassed to confess it, or gloves are kept in the store room and she doesn’t know the door combination. Any of these scenarios and more is possible. Your emotions about the situation are real, they can result from a broken promise (you’ve spoken to Janet before), judgement (she’s not a stellar tech anyway), or failed expectations (you recommended she be hired). However, you should not act on those emotions; there is little chance the coaching will go well. Approach Janet with a question that will start a reasonable, two-way conversation. “Hi, Janet. I notice you aren’t wearing gloves. What size can I get you?” Or “Janet, I see you are handling samples with no gloves and that is dangerous. Can you tell me why?” If this is a repeat situation, put the ball in Janet’s court. “Janet, we discussed glove use last week, but you are not wearing them. You told me you would. What’s going on?” Now the focus is on the important issue for you, Janet’s broken promise. The answer may help you understand her behavior, and help you to rectify the situation permanently. Remember to use a soft approach and a civil tone. Otherwise, the work of your thought-out coaching will be for naught.
Everyone has their own perspective. That in no way excuses all behaviors, especially failing to follow lab safety guidelines, but understanding a perspective will go far in helping you succeed with coaching those bad behaviors when needed. Think first, always act, and be the safety role model you need to be for your department. Those are the powerful steps to a strong lab safety culture.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.