Case History
A 2 year old female with a past medical history of spinal muscular atrophy type 1, trach/ventilator dependency presents to the hospital with complaints of desaturations at home. She has been hospitalized four times within the past year with an additional two visits to the emergency department. Patient has history of growing Pseudomonas aeruginosa from her lower respiratory tract culture. They began to work up causes of acute desaturations: mucus plug vs. viral illness vs. tracheitis vs. bacterial pneumonia. They sent tracheal aspirate and blood for cultures. The following organism was identified as the predominant organism from the tracheal aspirate.


Discussion
Chryseobacterium spp. are non-motile, oxidase positive, indole positive Gram-negative bacilli. While often considered low virulence environmental organisms, Chryseobacterium spp. can be pathogenic in immunocompromised patients and those less than six months of age. Chryseobacterium spp. and closely related bacteria are able to survive in chlorinated water and are intrinsically resistant to many antibiotics. They are often nosocomal pathogens that are selected for in immunocompromised patients who are treated with broad-spectrum antibiotics for long periods of time. Chryseobacterium spp. have been reported to cause blood stream infections, cellulitis, pneumonia, meningitis, pyomyositis and keratitis. The most common setting of Chryseobacterium infections is foreign bodies such as indwelling catheters or prosthetic joint materials. In the adult setting, Chryseobacterium indologenes has been associated with the history of colistin or tigecycline use. Due to its low pathogenicity, Chryseobacterium spp. are generally considered contaminants in otherwise healthy individuals.
Chryseobacterium spp. have a pair of interesting resistance mechanisms. They inherently have a Class A β-lactamase and a Class B-carbapenemase that function to hydrolyze β-lactamases. Due to these mechanisms, Chryseobacterium spp. are intrinsically resistant to carbapenems and cephalosporins. Common treatment options include: levofloxacin, sulfamethoxazole trimethoprim and piperacillin-tazobactam.
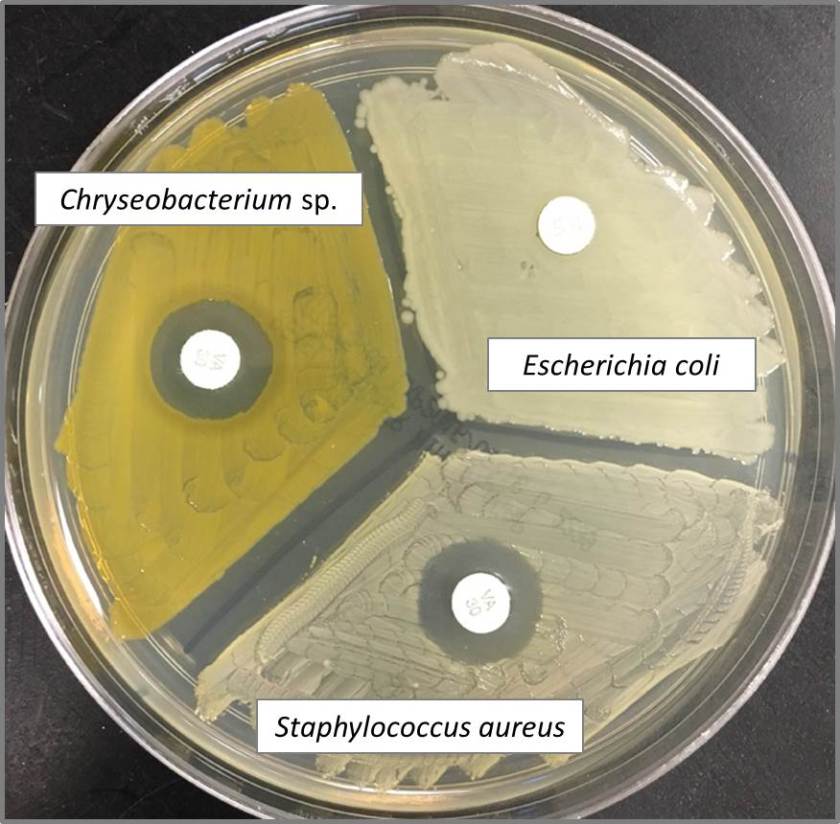
Chryseobacterium spp. have been shown to be susceptible to vancomycin in vitro (Image 3). This is a bizarre trait because they are Gram-negative bacteria, a group which is generally intrinsically resistant to vancomycin. The “susceptible” phenotype is based on Kirby Bauer disk diffusion testing, which was found not to correlate well with vancomycin MIC testing. In vitro studies found Chryseobacterium to be susceptible to vancomycin in 0 to 65% of isolates tested based on Gram-positive NCCLS or CLSI breakpoints. Due to this, vancomycin “susceptibility” can be used to aid in identification of the organism, but would not be an appropriate antibiotic for the treatment of Chryseobacterium spp.
References
- Chou DW, Wu SL, Lee CT, et al. Clinical Characteristics, Antimicrobial susceptibilities and outcomes of patients with Chryseobacterium indologenes bacteremia in an intensive care unit. J Infect Dis. 2011;64:520-524.
- Fraser SL and Jorgensen JH. Reappraisal of the antimicobial susceptibilites of Chryseobacterium and Flavobacterium species and methods for reliable susceptibility testing. Antimicrobial agents and chemotherpy. 1997;41(12):2738-2741.
- Nemli SA, Demirdal T, Ural S. A Case of healthcare associated pneumonia casued by Chryseobacterium indologenes in an immunocompetent patient. Case reports in infectious disease. 2015;2015:1-3.
- Srinivasan G, Muthusamy S, Raveendran V, et al. Unforeseeable presentaiton of Chryseobacterium indologenes infection in a paediatric patient. BMC Res Notes. 2016;9:212-217.
Contributor
-Erin Waehner, Pharm.D. PGY2 Pediatric Pharmacy Resident, Children’s Health, Children’s Medical Center Dallas.

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
