Case History:
A 34 year old G3P3 woman presents with PPROM at 30+4 weeks gestational age. Her pregnancy had been complicated by fetal hydrops and intrauterine growth restriction with evidence of multiple fetal anomalies and placenta previa.
Prenatal infectious disease testing was significant for:
- CMV IgG+/IgM+
- Toxoplasmosis IgG+/IgM+
- Parvovirus B19 IgM-/IgG+
- HIV screen negative (ELISA)
- HSV IgM-
- syphilis screen negative (RPR)
- rubella immune (IgG+)
- negative serologies for Hepatitis A, B and C
- Testing for VZV was not performed
Clinically, the fetal hydrops and IUGR were thought to be due to congenital CMV. She underwent caesarian section, and a fetus was delivered with APGAR 0/1/1/2/1, with eventual fetal demise at two hours of life. The placenta was sent to the laboratory for surgical pathology examination. The mother declined fetal autopsy.
Laboratory Work-Up:
Surgical pathology received a singleton placenta (13 x 13 x 4 cm) with attached umbilical cord and fetal membranes. The placental disc weighed 346 grams (<10th percentile for gestational age). Otherwise, the placental disc, umbilical cord and fetal membranes were negative for any gross abnormalities.
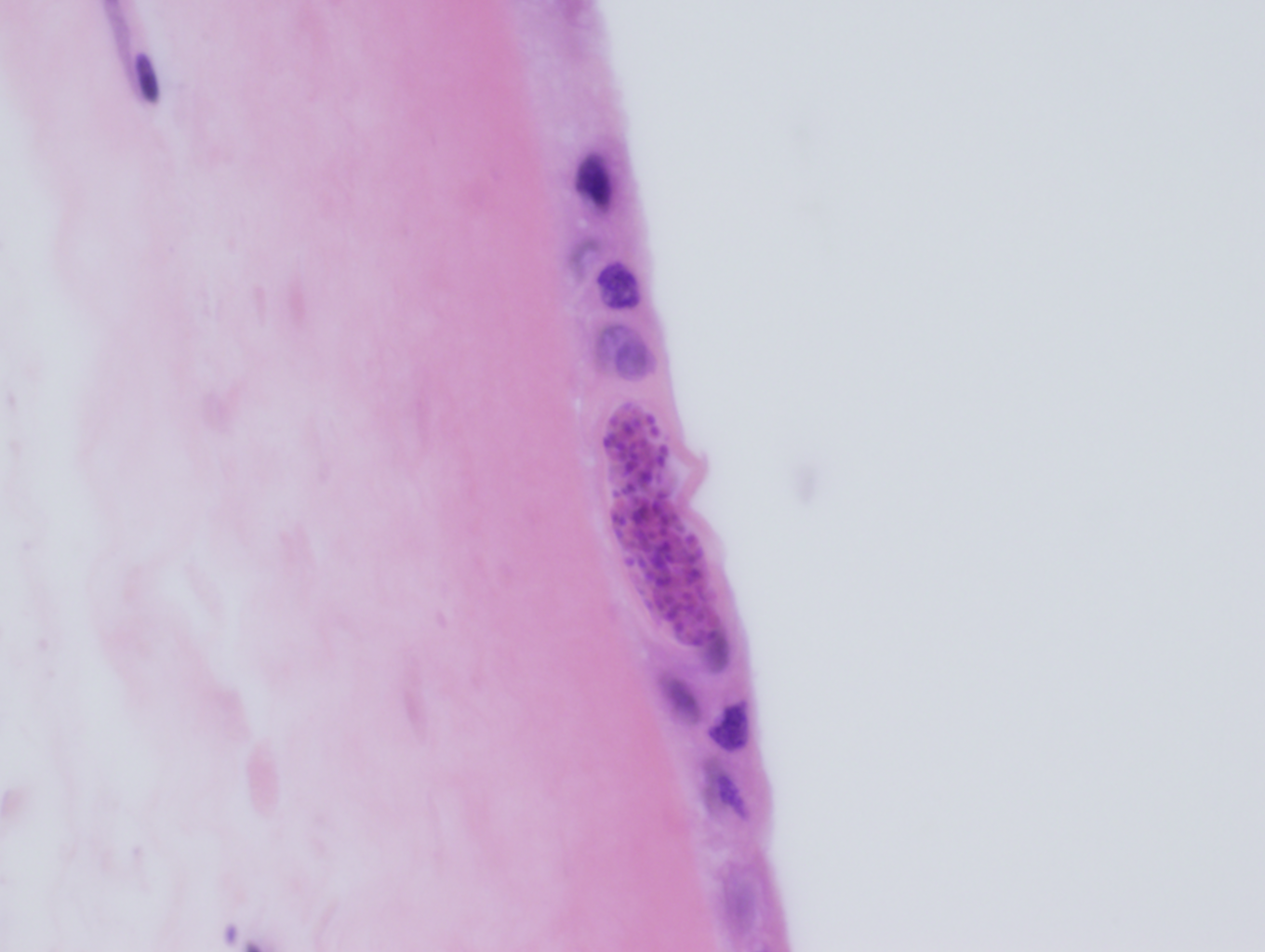
Routine microscopic sections demonstrated round to elongate cysts within the amnion of the fetal membranes (Figures 1a & 1b) and within the Wharton’s jelly of the umbilical cord (Figure 2). These cysts measured approximately 50 microns in diameter and had a thin, translucent cyst wall. Within the cysts were innumerable small round “dot-like” forms which could best be appreciated by focusing up and down through the plane of the section.
Tissue gram stain (Brown & Brenn) was negative for significant bacterial infiltrate, and immunohistochemistry for CMV was negative for CMV inclusions.


Discussion:
The histologic features are diagnostic of congenital Toxoplasmosis. The case was sent to the reference laboratory, where immunohistochemical staining for Toxoplasmosis demonstrated positive staining within the tissue cysts.
Toxoplasmosis is caused by the protozoa Toxoplasma gondii, a member of the protozoan subgroup coccidia, which also includes the GI pathogens Cryptosporidium, Isospora and Cyclospora. Cats of the family Felidae (including but not limited to domestic cats) are the only definitive host, while virtually any mammal can serve as an intermediate host. Humans can become incidentally infected in which case they act as “incidental” intermediate hosts.
The life cycle of Toxoplasma involves sexual reproduction in the definitive host (cats), as well as asexual reproduction in the intermediate host. Toxoplasma is “facultatively heteroxenous,” in that reproduction in the intermediate host is not necessary for completion of the life cycle. Unsporulated oocysts are shed in the cat feces and become infective after 1-5 days. Cats may ingest the infective oocysts, leading to sexual reproduction and completion of the life cycle within the intestinal epithelium. Alternatively, intermediate hosts such as rodents or birds ingest infective oocysts and subsequently develop infective tissue cysts. If the intermediate host is eaten by a cat, the infective tissue cysts are ingested, leading to sexual reproduction in the cat and completion of the life cycle.
The life cycle within the intermediate host involves two morphologically distinct stages, the tachyzoite and the bradyzoite. When infective oocysts are ingested by an intermediate host, they transform into tachyzoites, which are able to invade the intestinal epithelium and then widely distribute throughout the body. Tachyzoites are crescent-shaped, non-encysted and measure from 3-7 microns in length by 2-4 microns in diameter. They migrate preferentially to the muscle and neural tissues, where they eventually develop into tissue cysts, which are known as bradyzoites. Bradyzoites are much larger than tachyzoites (approximately 50 microns), are round to elongate and contain numerous “dot-like” parasitic forms encased within a thin cyst wall. Tachyzoites are eventually cleared following acute infection, but the intermediate host remains chronically infected with bradyzoites. If the host becomes immunocompromised, the bradyzoites differentiate into tachyzoites, which then recirculate through the body leading to reactivation of latent disease.
It is estimated that 10-20% of the U.S. population is chronically infected with Toxoplasma. Humans can become infected through one of five mechanisms: (1) ingestion of infective oocysts, either from cat feces or from infected water or other environmental sources, (2) ingestion of infective tissue cysts in undercooked meat, (3) vertical transmission to the fetus from a mother acutely infected with Toxoplasma, (4) through organ transplantation and (5) through blood transfusion. Epidemiologically, it is not clear whether the majority of infections occur through ingestion of infective oocysts or whether tissue cysts in undercooked meat are the major source of infection.
Vertical transmission from mother to fetus requires a first-time exposure during pregnancy. In primary/acute infection, tachyzoites widely disseminate and are able to invade the developing fetal tissues. By contrast pregnant women who are chronically infected with Toxoplasma harbor only tissue cysts (bradyzoites) and will not transmit infection to the fetus.
Acute infection is self-limited and usually asymptomatic, however some patients may have mild flu-like symptoms. A smaller subset of patients present with moderate to severe acute infection which can mimic mononucleosis: fever, sore throat, myalgias and cervical lymphadenopathy. Biopsy of inflamed lymph nodes reveals the classic histologic triad of follicular hyperplasia, monocytoid B-cell hyperplasia and epithelioid histiocytic aggregates. Once acute infection has passed, chronic infection is usually asymptomatic, unless the host becomes immunocompromised, in which case reactivation of latent disease can occur.
Treatment for immunocompetent patients in not indicated as acute infections are self-limited and chronic infection is asymptomatic. Immunosuppressed patients with CD4 counts <100 cells/mm3 should receive Toxoplasma prophylaxis with trimethoprim-sulfamethoxazole (TMP-SMX). Reactivation of latent disease can occur in immunosuppressed patients who are not taking prophylaxis, in which case first line treatment includes combination therapy with sulfadiazine and pyrimethamine.
-Javier De Luca-Johnson, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
