The patient is a 54 year old woman, presenting to the Emergency Room with complaints of abdominal cramps and feeling lethargic for the past few days. She also reports her stools have been black and sticky. Her chart reveals a history of ulcers and GI bleeding. She was transfused with 2 units packed RBCs 2 months ago for the same symptoms. CBC results are shown below.

The patient was admitted to the hospital and four units of blood were ordered. The patient is type A pos with a negative antibody screen. One unit of packed red blood cells would be expected to raise the Hgb by 1g/dl. Because the patient was actively bleeding, 4 units were crossmatched and transfused.
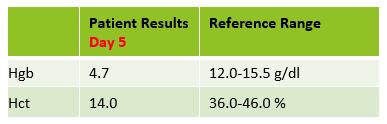
Two days later, the patient was discharged, with orders to follow up with her GI doctor for further testing and treatment. Three days after discharge she still felt weak and returned to the ER. On examination, it was noted that the patient’s eyes and skin appeared jaundiced. The patient had a fever of 100F. Repeat lab results are shown below.
The Physician ordered a type and crossmatch for 2 units of packed red blood cells. The patient’s antibody screen was now positive. A transfusion reaction workup was initiated
Transfusion workup
Clerical Check- No clerical errors found.
Segments from all 4 transfused units were phenotyped for Jka antigen. Three of the four units transfused typed as Jka positive.
A transfusion reaction is defined as any transfusion-related adverse event that occurs during or after transfusion of whole blood, or blood components. Transfusion reactions can be classified by time interval between the transfusion and reaction, as immune or non-immune, by presentation with fever or without fever, or as infectious or non-infectious.
A delayed transfusion reaction is defined as one whose signs or symptoms typically present days to several weeks after a transfusion. In Transfusion Medicine, we do not want to give the patient an antigen that is not present on their red blood cells. However, we do not routinely phenotype patients, so, in the patient with a negative antibody screen and history, it is always possible that the patient receives units with foreign antigens. The more immunogenic the antigen, and the greater number units received that expose the patient to this antigen, the greater likelihood that the patient will develop an antibody to the foreign antigen. Therefore, this type of reaction would also be categorized as immune.
In a delayed hemolytic transfusion reaction (DHTR) investigation, the units transfused would have appeared compatible at initial testing. This type of adverse event is fairly common in patients who have been immunized to a foreign antigen from previous transfusion or pregnancy. The antibody formed may fall to a very low level and therefore not be detected during pretransfusion screening. If the patient is subsequently transfused with another red cell unit that expresses the same antigen, an anamnestic response may occur. The antibody level rises quickly and leads to the DHTR. In the transfusion reaction workup, this antibody can often be detected when testing is repeated. However, in some cases, particularly with Kidd antibodies, the levels again drop off so quickly they may not be detected! The diagnosis of DHTR is often difficult because antibodies against the transfused RBCs are often undetectable and symptoms are inconclusive.
This case is a classical example of a DHTR. Kidd antigens are notorious for causing DHT because their levels can drop off quickly and disappear, making them difficult to detect in screening. In this case, the transfusion two months earlier exposed the patient to the Jka antigen and the patient produced the corresponding antibody. The levels then dropped quickly, as elusive Kidds are known to do! When the patient returned to the ER in crisis, the antibody levels had dropped below detectable levels and the antibody screen was negative. The patient was given 4 units and returned to the ER five days after transfusion. This patient did exhibit mild jaundice and a low-grade fever. However, often, the only symptom of a DHTR is the unexpected drop in Hgb and Hct, making them even more difficult to diagnose.
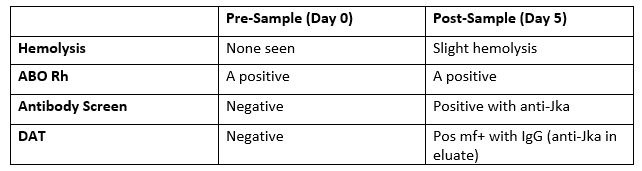
The new antibody screen, sent to the Blood Bank on day 5, detected anti-Jka. The DAT was positive mixed field due to the transfused cells. Elution was performed and anti-Jka was recovered in the eluate. In the DHTR, only the transfused cells are destroyed. Phenotyping segments from the transfused units can estimate amount of transfused RBCs that may have shortened survival. Management of this case patient would be to provide antigen negative units for all future transfusions.
Kidd (Anti-Jka and Anti-Jkb), Rh, Fy, and K have all been associated with DHTR and occur in patients previously immunized to foreign antigens through pregnancy and transfusion. These types of reactions are generally self-limiting but can be life threatening, especially in multiply transfused patients, such as those with sickle cell anemia. Antigen negative blood must always be given, even if the current sample is not demonstrating the antibody in question. For that reason, it is vitally important to always do a thorough Blood Bank history check on all samples!

-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.

Thanks for sending some Transfusion Medicine cases. Retired from 45 years in the Blood Bank and enjoyed reading them.
Glad you enjoy them. Watch for them every other month!
Thank you Becky Socha, for this interesting case study and I loved your additional information and explanations. I am currently in a BB course for my MLT-MLS program (at APSU) and I have used the basic information from this case for my education. I have cited you and this website, I hope that this will be okay. I now have found this wonderful site for techs and I am excited to read more studies on other subjects. I hope to read more from you again in the future as I explore this amazing blog page!
I was thinking about during this patient’s ER visit with known transfusion history 2 months prior, would it be possible to microhematocrit centrifuge or use hypotonic saline to wash her blood to separate the two cell populations and phenotype both populations to find any discrepancies in different RBC antigens? Also, after 120 days or so when all Donor cells are most likely cleared, she should probably have further testing done to get an accurate antigen and antibody profile, so that when she possibly has another GI bleed in the future, they will have more information on her along with transfusion history.
I have never worked in blood bank yet. I commend all who do as I do not think I could take that kind of pressure. But I find the process both fascinating and complicated/frustrating (with clinically insignificant antibodies causing many issues and interferences in testing!). I am a micro tech at heart, currently working in immunochemistry and general chemistry.
Thank you again!
Maya R.