Laboratory professionals work with vendor representatives on a regular basis, and it is important to develop a good working relationship with them to ensure continued smooth operations in the department. They provide analyzers, products, equipment, and services. However, lab managers and employees may sometimes need to pay special attention to the actions a representative will take in the department or to some of the information they may provide. They should be experts about their products and processes, but they may not always be well-versed in your lab-specific process and the regulations.
One common safety mistake representatives make has to do
with proper use of personal protective equipment (PPE). Not all vendors provide
adequate PPE training, and many of the representatives may not have a
laboratory background. Check to make sure vendors wear lab coats and gloves
when working in the lab, and offer face protection if they open up instruments
for repairs or diagnostics. Some reps bring their own lab coats and use them in
different settings where they work. This is common, but it is also a violation
of OSHA’s Bloodborne Pathogens standard. PPE used in a lab should never be
taken out of the department (except as waste). Don’t let your vendor roll up his
used lab coat and place it into his work bag for his next stop. Let him know
about the regulations and offer him a new disposable coat upon each visit.
Another common issue with lab vendor reps is the use of
laptop computers and cellphones in the laboratory. In some cases, they must use
their computers to connect to instruments or to the company control center, but
they should be decontaminated before removal from the department, especially if
they were set on top of a lab counter or analyzer. Can reps use lab phones
instead of their cell phones? It’s a worthwhile question, especially if cell
phone use is against your lab policy (it should be), and if allowing vendor use
of the cell phone will be a detriment to your lab’s safety culture. Again, as
with PPE use, this safety knowledge may not be known by the vendor company, and
certainly they need education about local policies as well.
Laboratory vendors that manufacture analyzers or that design
testing processes know their products inside and out, but their set-up work and
lab staff training should be monitored, particularly if the information
pertains to local or state regulations. For example, some lab analyzers are put
in place using an extension cord for power because the analyzer cord doesn’t
reach the outlet. In many locales, the permanent of an extension cord is not
permitted. Often a vendor will train staff to incorrectly dispose of
bio-hazardous or chemical waste. That can lead to large citations and fines if
the mistakes are not caught and corrected. If a new process or analyzer
generates a new waste stream, be sure all waste regulations are being followed.
For example, if an instrument waste line is tied to a drain, contact your local
wastewater treatment center to obtain approval for drain disposal.
Labs need vendors and their representatives, they play a vital role making sure the department can provide quality patient testing and care. Be sure these valuable team members understand your operations, and provide lab safety training in order to prevent injuries or even lab-acquired infections. Ask questions, and communicate with the vendor to ensure that all lab safety procedures are being followed and that safety regulations are not violated. Keeping that eye on safety when dealing with vendors will help to ensure that the important relationships created with them will last.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Last
month we discussed the rules and requirements for how to properly perform
proficiency testing (PT) within your laboratory. In part 2 of this 3-part
series we’ll review the rules associated with evaluating your results, and how
to investigate any unsuccessful surveys. Still to come in part 3 we will look
into how to utilize your PT results to monitor for trends and shifts in your
values.
The
rules:
Performance Review: Laboratories must initiate and document a review of their PT performance evaluations within 2 weeks of notification that results are available. This includes a review of both graded and non-graded/educational analytes and events as well.
Key
things to note: Even though educational samples are not formally graded, you
should still verify the accuracy of your results, with appropriate follow-up
for any failures. CAP specifically requires you to evaluate these educational
challenges as well. Whether the sample is graded or not does not change the
fact that you had an incorrect result.
Unsatisfactory Performance: For any unsatisfactory results,
you are required to perform a root cause analysis to determine why (see below
for guidance). This also includes any clerical errors – you need to evaluate
your process and find ways to prevent these simple errors from happening again.
If they are happening with PT samples, it is possible they are happening with
patient samples as well.
Cessation of Patient Testing: Unsatisfactory events indicate
that there was a problem with that particular survey; whereas unsuccessful events indicate
there has been a pattern of unsatisfactory events/samples and a larger problem
exists. If a pattern of poor performance is detected, you may be asked by your
local state department of health to cease all testing for a particular analyte.
Key
things to note: This also applies to clerical errors. Even if there was no
technical problem with the accuracy of your results, failure to submit results
on time or clerical errors made while submitting can also have severe impacts
on your ability to continue offering that test.
Remedial Action: If you’ve been notified by your
PT provider or state DOH to cease testing, there are extensive steps that must be
completed to prove that the problem was correctly identified and corrected. You
must also identify where samples will be referred to for tests you are unable
to perform in-house.
Key
things to note: If testing has been removed from your laboratory, you will be
required to demonstrate successful performance in 2 consecutive PT survey
events for the analyte(s) in question before being granted permission to resume
patient testing. This can cause significant delays and financial impact for
your organization.
Root Cause Analysis: Investigate to determine who,
what, why, when, and how the event occurred. Be sure to evaluate all phases of
testing to ensure you identify all potential causes.
Pre-Examination:
Human Resources – evaluate the training and competency records for staff involved in the handling and testing of samples.
Facilities – reagent inventory control & storage temperatures, equipment maintenance and function checks
Standard Operating Procedures (SOPs) – staff compliance with written policies, bench excerpts are current and valid, document version control up to date
Specimen –test requisition/order entry (was the correct test code ordered/performed?), labeling (were aliquot/pour off tubes properly labeled?), transport (was appropriate temperature requirements maintained until testing performed), quality (was there visible deterioration with the sample prior to testing or cracked/damaged tubes received?), quantity (was the original sample spilled or leaking causing an incomplete aspiration of sample by your instrument?)
Examination:
Method
Validations – were instruments current with calibration requirements, any bias
noted during instrument correlation studies, values being reported within the
verified AMR
Environmental
Controls – temperatures/humidity within tolerance limits, for light sensitive
studies (bilirubin) was there excessive exposure of the samples to light prior
to testing, excessive vibrations occurring that may have affected results
(nearby construction or a running centrifuge on a shared work bench)
Quality
Control – did QC pass on the day of testing, was QC trending or shifts noted
that month
Analytical
Records (worksheets) – were sample results transcribed correctly between the
analyzer and worksheet, between the worksheet and LIS
Instrument
Errors – were any corrective actions or problems noted for the days before,
during, or immediately after testing of PT occurred
Testing
Delay, Testing Errors – were samples prepared and not tested immediately
leaving them exposed to light or air which may affect results (blood gas
samples), any errors or problems noted during testing that may have caused a
delay or affected accuracy of results
Post-Examination:
Data
& Results Review – check for clerical errors, was data trasmitted correctly
from the instrument into LIS, was data entered correctly on your PT provider
entry submission forms
Verification
of Transmission – did your results correctly upload to the PT provider website,
was there an error or failure with submission
Review
of LIS – are your autoverification rules set up correctly, is the
autoverification validation current with no known issues
Patient
Impact – perhaps
the most important step to take when reviewing PT failures, you need to
determine what impact your failure had on your patient results. Depending upon
the identified root cause and how different your values were from the intended
response, this can potentially pose a severe impact on your patient values
tested at the same time as the PT samples.
Involve
your medical director to determine if the discrepancy in results is clinically
significant. Perform a patient look-back to review patient values for the same
analyte with the failure during the time period in question. Evaluate the bias
that was present, and if deemed to be clinically significant then corrected
patient reports will need to be issued with a letter from the medical director
explaining why. If it was decided that the discrepancy is not clinically
significant, document this in writing and keep on record with your complete
investigation response.
Corrective Actions/Preventative
Actions– use the following set of questions to help guide you
in ensuring that the problem identified during your root cause analysis will
not occur again:
What
changes to policies, procedures, and/or processes will you implement to ensure
there will not be a repeat of this problem?
Do
any processes need to be simplified or standardized?
Is
additional training or competency assessment needed? If so, identify specific
team members to be trained, and who will be accountable for performing and
documenting this training.
Is
additional supervisory oversight needed for a particular area or step?
Are
current staffing levels adequate to handle testing volumes?
Would
revision or additional verification of the LIS rules address or prevent this
problem?
How
can the communication between laboratory, nursing, and medical staff be
improved to reduce errors in the future?
Continuous Process
Improvement –
after identifying the true root cause(s) for the failure and implementing corrective/preventative
actions, you need to evaluate the effectiveness of those improvements. Have
they been sustained? Are they working to correct the original problem? Have you
created new problems by changing the previous process?
Quality
Management Meetings – if necessary, increase the frequency of these meetings
during the evaluation period for timely feedback to management and staff
Implement
internal audits and quality indicators to check for potential issues
Access
the specimen transport conditions to ensure they meet test requirements
Evaluate
and monitor your turnaround time metrics to track problem specimens and impact
of testing delays
If
necessary, increase the frequency when QC is performed or calibration frequency
if stability issues are identified
Performing
a thorough root cause analysis for any failures will allow you to implement
appropriate corrective actions that will address the true issues. Having a
robust quality management program will help ensure these issues are identified
and corrected in a timely manner, and reduce the potential for the dreaded
Cessation of Patient Testing letter from your local DOH.
Coming
up in the final installment of this series on PT testing, we’ll review all of
the quality indicators and data that can be found in your PT evaluation reports
to help ensure you’re on track for accurate patient values.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018
Top 5 in the 40 Under Forty recognition program. She has worked in the
medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.
Outside the city of New Bern, in Craven County, North
Carolina, there is a particular system for residents to dispose of their
garbage. Locals must go to the nearest participating gas station and purchase
stickers which cost about $2.00 each. These stickers must be placed on each bag
of garbage generated in the household, otherwise they will not be picked up
during the weekly trash collection. In order to save money, a group of widows
has formed a club in which members scout out the open dumpsters in town
(usually behind stores or gas stations). Then they call and let group members
know where they can covertly dump their trash for free that week.
This story may seem funny, but for the most part, it is
true. I have no doubt this also occurs in other parts of the country where the
system for trash collection is similar. Why do people behave this way? Are they
purposely trying to circumvent the trash collection system in place or is the
system just not easy for locals to utilize? If you’re having difficulty getting
people to change safety behaviors (like PPE compliance) in your laboratory, you
might need to determine that for the systems you have in place and ask similar
questions.
In one laboratory the manager struggles with staff who work
part of the day in a clean office and another part in the lab itself. When the
employees go into the lab for brief periods, they often fail to don their PPE.
Upon further investigation, you would learn that staff are not allowed to keep
their lab coats on their chairs and that all PPE is kept in one lab store room
located on the opposite side away from the offices. The system is set up to reinforce
PPE non-compliance.
In another lab the manager placed a permanently-mounted
counter face shield in the chemistry department so that staff would be forced
to use it when popping specimen caps. Staff loaded instrument racks behind the
shield, but when they carried the racks over to the analyzers, their faces were
not protected from splashing. Exposures continued to occur. Here the system is
at play again. A face shield was put in place to change behaviors, but it was
only a partial solution. In order to protect staff fully here, they would need
goggles or a face shield that can be worn. Offer light-weight reusable or
disposable face protection that staff can use easily. Be sure to give them a
say in whatever option is chosen.
Sometimes the system issues are not apparent until there is
a safety event, and unfortunately, that can result in bigger problems. If your
training program does not include regular fire safety training, a small fire
situation may get out of hand quickly. Does your staff have experience handling
a fire extinguisher? Would they easily be able to put out a fire? Do they know
their evacuation routes and meeting places, and could they get there with ease?
What about the lab emergency management plan? Have staff participated in a
table-top drill so they have a basic understanding of how to respond during a
chaotic disaster? These are examples of some safety systems that need to be in
place to keep staff ready and safe at all times.
When people take shortcuts or find ways to circumvent the system, there is usually a pretty good reason, Often, it is the design of the system. In New Bern, elderly women can’t lift large heavy trash bags, so they use smaller bags. They don’t want to pay the same price for a garbage bag sticker that others are paying for big bags. There’s a problem with the system- and those ladies found a way around it. What problems do you see in your lab safety system? If you don’t know what they are, ask around. Staff will talk. It’s better to find out what the workarounds are now and to fix them before an injury or exposure occurs.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Generation Y is coming and they are coming in strong! It is
fast becoming the world’s largest working generation and their impact on the
workforce will become even clearer in the next few years. These digital natives
find communication natural, in any shape or forms it comes. They prefer texting
and instant messaging, but also appreciate face-to-face meetings and
hand-written notes. They use social media for both personal and professional
use and consider it essential to know how and where to access information.
Instant gratification has become one of this generation’s key values, because
they grew up with the world of information at their fingertips. They value
professional development and feedback and they are at work to learn and grow.
When working with a Millennial the first step is to show
them that you respect them and what they bring to the table. This generation
has received more negative attention than other generations, but they have a
tremendous amount to offer to the workplace (as do all the other generations).
They value collaboration and learning opportunities, so they are typically
quick to adjust when giving constructive feedback. Because of their
collaborative approach, they value inclusion and Social Media to bring people
together. They are well versed in finding information and can typically solve
smaller technological issues without any help.
This generation is focused on having their work mean
something, to have a purpose that is larger than simply getting a paycheck.
They dislike long email and voicemails and anything that is a waste of paper.
They appreciate flexibility and sending documents electronically. They
experiences high academic pressures, so they are comfortable working in a
fast-paced environment. They are comfortable multitasking and handling multiple
projects simultaneously.
Millennials who work in larger organizations are on the
brink of entering leadership positions. However, there are many self-starters
who have had to learn leadership skills along the way. Because this generation
values collaboration, leaders tend to encourage group work and giving people an
acknowledgement for trying. They dislike people who are afraid or do not want
to learn new technology and cynicism as they are a generally very positive
generation.
When working with Millennials, note that they respond well to a participation work environment so ask for their input and suggestions. Be open about any processes, systems, and share information freely. Provide them with lots of feedback to help them learn and grow. Millennials respond well to a faster pace work environment, so do not try to slow them down. They dislike formality and stiffness, so allow flexibility whenever possible. For example, invite them to provide input for their own goals and do not hover over them. Give them multiple things to work on simultaneously so that they can go from project to project when their energy shifts. This generation is crucial to bring your organization to the next level, so mentor them, help them grow and develop and you get their dedication, passion, collaboration, and positivity in return.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
What’s the purpose? That’s the question that most Gen Ys, or
commonly known as Millennials, ask of their job. Why am I here? Can I make a
difference in the world if I remain doing what I am doing?
The Baby Boomers worked because they felt an obligation to
put in a hard day’s work whether they liked doing what they were doing or not. It
was a job. The Generation Xers introduced a focus on work-life balance, which
was not the case for the Baby Boomer. The Boomers never heard of the concept of
“work-life balance” until their children, the Gen Xers, made it a job
requirement and reality.
As for the Millennials, they need to really believe in their
job and what they are doing. Millennials ask questions that the Boomers and Gen
Xers wouldn’t think of asking. This is often misinterpreted as being lazy or
looking for the easy way out. This is not the case. The Millennials took the
best of their predecessors. Most Millennials have a good work ethic and they definitely
look for balance. However, they’re also searching for a purpose.
My favorite story of a Millennial is centered on the importance of taking lunch at work. This topic surfaced from a Roundtable Discussion with laboratory professionals last October 2018, at the ASCP Annual Meeting in Baltimore. The actual topic for this Roundtable Discussion was “diversity.” However, that quickly changed when the nine people at the Roundtable focused on generational differences. This roundtable was rich in generational diversity. The table was comprised of Boomers, Gen Xers and Millennials. Boomers stated that they found it both necessary and easy to work through lunch. Why? It’s because they pride themselves in their incredible work ethic. The Boomers praised themselves for being better than “most Millennials” who often don’t and won’t work through lunch. Instead of that mindset, perhaps the better approach would be “What can we learn from Millennials in the work place?” That answer is “purpose and balance.”
-Catherine Stakenas, MA, is the Senior Director of Organizational
Leadership and Development and Performance Management at ASCP. She is
certified in the use and interpretation of 28 self-assessment
instruments and has designed and taught masters and doctoral level
students.
An 83 year old man with rapidly growing squamous cell carcinoma of the left temple and scalp underwent workup prior to surgery which showed an elevated PTT and a slightly elevated PT. The patient denied a history of abnormal coagulation tests or excessive bleeding or bruising. He also noted that he had previous surgeries including dental procedures without excessive bleeding. In addition, he did not have a history of clot formation.
Lab Values
Differential
Diagnosis
At
this point, the differential diagnosis for a prolonged PTT included the
presence of an inhibitor (specific factor inhibiter vs. non-specific lupus
anticoagulant) vs. reduced levels/activity of intrinsic pathway factors that
would prolong the PTT, but would not significantly affect clot formation. This
would include factors XI and XII.
Additional
Testing
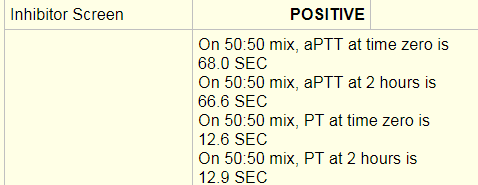
An
inhibitor screen/mixing study was performed and was positive. An inhibitor
screen is performed by mixing the patient’s plasma with pooled normal plasma
and running a PT or PTT. If the PT/PTT
corrects than the screen is negative. This means that a factor or factors were
deficient in the patient’s plasma and were replaced with the pooled normal
plasma resulting in a correction of the PT/PTT. In this case, a PTT at time 0
of 68 seconds and a PTT at 2 hours of 66 seconds was a failure to correct and
indicated that an inhibitor was present, thus a positive result was entered.
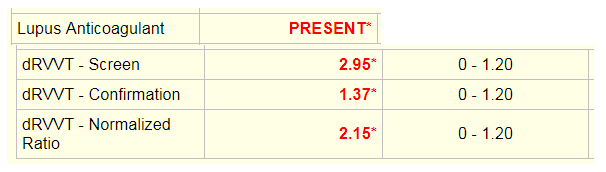
The
dilute Russell’s viper venom time (dRVVT) was used to test for a lupus
anticoagulant. The screening test is performed by adding Russell viper venom,
which directly activates coagulation factor X in the presence of calcium and a
phospholipid poor reagent to the patient’s plasma and calculating time to clot.
The confirmation test is the same assay with added excess phospholipid. In the
presence of phospholipid dependent antibodies, the time to clot will be shorter
for the confirmation test. The screen and confirmation ratios are normalized
ratios (NR) of the patient sample result in seconds divided by the mean of the
normal range in seconds. If the screen is <1.20, the confirmation test will
not be run. If the screen is greater than 1.20 as seen here, the confirmation
test will be run. The end result is reported as a normalized ratio of the
screening test over the confirmation test. If the NR is greater than 1.20, than
a lupus anticoagulant is reported as present.
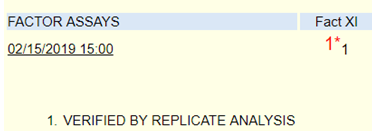
Specific
factor assays are performed by mixing the patient’s plasma with substrate
plasma that is severely deficient in the factor being measured. Factor
deficient plasma would be expected to give a prolonged clotting time. When
patient plasma is mixed with factor deficient plasma, the clotting time will shorten
and the degree of correction is proportional to the factor level in the
patient’s plasma. The clotting times for the patient sample are compared to a
reference curve. The reference curve is made with dilutions of normal plasma
(containing 100% factor) added to factor deficient substrate plasma. All tests
are run with 3 dilutions at 25%, 50% and 100% and curves are checked for
parallelism errors, which might indicate the presence of an inhibitor. For this
patient, factor XI was initially resulted as 1%, which would indicate a factor
deficiency.
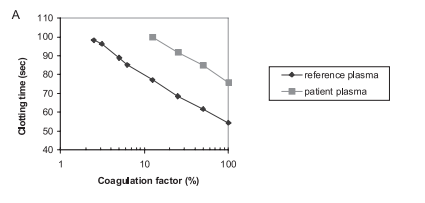
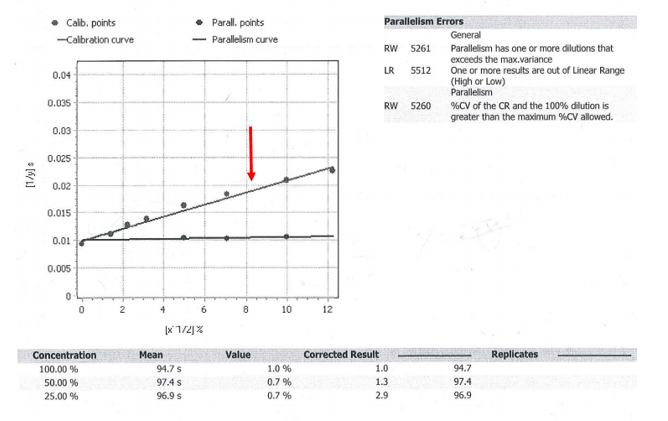
This
is an example of a factor assay that shows parallelism. The reference plasma
calibration curve and the patient plasma are parallel lines. 1
Analysis
From the
results, it initially appeared that there was both a lupus anticoagulant and a
factor XI deficiency. However, it would be odd for a patient with no reported
coagulation abnormalities to suddenly have both a lupus anticoagulant and a
factor XI deficiency. The raw data from the factor XI assay was obtained.
Upon
review, the factor XI assay did show parallelism errors. Parallelism is tested
by performing serial dilutions of a standard with known normal concentrations
of factor and recording the time to clot. This line is shown with the red
arrow. In contrast, the patient sample appears to be a flat line that is not parallel
to the calibration curve. Parallelism errors were flagged because from the 50%
to 25% dilution, the corrected results more than doubled. If there is a >20%
change between dilutions, this indicates possible interference and additional dilutions
should be run to dilute out the inhibitor. The 25% dilution had a corrected
result of 2.9, which was greater than a 20% increase from the 50% dilution
result of 1.3. Once more dilutions were performed; the Factor XI level was
ultimately close to 100%.
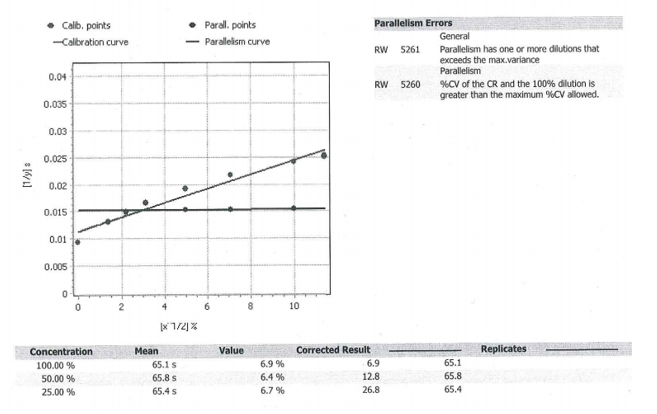
Additional
factors were checked to see if they also increased with dilutions. This would
add support to the theory of a non-specific inhibitor (lupus anticoagulant)
that was affecting all of the factor levels, rather than a specific factor XI
inhibitor or a concurrent factor XI deficiency. The curve from factor IX
(below) showed a similar phenomenon. As the sample underwent additional
dilutions, the corrected result increased significantly (from 12.8 at 50% to
26.8 at 25%). Ultimately, the factor level was close to 82%.
The
curve from factor VIII also showed low results to begin with and ultimately
normal levels with additional dilutions. Altogether, this supported the
presence of a strong lupus anticoagulant that was non-specifically interfering
with all of the factor levels and prolonging the PTT.
Discussion
A
prolonged PTT can be caused by many factors. In a patient without a bleeding
history, lupus anticoagulant and certain factor deficiencies are high on the
differential. The most common specific factor inhibitors are to FVIII and FIX.
These generally arise in hemophilia patients treated with factor concentrates.
It is very rare for a patient to develop an inhibitor to factor XI or XII.
Factor
XI acts in the intrinsic pathway of the clotting cascade and is important for
hemostasis. Deficiency of factor XI is rare and mainly occurs in Ashkenazi
Jews. Generally, it does not cause spontaneous bleeding; however excessive
blood loss can occur during surgical procedures.
Lupus
anticoagulants are directed against proteins that complex with phospholipids.
Although they prolong the PTT, they are associated with an increase in
thrombosis rather than bleeding. In addition to interfering with the PTT assay,
lupus anticoagulants may interfere with individual factor assays and result in
non-parallelism (patient curve is not parallel to calibration curve) as seen in
this patient. With increasing dilutions, the lupus activity will be
disproportionately neutralized and the coagulation factor activity will
increase in a non-parallel manner. 1
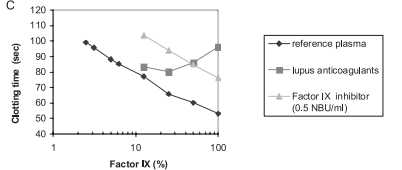
In a letter to the editor by Ruinemans-Koerts et al., they performed a set of experiments to investigate whether lupus anticoagulants vs. individual FVIII and FIX inhibitors can cause non-parallelism in the one-stage factor assay. Non-parallelism was only detected using lupus sensitive reagents in plasma with high titers of lupus anticoagulants. The FVIII and FIX inhibitor containing samples both resulted in curves that were parallel to reference sample.
This
curve shows that the factor IX inhibitor line is parallel to the reference
plasma, while the lupus anticoagulant line is not. 1
Ultimately,
this demonstrates the importance of running dilutions and being aware of
parallelism errors when performing factor assays. This is especially important
in patients with known or suspected lupus anticoagulants. In this case, the
unlikely presence of a FXI deficiency with no previously reported coagulation
testing abnormalities or bleeding history raised the suspicion of an inhibitor
interfering with the factor assay. With a concurrent positive inhibitor screen
and lupus anticoagulant test, as well as interference demonstrated with
multiple factor assays, the best unified conclusion was a strong lupus
anticoagulant. 1
References
Ruinesman-Koerts,
J., Peterse-Stienissen, I, and Verbruggen, B. ”Non-parallelism in the one-stage
coagulation factor assay is a phenomenon of lupus anticoagulants and not of
individual factor inhibitors. “ Letter. Thrombosis
and Hemostasis, 2010, p.104.5.
–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel
Deaconess Medical Center in Boston, MA. She has a particular interest in
High-grade B-Cell lymphomas and the genetic alterations of these
lymphomas.
Every
laboratory knows that they must participate in proficiency testing (PT) for all
of the regulated analytes they report. But did you know that there is more to
it than simply checking your overall score in each survey you participate in?
Whether you utilize samples from the CAP, API, or have developed your own
in-house blind sample testing algorithm, there is a lot of data available to
help you assess the quality of your laboratory program. In the first of this 3-part
series, we’ll review why PT testing is important and the rules that must be
followed. In part 2 we’ll discuss how to properly perform an investigation when
scores are <100%. Lastly, in part 3 we’ll look at how to review your results
so that you get the most out of them for a successful quality laboratory.
Why
participate? Well frankly, because you have to. It is a CLIA/CMS requirement,
and if your lab has additional accreditations, those agencies will have their
own rules and requirements as well (we’ll get to the rules in a little bit).
But outside of the regulations stating you must
participate; all labs should want to
participate. It’s an opportunity to check your accuracy against peers who are
using the same instrumentation as you. Similar to utilizing an affiliated QC
report, this is a way to see what the “real” value is supposed to be (despite
what a manufacturer may claim it to be), and how close/far off your lab is to
that true value. It can help you identify potential problems before they become
huge problems with patient values being affected, and it’s also a great way to
satisfy competency requirements for your staff.
The
rules:
Participation: For every regulated analyte being tested under your laboratory permit1, you must participate in a CMS-approved PT program2.
Key things to note: This only applies to testing performed using non-waived methodologies. Waived testing is exempt from PT requirements; although it is still recommended that participation occur if an evaluation program is available. Additionally, this only applies to your primary instrumentation. For example, if you have an automated urinalysis reader and your backup methodology is to read dipsticks manually, you are only required to participate in PT for the primary methodology. (Your backup method would then be evaluated for accuracy through semi-annual correlation studies.)
Routine
Analysis:
Unless otherwise instructed by the provider of your PT samples, PT samples are
to be treated the same as patient samples. Meaning they are handled, prepared,
processed, examined, tested and reported the same way you would perform patient
testing; AND by the same staff who would handle patient testing.
Key
things to note: If nursing staff perform a particular test within their unit
(for example, ACT testing in the cardiac cath lab), it is those nursing staff
members who must run the PT samples. You cannot have the laboratory perform PT
testing unless the laboratory also performs the patient testing. Additionally,
PT samples should be rotated among all staff members who perform patient
testing. Meaning all shifts, and all days of the week that the test is
performed – don’t let the day shift get all the fun.
Repeated
Analysis:
Similar to rule #2, unless you routinely perform duplicate testing on your
patient samples, you cannot perform duplicate or repeat testing on your
PT samples. You cannot run a PT sample in duplicate “just to make sure.” Patient
samples are just as important to be accurate as a PT sample, which is why we
participate in a PT program in the first place.
Key
things to note: After the date that laboratories are required to report results
back to the PT provider, you are then allowed to use the samples for repeat
testing. This can be used to check for uniformity in grading of reactions among
staff members, and to assess annual competency. But only after the submission date has passed.
Interlaboratory
Communication:
You cannot discuss the results or samples from a PT survey with any other
laboratory (or Facebook user group) until after
the results submission deadline has passed. Doing so before that time would be
considered cheating. The point of PT testing is not to see how good your
networking skills are, but to ensure accuracy of your own results. Plus, the
other lab may not be as good as you think they are.
Key
things to note: If your laboratory is part of a larger integrated health
system, be careful that you have separate designated staff assigned to enter
results from each location. Entering results for more than one permit number by
the same person would be considered a violation of the interlaboratory
communication rule as they could compare results from Lab A to Lab B prior to
submitting. Also, be mindful of what you put on social media. User groups are a
great networking resource and learning tool, but you still need to follow the
rules. Violating them in a public arena such as Facebook for all the world to
see would put yourself and your organization in great jeopardy if you were
caught.
Referral
of Samples:
You are not permitted to forward or share your PT samples with any other
laboratory until after the
result submission deadline has passed. Similarly, if your laboratory has
received PT samples from another lab, state regulations may require you to
notify your local Department of Health to inform them of the violation.
Key
things to note: The intended purpose of performing PT testing is to verify the
accuracy of your own laboratory testing. If you would routinely send a positive
sample to a reference lab for additional confirmation testing, you would not do
so in this case. Simply report out the values for the tests that your
laboratory performs only. The reference laboratory will have their own PT
samples to check accuracy for the confirmation testing they perform for you.
Ensure your testing menu is up to date and accurate so that your PT provider is
not expecting values for a confirmatory test if you do not physically perform
it in-house.
Records
Retention:
Ensure that all records and documents related to the testing of PT samples are
saved for the amount of time required by your regulatory agencies (typically
2-5 years). This includes instrument print outs, LIS chart copies of the filed
results, QC records for the day of testing, and any associated worksheets used
to document your results.
Key
things to note: Retaining a copy of the instrument maintenance logs and QC
records along with the actual PT results will help you investigate any scores
that are less than 100%.
Attestation: Both the laboratory director and
all personnel performing testing must sign the included attestation statement.
This is not just a way to track who performed the test, but is a legal binding
document assuring that testing was carried out appropriately as per the rules
defined above.
The penalties
for labs that are caught violating the rules (whether intentionally or not) can
be quite severe. These penalties can include the revocation of your CLIA
permit; a ban for the laboratory owner and laboratory director; as well as
possible financial penalties and fines.
Coming
up in the next blog we’ll review the rest of the rules related to evaluation of
your scored PT results, and how to perform a thorough investigation into any
unsuccessful survey events.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018
Top 5 in the 40 Under Forty recognition program. She has worked in the
medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.
The patient is a 54 year old woman, presenting to the
Emergency Room with complaints of abdominal cramps and feeling lethargic for
the past few days. She also reports her stools have been black and sticky. Her chart reveals a history of ulcers and GI
bleeding. She was transfused with 2
units packed RBCs 2 months ago for the same symptoms. CBC results are shown
below.
The patient was admitted to the hospital and four units of
blood were ordered. The patient is type A pos with a negative antibody screen.
One unit of packed red blood cells would be expected to raise the Hgb by 1g/dl.
Because the patient was actively bleeding, 4 units were crossmatched and
transfused.
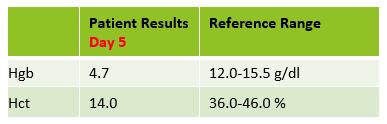
Two days later, the patient was discharged, with orders to
follow up with her GI doctor for further testing and treatment. Three days
after discharge she still felt weak and returned to the ER. On examination, it
was noted that the patient’s eyes and skin appeared jaundiced. The patient had
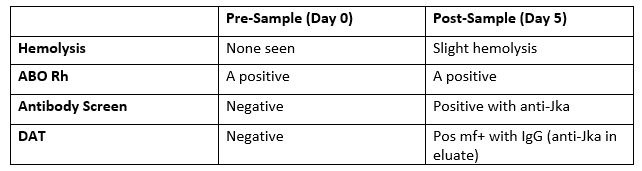
a fever of 100F. Repeat lab results are shown below.
The Physician ordered a type and crossmatch for 2 units of
packed red blood cells. The patient’s antibody screen was now positive. A
transfusion reaction workup was initiated
Transfusion workup
Clerical Check- No clerical errors found.
Segments from all 4 transfused units were phenotyped for Jka
antigen. Three of the four units transfused typed as Jka positive.
A transfusion reaction is defined as any transfusion-related adverse event that occurs during or after transfusion of whole blood, or blood components. Transfusion reactions can be classified by time interval between the transfusion and reaction, as immune or non-immune, by presentation with fever or without fever, or as infectious or non-infectious.
A delayed
transfusion reaction is defined as one whose signs or symptoms typically present
days to several weeks after a transfusion. In Transfusion Medicine, we do not
want to give the patient an antigen that is not present on their red blood
cells. However, we do not routinely phenotype patients, so, in the patient with
a negative antibody screen and history, it is always possible that the patient
receives units with foreign antigens. The more immunogenic the antigen, and the
greater number units received that expose the patient to this antigen, the
greater likelihood that the patient will develop an antibody to the foreign
antigen. Therefore, this type of reaction would also be categorized as immune.
In a delayed hemolytic transfusion reaction (DHTR)
investigation, the units transfused would have appeared compatible at initial
testing. This type of adverse event is fairly common in patients who have been
immunized to a foreign antigen from previous transfusion or pregnancy. The antibody formed may fall to a very low level
and therefore not be detected during pretransfusion screening. If the patient
is subsequently transfused with another red cell unit that expresses the same
antigen, an anamnestic response may occur.
The antibody level rises quickly and leads to the DHTR. In the transfusion reaction workup,
this antibody can often be detected when testing is repeated. However,
in some cases, particularly with Kidd antibodies, the levels again drop off so
quickly they may not be detected! The diagnosis of DHTR is often difficult because
antibodies against the transfused RBCs are often undetectable and symptoms are
inconclusive.
This case is a classical example of a DHTR. Kidd antigens are notorious for causing DHT
because their levels can drop off quickly and disappear, making them difficult
to detect in screening. In this case, the transfusion two months earlier
exposed the patient to the Jka antigen and the patient produced the
corresponding antibody. The levels then dropped quickly, as elusive Kidds are
known to do! When the patient returned to the ER in crisis, the antibody levels
had dropped below detectable levels and the antibody screen was negative. The
patient was given 4 units and returned to the ER five days after transfusion. This
patient did exhibit mild jaundice and a low-grade fever. However, often, the
only symptom of a DHTR is the unexpected drop in Hgb and Hct, making them even
more difficult to diagnose.
The new antibody screen, sent to the Blood Bank on day 5, detected
anti-Jka. The DAT was positive mixed field due to the transfused cells. Elution
was performed and anti-Jka was recovered in the eluate. In the DHTR, only the
transfused cells are destroyed. Phenotyping segments from the transfused units
can estimate amount of transfused RBCs that may have shortened survival. Management
of this case patient would be to provide antigen negative units for all future
transfusions.
Kidd (Anti-Jka
and Anti-Jkb), Rh, Fy, and K have all been associated with DHTR and
occur in patients previously immunized to foreign antigens through pregnancy
and transfusion. These types of reactions are generally self-limiting but can
be life threatening, especially in multiply transfused patients, such as those
with sickle cell anemia. Antigen negative blood must always be given, even if
the current sample is not demonstrating the antibody in question. For that
reason, it is vitally important to always do a thorough Blood Bank history
check on all samples!
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
The Lab Safety Officer (LSO) had years of experience, and he
was proud about how far he had advanced the lab safety culture. He had focused
on fire safety for a long time because when he started, very few staff members
knew how to respond to fire drills or alarms. He studied fire regulations and
educated staff about them. He performed safety audits, looked for and corrected
potential fire safety issues, and overall felt fairly certain that he had
learned all there was to know about fire safety.
When the hospital accreditation inspector walked through the
laboratory, the safety officer accompanied her. The inspector opened a freezer
containing patient specimens in one of the specialty labs. The safety officer
had opened that freezer many times during audits, but this time the inspector
asked a staff member if anything other than serum was stored in the specimen
tubes. The staff member stated that there was methanol and other reagents added
to the tubes. The inspector turned to the lab safety officer and stated she
would need to cite the lab for inappropriate storage of flammable materials.
According to NFPA-45, a national fire code for labs using flammable materials,
these specimens need to be stored in a freezer that is designated as
explosion-proof. In all his years, the LSO had never seen that regulation. Upon
further investigation, he also learned that every laboratory refrigerator needs
to be labeled as to whether or not it is capable of storing flammable
materials.
Later during the accreditation walk-through, the inspector
noticed that the flammable cabinets in the laboratory did not have self-closing
doors. The LSO asked if that was a requirement, and if so, where was it stated.
The inspector said that self-closing doors was a requirement of the
International Fire Code (IFC), and it was required if the state adopted the
code. Again, upon further study, the LSO learned that 48 U.S. states had adopted
IFC, and he now needed to consider replacing his flammable storage cabinets
with self-closing units.
When the auditor reviewed the lab’s Exposure Control Plan,
she asked how education about Bloodborne Pathogens was given to the staff. The
LSO was happy to show the inspector staff education records which showed that
every employee viewed a mandatory computer-based training program which covered
all aspects of bio-hazard education. When the inspector asked how employees
could inter-actively ask questions about bloodborne pathogens as required by
the standard, the LSO could not answer. When he researched the OSHA standard,
he found the requirement, and he told the inspector he would work with the
hospital to figure out how to make the changes to their annual education.
As you might imagine, the safety officer wasn’t feeling
quite as proud of his lab safety program after this inspection. In fact, he
felt more than a little surprised that after so many years in the field that
there was so much he still had to learn about lab safety regulations. He was
disheartened, but he was able to turn that feeling around into a resolve to
make the necessary corrections, to learn more about the regulations, and to
continue to make improvements to the lab safety program.
One of the benefits of having an outside auditor come through your lab is having that new set of eyes in an area that you may see every day. Maybe the inspector has a very different background- perhaps they were a fire inspector previously – and they can enlighten you about specific regulations you hadn’t considered before. Be sure to look at audits as an educational opportunity, even if (or especially if) you receive several citations you were not expecting. The world of safety is always changing, and there will be changing regulations and other regulatory agencies you just didn’t know about. Take that as an opportunity to learn, to grow, and to always be working to improve your lab’s safety culture.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
When I was considering the Chief Medical
Officer role at ASCP, there was significant travel on the table. Prior to ASCP,
I was already a seasoned traveler, having been to every continent except
Antarctica. I had a few travel tricks up my sleeve. However, the nearly 2 weeks
per month that I find myself out of the ASCP offices have evolved my travel
skills from seasoned to ninja. For your enjoyment, here are some of my best
tips.
Join and explore a loyalty program. We all have frequent flyer miles with one or more airlines; however, consistent use of a single airline or group of airlines (Star Alliance, Sky Team, etc) will rapidly add up and provides perks and benefits you may have to research a bit. Most importantly, don’t get discouraged by one bad flight and switch! They are called loyalty programs for a reason. In addition to upgrades, lounge access, early boarding, and free premium snacks, perks like premium economy for the same price as economy make a huge difference as planes seats get tighter.
Book economy, fly business. Economy non-refundable tickets are the least expensive typically, especially when booked on a Tuesday. If you’re booking a common business commuter flight (Chicago to NYC, Boston to DC), make sure you’re staying over a Saturday and watch prices to book effectively over time. Typically, business customers book last minute (paying highest prices) so prices are lower when booked very early; however, commuter flights are often packed with business travelers so booking early may not always be cheapest. When you get to the airport, ask if upgrades to business are available when you check in but be patient! Booking the upgrade at the gate desk is often significantly cheaper. Set a limit for yourself. “I won’t upgrade unless the cost is less than $XXX.” This will keep your personal budgeting in check and not let your exhaustion or irritation with your last economy leg lead to something rash.
Plan ahead. If you’re planning a vacation, especially a long flight (not a typical business flight), research prices way ahead of time and watch them for some time. There are websites into which you can load your favorite flights and received pricing alerts. Even if you’re a business traveler (for example, attending conferences), you’ll likely know the dates early and be able to do the same. The earliest flights of the day are often the cheapest but remember the opportunity cost to you of having to get up extra early (especially if hauling little ones!).
Carry on. Don’t check a bag. There are exceptions but, for the most part, don’t check a bag. Consider the laundry services at your hotel or access to laundry machines. When you are packing, lay everything out and ask yourself, “Am I going to die if this is not with me?” If the answer is “no,” move to the “maybe” pile. If you’re bringing gifts, carry them in a reusable sack as your personal item. Speaking of reusable sacks, organizing your back pack with a few of these means you can pull out “computer” or “clothes” or “other” quickly and replace them easily (it’s like file folders). If you are going on a big trip and just can’t do without a checked bag, try to fly direct and/or make sure you have a full one hour (domestic) or two hour (international) layover between flights— both will increase the likelihood of your luggage arriving. If you are a business traveler, INVEST in a very good carryon bag. Because carryon luggage at the low end of the scale is assumed to never be checked, one bad flight can destroy it.
Toiletries. I know you have a strict beauty regiment with 12 products you can’t live without but consider lightening your load when possible. All hotels provide basic toiletries and there are stores everywhere (clearly, if you’re vacationing or working very remotely, there may be limitations, but remember context and consider the essentials). Most large format toiletries have to be checked and that’s adding challenges you don’t need. Some of my pro-travel colleagues who MUST have their complete hygiene system check bags but always use the suggestions I mention above about checked bag security. A clever, lovely friend of mine once said (when I asked why she was wearing only mascara in the middle of Africa), “If I just have this one thing I do every morning, I feel normal.” Sound advice.
Security. There is general anxiety about going through security but there doesn’t have to be. First, it’s for your safety and, unless you are a criminal or a terrorist, the security people are there for your protection and they are quite nice. Second, if you get TSA pre-check, know the drill. Nothing infuriates fellow travelers like a confused passenger in the TSA pre-check line disrobing and regurgitating the contents of their bag into a bin. If you’re not TSA pre-check, be ready to remove coats, shoes, laptop, belt, all pocket contents, and sunglasses. You can do all of that during your 10 + minute waiting in line. You should not do it when you get to the table—that’s why the line is so long. Third, when you travel internationally, the rules are always different but the security agents are still just human beings doing their job. Politeness and paying attention will make all the difference. Fourth, some of us are more likely to experience friction with security because of the way we look, our clothes, or even our perceived attitude. It’s not right, it’s not fair, and it’s annoying… but we know this and can prepare for it. Displaying courtesy and politeness at all points in the airport will get you through security quickly. If you happen to have a difficult experience, I encourage you to send a strongly worded, formal letter later (you can write it on your smartphone on the plane… just don’t send it until you are back home). There is no point in ruining your trip over someone else’s potential unfounded fear or ignorance. Lastly, I understand the world is liberated (being liberated) and we all think we have the freedom to do as we wish l; however, showing up to a security check point drunk or stoned or reeking of pot will get you heavily screened and searched. The rest of us enjoy the show but not the delays.
Boarding. The bin above your seat is not assigned to you. The space under the seat in front of you is. The bin above your seat is determined to be full by the crew, not by you. Other peoples’ bags are going to touch yours. The crew can and will place your bag correctly in the overhead bin. When you find your seat, quickly store your bags and sit quietly with your seatbelt unfastened and your hands in your lap. Don’t pull out your laptop. Don’t have 5 things in your hands and in the seat pocket. Your personal item under the seat in front of you should contain anything you’ll need during the flight. Organize yourself at home before you depart—not while the rest of the plane is trying to board. People will like you. The crew will like you.
Seat selection. If you know you get up frequently to use the restroom normally, book an aisle seat. If you pass out on airplanes at takeoff and wake up at landing, book a window seat. If you are in a middle seat (someone has to be), it’s frustrating but it does not entitle you to more space than the people on either side of you. Booking early and checking in early is the best way to score a window or an aisle. We are all trapped on the same plane and courtesy wins the day. If you are rude or discourteous, the crew will notice and you will have a miserable flight.
Jet lag. It happens. It’s terrible. It can take you out for a day or more of your trip. There are apps and websites that explain how to avoid, reduce, or beat jet lag. But each person’s physiology is different and these remedies may fail. Common chemicals used include melatonin and caffeine. You’ll have to find your own way of coping but, for fun, here is mine. First, sleep when it’s dark and stay awake when it’s light. Avoid napping during the day. Second, if you are on an overnight flight to an earlier time zone (US to Europe), do your best to sleep on the plane. I don’t recommend drugging yourself but earplugs and an eye mask can do the trick. Lastly, the first night you are in your final destination and about 1.5 hours before bed, run a hot bath and drink a very cold beverage (beer is my preferred coolant but anything cold, with calories, and no caffeine will work). Turn the AC down to a low setting so the room is chilly (even if it’s winter).The hot bath relaxes your muscles, shifts your blood flow, and tells your brain to cool down your body. The cold liquid helps do this. Why? We are naturally diurnal and our bodies are warmer when we are awake than when we are asleep (and the switch is related to light cycles and perceived time of day). After the bath, don bathrobe or towel and sit in the cool room for 15 to 30 minutes so your body dries with water on it (more cooling effect!). Now that you are chilled, crawl in bed and sleep. As I said, this works for me and it may not work for you. And, of course, it requires a bathtub.
Consumption. Drink plenty of water. Deep vein thromboses are no laughing matter. Being well hydrated and getting up to use the restroom a few times is actually good for you. Don’t drink tea or coffee on an airplane (google it to see why). If you’re on an international flight and the alcohol is free, pretend you’re at your grandmother’s house. A glass of wine or a cocktail are fine but becoming inebriated will do you no favors. It can also cause you to sleep when you shouldn’t and it dehydrates you. Make your own choices about eating food on the airplane. It’s often hit or miss so my decisions are made in real-time.
Here’s some
self-explanatory one-liners to wrap up:
Wear comfortable, slip on shoes
Loose fitting pants (with belt)
Leave you giant pillow at home
Headphones! No exceptions
Ziplock bags to organize electronics
Always have a pen
Seats are for people, not bags
Understand time zones in advance
Learn “Hello” and “Thank you” in the local language
Carry at least two universal travel adapters
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
Generation X is sandwiched between the two largest generations alive today: Baby Boomers and Generation Y/Millennials. This means that Generation X will never be the largest generation at the workplace, but even so, their impact is significant. Gen Xers are in a unique position as they started their careers relatively recently and can understand the challenges Millennials face, while also starting to enter leadership positions and can therefore relate to Baby Boomers.
One of the things that make Generation X stand out from
other generations is that many of them have young children and aging parents.
This means that having a work-life balance is important to them as they often
have responsibilities to take care of their family members. They typically also
prefer a divide between their personal and work lives. This is not to say that
they do not make friends at work or not hang out with colleagues after work,
but they tend to have a “business first” approach to their work relations.
When working with Generation X, note that they appreciate it
if you use their time efficiently. When presenting an idea of have a meeting
with them, make it as productive as possible and focus on what is in it for
them. Gen Xers value brevity, fast turnarounds, and efficiency. This is a stark
contrast with Baby Boomers, who focus on interpersonal relationships before
getting a task done. Making your communication, whether it is in-person, over
the phone, or via Gen X’s preferred mode of communication (email), as concise
and to the point as possible will increase your effective collaboration with
this generation.
As leaders, Gen Xers dislike micromanagement, both as a leader and as a follower. Their leadership style revolves around trusting others to get the job done and they expect the same courtesy in return. They value people doing what they say they are going to do, so do not promise Gen Xers that you will do something if you know you cannot. Their leadership style is therefore quite informal as they expect people to follow deadlines and get the job done, while giving their workers a high degree of freedom.
Generation X is an efficient generation who hate wasting time with empty words, promises, and incompetence. They appreciate immediate actions, a focus and straightforward approach to work without long social interactions. They respect child-friendly environments, such as being able to have a flexible schedule that allows them to accomplish their professional tasks while also taking care of their family members. They can brief and blunt, but they have an authentic and results-orientated approach to work. If you work with a Gen Xers, give them freedom to do their work and explore and only make promises you can keep. Keep your emails and interactions to the point and follow up quickly after a meeting. Having an efficient but friendly approach will take you far with this generation.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
So what does working with a Gen Xer really mean? Does it
only apply to the laboratory, or do we work with people outside of the
laboratory? Hmmm. How about our family, friends, social and community
relationships? That said, I took this question to the streets as well as the
laboratory and asked these questions.
Boomers, what’s it like working with a Gen
Xer?
Gen Xers have a good work ethic; however, their family often
ranks higher than their job. Boomers pride themselves in their work ethic. The
Gen Xers are still so busy taking care of their aging parents, as well as,
their kids, even when they’re off at college. They are the “Sandwich
Generation.”
Millennials, what’s it like working with a
Gen Xer?
I took this question to the classroom where I teach. My
students are all working on their Masters Degree, and by the way, I have three
Gen Z students in my class. Both the Millennials and Gen Z students found that
the communication with a Gen Xer is different. The stated that the Gen Xers use
email, messaging and Slack. As a Boomer, I didn’t know what Slack was! The
Generation Y and Z students felt that the Gen Xers were resistant to change and
to some technology.
One Millennial by the name of Erika shared that she found
Gen Xers relatable and at ease. I found her most profound statement to be that
she said the Gen Xers seemed like they were in-between and strike a balance
between the Boomers and the Millennials. Hmmm…. They are known as the “Sandwich
Generation” because they are often taking care of their parents and their
children, but it’s interesting Erika saw them “sandwiched” in a different way.
Time to hear from
our Gen Xers and how they feel about working with the Boomers and Millennials.
Gen Xers, what’s it like working with the
Boomers and Millennials?
My first Gen
X interview came from a regional director of a Beverage Company. As a Gen Xer,
he felt that he was more effective working with the Boomers when the
communication was face to face, or on the telephone. Emails worked, but he
definitely noticed the Boomer preference. On the other side of the coin, this
Gen Xer found that the Millennials who worked for him or with him preferred the
technology communication.
The Gen X laboratory
professional I interviewed found the Boomers resistant to change. This was
interesting because this is how the Millennials felt about the Gen Xers! Again,
is this the “Sandwich Effect!” Overall, this Gen Xer appreciated the depth and
vast knowledge of the Boomer and how they wore that hard work as a badge of
pride.
Lastly, on a
high note, the Gen X laboratory professional really appreciated the Millennial’s
enthusiasm. The grass doesn’t grow under their feet in the work place. If they
perceive there’s no place to climb the ladder, they’re off and running. The Gen
Xers let go of the “Boomer Job Loyalty Program,” however, they are more stable
than the Millennials in the work place. Again, they possess the gifts from the Boomers
and Millennials. They are “The In-betweeners!”
-Catherine Stakenas, MA, is the Senior Director of Organizational
Leadership and Development and Performance Management at ASCP. She is
certified in the use and interpretation of 28 self-assessment
instruments and has designed and taught masters and doctoral level
students.