The current pandemic has highlighted the importance of the laboratory in the delivery of healthcare. Patients and families depend on the laboratory to delivery accurate and timely results. Regulations have been written to ensure laboratories meet society’s expectations. Medical laboratories are one of the most highly regulated industries requiring biennial inspections by accrediting agencies. Despite operating under the COVID-19 testing pressures, laboratories still need to be inspection-ready.
New Inspection Process
As a result of social-distancing mandates and state-level restrictions, laboratories need to adjust to a new inspection environment. The College of American Pathologists (CAP) is temporarily allowing virtual inspections and has created information on its website about a few laboratories’ experiences with the virtual inspection process.
The CAP has also shared some expectations laboratories should be aware of when discussing inspection aspects.
Currently, in states where there are travel restrictions with quarantine requirements, a greater than 5% positivity rate, or where the institutions have travel/visitor restrictions, the laboratory medical director may choose to have a virtual inspection. However, the laboratory should be aware that they will still be required to have an in-person on-site inspection within 4-6 months if virtually inspected.
In addition, the laboratory director and the inspection team must both agree to perform a virtual inspection.
Virtual Aspects
Laboratories should take into consideration some of the aspects of a virtual inspection. In-person inspections for many small to medium laboratories often consist of inspectors being on-site for only one day. Conversely, virtual inspections can be weeks or even a month in duration depending on the laboratory’s size, the number of specialties, and the inspectors’ availability.
Virtual inspections also require a lot of document handling. Laboratories utilizing manual worksheets, quality control and troubleshooting logs will need to upload these documents for review. The CAP has created a secure website for this purpose, but it still requires personnel to scan each document individually.
Technical Priorities
There is also the risk of technical issues hampering the virtual process. Laboratories must have reliable Wi-Fi, electronic communication devices (laptops, tablets, cameras) and have personnel comfortable with the challenges inherent in managing multiple requests simultaneously. Having a dedicated IT person for an inspection is a great but difficult to get asset.
Mult-day Inspection
If there are no limiting COVID restrictions, laboratories may still opt for an in-person inspection.
Some inspection teams (in agreement with the laboratory medical director) have modified the in-person inspection process so that it is conducted over a 3-4 day time period. In this process, only a few inspectors come on each day to inspect specific disciplines. Usually, one inspector will return the next day to provide some continuity to the inspection process.
Instead of an intense one-day process, spreading an in-person inspection out to 3-4 days allows the team and facility to practice social distancing, reduces the level of stress, and gives the laboratory more time to provide evidence or have a deficiency changed to “corrected on-site.”
Competency Note
Laboratories need to be reminded that regardless of COVID, the requirements for competency still apply. New hires must still have semi-annual competencies performed at the required frequencies, and the laboratory must be able to provide competency documentation during an inspection. There are no exceptions to the competency mandate.
Conclusion
It is expected laboratory administrators and managers may have a bit of angst regarding the uncertainty that comes with a new inspection process affecting the entire laboratory. Amid the COVID crises, the laboratory has been tasked to deliver high-quality results efficiently. Laboratories across the nation have met the COVID challenge and are able to adapt to the demands inspections require. Virtual inspections are just another example of the laboratory adapting to meet its regulatory and accrediting requirements.
-Darryl Elzie, PsyD, MHA, MT(ASCP), CQA(ASQ), has been an ASCP Medical Technologist for over 30 years and has been performing CAP inspections for 15+ years. Dr. Elzie provides laboratory quality oversight for four hospitals, one ambulatory care center, and supports laboratory quality initiatives throughout the Sentara Healthcare system.
Laboratorians struggled through 2020 but successfully navigated a difficult situation while maintaining and improving our high-quality service to our patients. By laboratorian, I mean all of us—medical, public health, research, industry, etc.—because, across all sectors, anyone working in a laboratory (our family) was pushed to the limits to do more with less, work harder with fewer people, provide results with challenging procedure standard, and save lives while risking our own. It is quite easy to go into a clinical laboratory that is providing COVID-19 testing and find heroes that were there before, excelled during this pandemic, and will be there tomorrow. But there were heroes in every laboratory. Our public health laboratorians spent tireless hours trying to provide testing, coordinate testing, disseminate information, and relay the best current epidemiology to leadership to keep the country running. Our research laboratorians developed and delivered data, new information, novel biology, and potential interventions for the novel coronavirus. Our industry laboratorians were crucial components to vaccine development and delivery. And, unlike most of the country, our laboratorians were not able to “work from home” because, well, there are laws against having certain things in your house that might escape and kill your neighbors. It is good to be essential, but it has it pain points. Our laboratorians have felt that pain by still commuting to their benches to get the work done every day. But they did it and did it well! And what is often forgotten is that every single one of these laboratorians already had a “day job” in delivering a full catalog of laboratory-based services to which they added a successful COVID-19 response. If you see a laboratorian after you read this blog, you should want to hug them and say thank you.
Vaccination is spreading and will overtake and conquer this virus in parallel with our continued social distancing, hand washing, and mask wearing. In the background, testing will continue and will drive how our leaders make decisions more than anything else. We can see an end to this bedlam and are now facing, perhaps, one of the most difficult questions we have ever faced as a global laboratory community: “What do we do now?”
Our pathologists, long awaiting the day when digital telepathology was the norm, were thrust headfirst into that practice during the pandemic under emergency conditions. Many of them had already started (sometimes in a big way) but others were pushing glass routinely. Many of us have leapfrogged to a place from which we cannot return. We need to evaluate the virtual practice of the past year to determine the error rates and see if it is comparable (or better) than our routine glass slide practice. Is eBay or LetGo going to be overwhelmed with microscopes while high resolution monitors go into backorder? We must still contend with the requirement of “presence” and the moniker of “CLIA”, which was temporarily separated from a pathologist’s role in care during the pandemic. These new digital practices may address our long-standing workforce shortages. Working from home was not a possibility but a requirement for much of the last year. Care continued and work was done. What evidence would argue that working in an office is “better” than working from home when we consider the practice of pathologists? The financial implications of cost per square foot of overhead when taking up space in an academic medical facility is more than sufficient for a CFO to argue that pathologists working from home is great. But this is assuming that the workstation, the workflow, and the outputs were optimized. Not all pathology laboratories went fully digital and there was a great deal of slide shipping/couriering. On the other side of this pandemic, much like the 6 to 10 different platforms found in a clinical lab to perform a COVID-19 test, we will find that many practices are not sustainable, can be replaced and optimized, and will require more upheaval and pivot from our pathologists. To clarify, before COVID-19, pathologists practiced basically the same anywhere in the world; namely, review of glass slides in slide folders with a connected case file. During COVID-19, a whole new set of options emerged for how we would do that routine work that were uncontrolled and ad hoc. Now on the other side, we must separate the practices that are best for patient care from those that got the work done in a crisis to find our way forward. If the optimal model is (and I am not saying that it is) digital telepathology from anywhere, we must work hard to define “anywhere” for the sake of our patient’s care and safety. Monitor or other devices standards, which have long been the bane of the telepathology community, are still not standards. CLIA is specific about what constitutes a laboratory and its four walls. Accreditation teams do not inspect people’s home offices. On the other side of this pandemic, how do we find a common, best practice in a virtual age? We must return to a state of highest possible quality for our patients without giving up the advances we made in this crisis.
I once wrote up a laboratory revision plan for a firm that had 9 hospitals. Each had its own pathology laboratory employing 1 to 3 pathologist and similar staff for grossing, histology, and admin. Each laboratory had a volume of less than 3000 samples per year (and referred complex cases to a tertiary care center out of network). Based on our revision, in formalin concentration and recycling alone, the system would save $100,000. With a centralized laboratory (easily capable of handling 30,000 samples per year) and a digital pathology strategy, the work could be done by half the number of pathologists. Most importantly, the reagent/supply savings from having one laboratory rather than 9 was astronomical. The bottom line was an increase in revenue of nearly $1,000,000 with a cost savings of more than 75%. The key element of this plan that is important here is the digital telepathology component that reduces the number of staff needed and the office space needed which, at the time of the revision proposal, was “innovative” but thought too new to be reasonable. COVID-19 has tested that one aspect of the model and found it to be more than reasonable. More importantly, laboratory management and organizational leadership has had to take a hard look at costs, cost centers, and fixed expenses in such a way that the model above now becomes not lucrative but essential to staying in operation. We are trained in the laboratory to always be working on quality improvement, but COVID-19 has pushed us to always be working on fiscal improvement as well.
As we return to our “new normal” after COVID-19, the lessons we learned from this pandemic are going to translate into mergers, acquisitions, consolidations, closings, and restructurings of all types of businesses and services with the laboratory being no exception. The concept of surge capacity, for example, for testing of a new infectious agent that has emerged, has been a trial by fire, and there are many important lessons to learn from this as well. Should our approach to the next pandemic be to divert our staff from regular laboratory operations and bring into our facilities 6 to 10 new platforms for testing? Perhaps we should consider using temporary warehouse space offsite from our existing laboratory as well as backfill or relocating staffing for this crisis management to prevent complete disruption of our workflow and our policies. This is the type of solution that can exist when contingency planning is a routine part of operations. Those many facilities that were forced to bring in extra platforms are going to be facing a different crisis as test volumes crash; namely, what to do with the equipment. The firms that produce and sell that equipment have a similar challenge of expanding their platform beyond COVID-19 testing and making it relevant and competitive for the laboratories that have their extra platforms. Although I am not sure eBay or LetGo will be full of microscopes just yet, I am sure you are going to be able to pick up some nifty analyzers for an incredibly low price very soon. Will the memorial to the half-a-million we have lost in this country to COVID-19 be the useless bodies of laboratory devices that we so desperately needed in 2020? I think we owe them a lot more than that. Let us actively rethink our strategies in the laboratory and across our healthcare system so that such memorials are never needed again.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
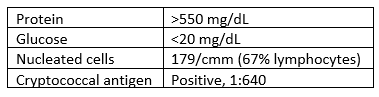
A 53 year old male with a past medical history significant for dermatomyositis, antisynthetase syndrome, and atrial fibrillation with rapid ventricular response presented with a chief complaint of worsening confusion, auditory hallucinations, and hearing loss. Pertinent medications included prednisone and mycophenolate. Head MRI demonstrated leptomeningeal enhancement and hydrocephalus. A lumbar puncture was performed, with CSF results as follows:
Laboratory Findings
CSF was sent to the microbiology lab for bacterial and fungal smears and cultures. No organisms were seen on the Gram stain.
Within 3 days, however, rare colonies of yeast were growing on both the bacterial and fungal media. The yeast was identified as Cryptococcus neoformans using the in-house MALDI-TOF mass spectrometry instrument.
Image 1. Budding C. neoformans at 1000x. Image 2. Colonies of C. neoformans on potato flake agar.
Discussion
Cryptococcus neoformans is an environmental saprophytic yeast that can be found around the world, although it is often associated with avian droppings.1 The cell is surrounded by a polysaccharide capsule that protects it from environmental hazards and, once within the host, from phagocytosis.2 Additionally, the cell wall of C. neoformans contains melanin due to the presence of the phenol oxidase enzyme, which assists in the formation of melanin from various phenolic substrates.1 Both the polysaccharide capsule and the melanin-containing cell wall can be helpful in the laboratory identification of C. neoformans.
If inhaled, Cryptococcus neoformans can cause disease (cryptococcosis) in immunocompromised patients. The most significant risk factor is AIDS, however any cause of immunodeficiency can be a risk factor, including long-term steroid therapy, organ transplantation, malignancy, and liver disease.1 Once inhaled, the organism spreads hematogenously and tends to favor the central nervous system, causing cryptococcal meningoencephalitis.1
Prognosis for patients with cryptococcosis can vary widely. In AIDS-associated CNS cryptococcosis, predictors of mortality include abnormal mental status, cerebrospinal fluid antigen titer >1:1024 by latex agglutination or >1:4000 by lateral flow assay, and CSF white blood cell count <20/µL.1 The prognosis for patients who are immunocompromised for other reasons depends on the cause of their immunosuppression.1
Treatment of patients with cryptococcal meningoencephalitis consists of an induction phase with amphotericin B and flucytosine followed by a consolidation phase with fluconazole then a long-term maintenance phase with a smaller dose of fluconazole.3
References
Jobson M. Microbiology and epidemiology of Cryptococcus neoformans infection. In: Post T, ed. UpToDate. UpToDate, Inc. Accessed March 13, 2021. https://www.uptodate.com
Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2010;50(3):291-322. doi:10.1086/649858
-Michael Madrid, MD is a 1st year Anatomic and Clinical Pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
Hello everyone and welcome back! Thank you to all those that read the previous piece on life and loss, personal growth, and—of course—vaccines. This month, let’s explore something relatively new on the horizon that has the potential to change pathology as we know it: The Cures Act.
Okay, well, new-“ish”; the Cures Act (114th Congress, H.R. 34) was signed into law on December 13, 2016…so you snooze, you lose I suppose. But don’t worry, this signed law faded into seeming obscurity and is now resurfacing because it’s being implemented and enforced based on some of the language of the bill. Along with supporting measures in research and innovation, the Cures Act has an aim at empowering patients with health record accessibility.
Image 1. Outlined here in a graphic from The Office of the National Coordinator for Health Information Technology (ONC Health IT), are the three major take-home points of how the Cures Act will affect patient access to health information. (Source: HealthIT.gov)
I will state this plainly. This means that, soon, whether folks like it or not, patients will directly be able to access their medical record en toto without an intermediary office or provider. Pathology reports and other diagnostic materials are not exempt from this. Within the next few months, more hospital systems will implement direct access and release protocols for patients who will now be able to directly read their pathology reports without their primary care physician or specialist’s filter.
Some of you reading are rejoicing and thrilled. Others may be projecting harsh words this way if I’m the first time you’ve seen this. To the former group: If you were a part of the last ASCP Annual Meeting, I was fortunate to be a part of a panel with Dr. Jeffrey Meyers discussing the role “Patient-Facing-Pathology” where he talked about practical applications of involving patients in our work. I discussed concepts like “Pathology Explanation Clinics” and other reimbursable potential encounters we in pathology might soon be involved in. The idea of bringing pathology out of the basement, out from behind the curtain, and in the forefront of the patient healthcare experience has become a large part of our professional discourse for the past few decades—and the Cures Act is an exciting potential catalyst.
Image 2. Excuse the stock-photo watermark, but if you’re expecting encounters like these. Well…you’re half right. (Source Cartoonstock.com)
To the latter group: don’t panic. It’s going to be fine. You’re (probably) not going to get a 03:00 am call from an anxious patient expressing confused consternation over your frozen section report of “low grade oncocytic malignancy” or “defer to permanent…” Well, at least for now. Most programs are implementing a sort of “proofreading delay” before reports are actually released, with enough time to compile addendum reports and amended notes, etc. Even still, the notion that we may be implicated in a tsunami of impending requisite patient demands is indeed daunting.
I’ve spoken to several colleagues inside and outside my department who can’t seem to come to a consensus (very specific joke there) about the nature of how the Cures Act will change our work. Dr. Imran Uraizee, a surgical pathology fellow with me here at Loyola who’s written on here before, shared much of the same sentiment. The double edged sword. The initial hesitation. The problematic “translatability” and readability of our material. The potential benefits… It led to a great discussion, and ultimately, with comparisons to HIPAA rollouts and other large-scale changes in our healthcare delivery, we agreed that there are going to be growing pains. But growing is good right?
And you’re right! Why should we have to add more responsibilities onto our overcrowded plates? We’ve all just accepted the reality of advancing technologies time and time again, adding infinite immunohistochemical capabilities to our testing/send out menus, incorporating as much molecular testing as our department funds can accommodate, and (some of you) painfully tolerating the advent of digital microscopy and—if I may—artificial intelligent software tools. That’s already so much that has changed our landscape. While we figure out ways to get out of the basement so we can finally have windows, why should we change the way we file and release our reports? Or should we? Will we be directly answering the phone calls of exceptionally-involved-in-their-care patients without some kind or reimbursable encounter? Will residents? Think of our administrative support and ancillary staff—we may not have enough phones. When you add more, you expect some burden to shift. This will undoubtedly tax someone’s productivity; we just haven’t figured out who, what, where, or how yet.
But let’s go back to the positives… This is, in fact, a double-edged sword. And while, on the one hand, we might worry over the implications of diving in too deep, this really has potential to advance our profession in such a positive way. First of all, patients’ direct access to pathology reports may do us all a favor an slowly increase the medical literacy challenges we face today. Let’s be honest, pathology reports are not user-friendly and, as much as we may like to admit that our autopsy reports are written so that decedents’ families may find solace or comfort, we’re not writing for them directly. Behind our medico-legalese, our coded clinical content, and high-expert level commentary that far supersedes the standard 7th grade reading level, are decades of evolution in a field of medicine that has catered to fellow clinicians over patients. We write for heralded concepts in high-reliability and high output departments that demand precision, accuracy, and volume. To some, this may have contributed to some of the medical mistrust we face in this country and with increased transparency and open doors, we may even reduce the litigious nature of the patient-physician dynamic. And hey! If we can actually charge for these encounters like our clinical compatriots—which we have the potential too, by the way—then why not? The average CPT reimbursement in 2018 was $75 for a 15 minute encounter. Let’s say a full day of meeting patients includes four of these consults per hour. That’s about $300 per hour, $2,400 per full work day; with a faculty of about 20-30, just a handful doing consults for a day would be nearly $10,000. I can do more math. So could you. But hey we just bought new state-of-the-art IHC stainers and a boatload of shiny clinical analyzers with matching middleware support. Let’s not look a gift horse in the mouth? Wishful budgets aside, I don’t have any definitive answers for you—I know, I usually do, I’m sorry. But if the last two years have taught me anything, it’s that we can’t know what we don’t know unless we figure out what we do know.
We know we’ve been wanting to get out from the “paraffin curtain” for quite some time.
We know we’ve wanted to play a larger part in clinical patient care for decades.
We know we’ve got excellent professionals and experts in every nook and cranny this blog finds readers.
Well… careful what you wish for.
Is the Cures Act a cure all? Probably not. But maybe this is a chance for us to have some positive growth within our profession and an opportunity to connect with patients and simply make healthcare at-large better.
What do you think? Contact me on social media, leave a comment below, or share this piece with your colleagues to spark some conversations in your department.
Thanks for reading, see you next time!
–Constantine E. Kanakis MD, MSc, MLS(ASCP)CM is a first-year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. He is a certified CAP inspector, holds an ASCP LMU certificate, and xxx. He was named on the 2017 ASCP Forty Under 40 list, The Pathologist magazine’s 2020 Power List and serves on ASCP’s Commission for Continuing Professional Development, Social Media Committee, and Patient Champions Advisory Board. He was featured in several online forums during the peak of the COVID pandemic discussing laboratory-related testing considerations, delivered a TEDx talk called “Unrecognizable Medicine,” and sits on the Auxiliary Board of the American Red Cross in Illinois. Dr. Kanakis is active on social media; follow him at @CEKanakisMD.
Since my last post on the B.1.1.7 (UK) variant, several other variants have arisen. I wanted to describe what makes some Variants of Interest and other Variants of Concern. While a “variant” is often synonymous with a mutation in genetic terms, in the context of SARS-CoV-2, variant means an alternative strain of the virus.
To become a Variant of Interest (VOI), the World Health Organization (WHO) or Centers for Disease Control (CDC) has the following characteristics:
Evidence of variants that affect transmission, resistance to vaccines/ therapeutics, mortality, or diagnostic tests
Evidence that the variants is contributing to a rise in the proportion of cases in an area.
However, limited geographical spread.
Examples: P.2 (from Brazil) B.1.525 (New York), and B.1.526 (New York).
Variants of Concern have increased problems with the same characteristics listed above:
Evidence of reduced vaccine protection from severe disease
Evidence of substantially reduced response to neutralizing antibodies or therapeutics
Evidence of widespread spread
Increased Transmissibility or disease severity
Current VOCs: B.1.1.7 (UK), B.1.351 (South Africa), P.1 (Brazil), and B.1.427/ B.1.429 (California).
The initial VOC of B.1.1.7, B.1.351 and P.1 were identified from having increased spread and more mutations than expected, especially in the Spike gene region (Figure 1).
The N501Y mutation in the Spike protein is present in each VOC. It is located at the tip of the protein that binds the ACE2 receptor, increasing binding strength.
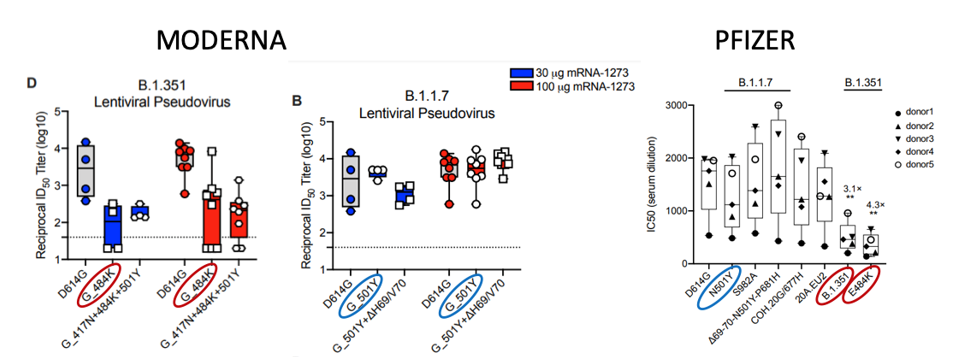
So far, vaccines react against the B.1.1.7 variant. However, B.1.351 pseudovirus shows decreased neutralization by both Moderna and Pfizer sera. Specifically, the E484K mutation in the Spike protein confers resistance to neutralizing antibodies. Thus, the strains B.1.351 and P.1 are more likely to be resistant as would any other strain with the E484K variant.
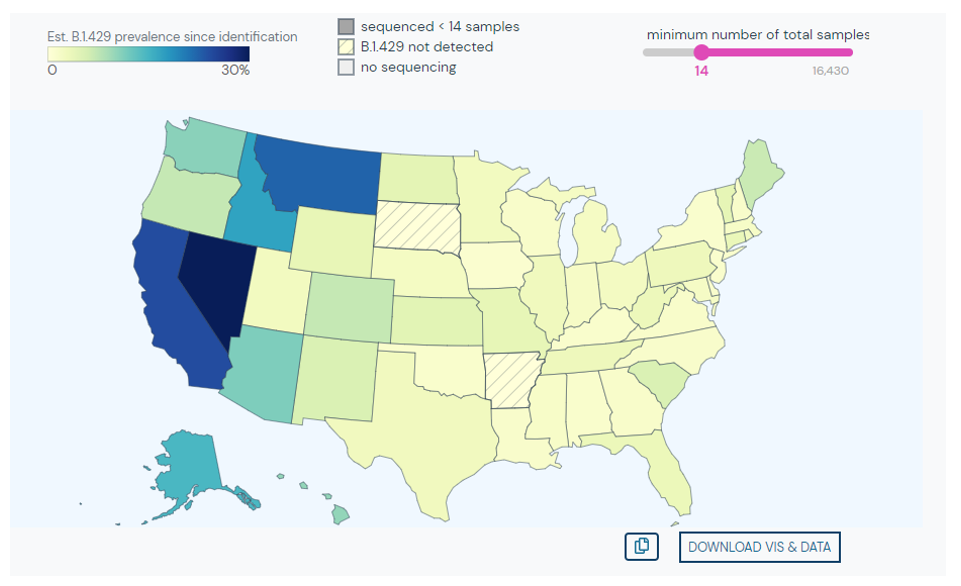
Lastly, the California variant arose as it was found to rise in prevalence from November to February. The key mutations include W152C and L452R, but the significance of this variant is uncertain. However, this variant has begun to spread over much of Southern California and Nevada.
References
Wu K, Werner AP, Moliva JI, Koch M, Choi A, Stewart-Jones GBE, Bennett H, Boyoglu-Barnum S, Shi W, Graham BS, Carfi A, Corbett KS, Seder RA, Edwards DK. mRNA-1273 vaccine induces neutralizing antibodies against spike mutants from global SARS-CoV-2 variants. bioRxiv [Preprint]. 2021 Jan 25:2021.01.25.427948. doi: 10.1101/2021.01.25.427948. PMID: 33501442; PMCID: PMC7836112.
Tada T, Dcosta BM, Samanovic-Golden M, et al. Neutralization of viruses with European, South African, and United States SARS-CoV-2 variant spike proteins by convalescent sera and BNT162b2 mRNA vaccine-elicited antibodies. Preprint. bioRxiv. 2021;2021.02.05.430003. Published 2021 Feb 7. doi:10.1101/2021.02.05.430003
Gangavarapu, Karthik; Alkuzweny, Manar; Cano, Marco; Haag, Emily; Latif, Alaa Abdel; Mullen, Julia L.; Rush, Benjamin; Tsueng, Ginger; Zhou, Jerry; Andersen, Kristian G.; Wu, Chunlei; Su, Andrew I.; Hughes, Laura D. outbreak.info. Available online: https://outbreak.info/ (2020)
–Jeff SoRelle, MD is Assistant Instructor of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX working in the Next Generation Sequencing lab. His clinical research interests include understanding how lab medicine impacts transgender healthcare and improving genetic variant interpretation.Follow him on Twitter @Jeff_SoRelle.
I quickly transitioned from from learning at Jefferson to teaching at Jefferson less than 6 months after I graduated from the Cytotechnology program. Assuming this new role of teaching future cytotechnologists was a refreshing twist after continuously learning at work. I stood at the podium as an alumna in my previous classroom with a breadth of fresh material to work with, appreciate, and share. At the beginning of each lecture, I would check in on my students, ask them how their other classes were going, ask if they had any questions, and then, I would share an interesting case from my work week thus far. Aside from the weekly lecture on ancillary techniques, such as molecular and immuno-diagnostics, I assigned multiple activities such as journal club/conferences, discussions, and my personal favorite – a mock tumor board. Each student would take turns playing the role of the physician, radiologist, cytotechnologist, pathologist, and oncologist (surgical, medical, or radiation). For my first year of instruction, I had assigned the group their “tumor” of interest, but I quickly encouraged their creativity run rampant during subsequent years.
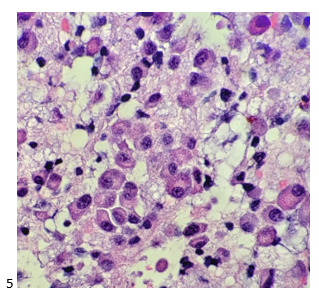
Despite working in a cancer center and being able to recognize some fairly obscure tumors with little experience, I did not realize how much I still had to learn, even as a part-time lecturer and full-time cytotechnologist. These tumor boards taught me so much more than I expected, and I am forever thankful for the experience of having such wonderfully bright students teach ME! For one very memorable tumor board, the students elected to present the diagnosis and treatment of a male patient with multiple myeloma. Yes, plasma cells! Plasma cell neoplasm, plasmacytoma, multiple myeloma. Awesome, let’s see what this group can do! The “physician” said the patient complained of widespread bone pain, malaise, and recurrent fevers and infections. The “radiologist” presented the images of osteolytic lesions throughout the skull and vertebrae, the latter of which core biopsies and FNAs were obtained. The “cytotechnologist” described a mix of plasmablastic cells, as well as mature and immature plasma cells, some with clock face chromatin and a perinuclear hof (which is my telltale feature that I now emphatically describe to everyone else). The “pathologist” bypassed flow cytometry and performed Kappa/Lambda light chain immunohistochemistry on the core biopsy, diagnosing the patient with multiple myeloma. Unfortunately, due to the extent of the patient’s disease, the “oncologist” and her team could not increase the life expectancy, and the student’s patient expired.
Now, whenever I have a plasma cell neoplasm or multiple myeloma case, I think back to my students and their mock tumor board and everything they taught me. I just recently attended an FNA on a 79-year-old male with a history of multiple myeloma who presented with a PET positive right facial mass and right cervical lymph nodes. The radiologist performed an ultrasound-guided FNA of a right peri-mandibular soft tissue mass, and it took everything in me to not tell the radiologist anything more than “adequate.” But when I saw those perinuclear hofs, I was elated to have a definitive diagnosis!
Later that afternoon, I couldn’t wait to screen my pap-stained slides. The clock face chromatin was so beautiful! My cell block the following morning highlighted the textbook perfect features diagnostic of a plasma cell neoplasm.
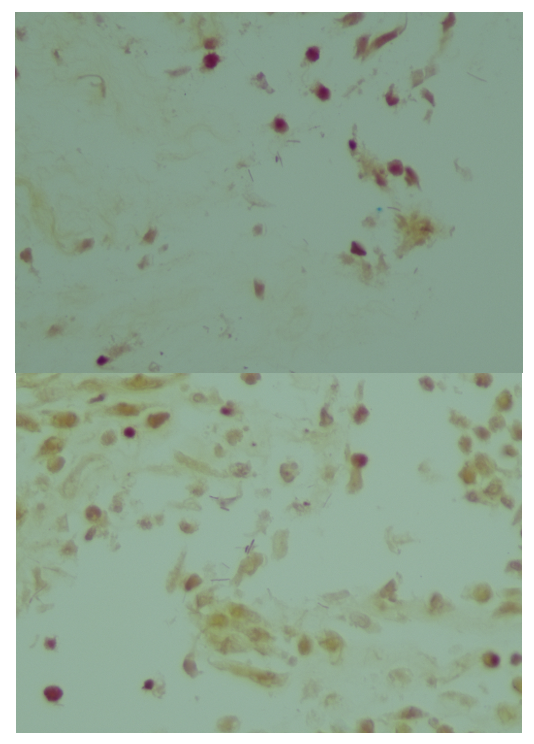
The attending pathologist ordered a routine myeloma immunocytochemistry panel, including CD138, kappa light chain, lambda light chain, CD20, CD45, and MUM1.
Immunocytochemical stains performed on the unstained paraffin sections showed the tumor to be positive for CD138, kappa light chain, and MUM1, focal equivocal staining for CD20, and negative staining for lambda and CD45. The case was signed out as a plasma cell neoplasm.
The bone marrow core biopsy was sent for Cytogenetic Microarray Analysis and Next Generation Sequencing. The CMA results revealed gains of chromosomes 3, 5, 9, 11, 15, 19, and 21 and losses of chromosome segments 1p and 2p and 7 p in mixed states. Loss of 1p is associated with a poorer prognosis for multiple myeloma. Next gen sequencing identified a tumor mutation burden of 8.4Muts/Mb with mutations detected in the following genes: FAM46C, BRAF, KAT6A, TSC1, KRAS, FLT3, and NFKBIA.
-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
A 14 year old female arrived at the emergency room with her mother and grandmother complaining of extremely heavy menstrual bleeding. Patient history reported by her mother included a history of “a bleeding problem” for which she had been treated a few times since age 4. Petechiae were noted on the girl’s abdomen, arms and thighs. There was no history of aspirin or other NSAID use. Blood work was ordered.
Patient results are shown in Table 1 below.
The mother called home to ask her husband for details and reported that her daughter had been diagnosed with Immune Thrombocytopenic Purpura (ITP) 10 years earlier but was not very clear on the treatments. She stated that other than frequent nose bleeds, some petechiae, and occasional bruising that the girl had seemed ok until she started menstruating. They had not seen the specialists in a number of years. Further questioning of the mother revealed that the parents had both immigrated from Iran with their families as infants. The patient was an only child. The grandmother reminisced about the village “in the old country” and mentioned that her daughter and son in law were related, the families being from the same village. When asked about any other family with bleeding disorders, the mother reported that neither she nor her husband had ever met any other relatives in Iran and were unaware of any bleeding tendencies in the family. The grandmother interjected that she did remember that several of her cousins and an uncle experienced frequent epistaxis.
The ER physician noted the normal PT/INR, APTT and slightly decreased platelet count but felt the extensive petechiae and hypermenorrhagia were out of proportion to these results. A manual differential was ordered. Differential results were within normal ranges, RBC morphology reported sight polychromasia and anisocytosis. Platelet estimate was slightly decreased with giant platelets noted. The physician suspected an inherited platelet disorder and the patient was referred to a hematologist for further workup.
I have written a few blogs about different thrombocytopenias. This case interested me because the patient was first diagnosed with ITP. ITP is an autoimmune bleeding disorder in which the immune system makes anti-platelet antibodies which bind to platelets and cause destruction. Even though the exact cause of ITP remains unknown, it is recognized that it can follow a viral infection or live vaccinations. In children this tends to be an acute disease which is self-limiting and self resolves in several weeks. However, in a small number of children, ITP may progress to a chronic ITP, as was thought to be the case in this patient.
A new hematologist saw the patient and reviewed the medical history. In this patient, the diagnosis of ITP had been followed for a short period of time in which the platelet count did not increase. She was treated with immunoglobulin. When her platelet count dropped below 30 x 103/μL, the patient was transfused several times. Early platelet transfusions increased her counts, but the patient became refractory and was then given HLA matched platelets, with some improvement. After a period of time, the patient did not return to the specialist and the parents described her condition as improved. However, as reported to the ER physician, she still experienced frequent epistaxis and other bleeding symptoms unrelated to accidental injury. The mild thrombocytopenia and giant platelets on the blood smear with normal PT and APTT in a patient with abnormal bruising or bleeding alerted the physician to the possibility of the diagnosis of Bernard Soulier Syndrome (BSS). The family history also suggested BSS.
The hematologist ordered further testing. Noted in the patients chart from 10 years ago was a prolonged bleeding time. This test was not repeated at this time because it has largely been replaced by platelet function analyzers (PFAs.) The PFA test analyzes platelet function by aspirating citrated blood through membranes to induce platelet adhesion and platelet plug formation. The test is first performed with a collogen and epinephrine membrane (Col/Epi). If the closure time is normal, platelet function can be considered normal. If the closure time with Col/Epi is increased, then the test is repeated with a collogen and ADP membrane (Col/ADP). A prolonged closure time with Col/Epi with normal Col/ADP closure time may indicate an aspirin induced platelet disorder, whereas an increased closure time with both membranes may indicate a platelet defect that is not aspirin related.3 The PFA closure times were increased in both the Epinephrine and ADP cartridges.
Platelet aggregation was normal with all agents except ristocetin. BSS can be differentiated from von Willebrand disease(vWD) by the addition of normal plasma to the ristocetin agglutination test. The addition of normal plasma adds vWF to the suspension, and in vWD the ristocetin agglutination is corrected. Agglutination with ristocetin requires vWF and GPIb/IX. Since GPIb/IX is absent or reduced in BSS, he ristocetin agglutination is not corrected in BSS, as seen in this patient.3 Flow cytometric analysis of platelet glycoproteins demonstrated reductions in CD42a (GpIX) and CD42b (Gp1bα).
Bernard Soulier syndrome (BSS), also known as Hemorrhagiparous thrombocytic dystrophy, was first described in 1948 as a bleeding disorder characterized by a prolonged bleeding time and giant platelets seen on a peripheral smear. It is an inherited platelet adhesion disorder caused by platelet glycoprotein (GP) deficiencies. The disorder is rare, affecting only about 1 in 1,000,000, though it is more common in families where parents are related. BSS is typically autosomal recessive, though a small number of cases have been found that are autosomal dominant. Most cases are diagnosed at a young age, with the autosomal dominant type often less severe and diagnosed later in life.1
Platelets are involved in primary hemostasis, the initial arrest of bleeding that occurs with vascular injury. As we know, platelets’ functions include adhesion and aggregation. Platelets first stick to the blood vessel wall (adhesion), followed by binding to each other (aggregation). In primary hemostasis, platelets first adhere to von Willebrand factor (vWF) which is bound to the subendothelial collogen fibers. This is followed by aggregation, a complex process that results in the formation of the platelet plug and the initial arrest of bleeding.. In BSS, platelet membrane GPs Ib, V and IX are missing, resulting from an inherited mutation in one of the genes that code for proteins in the complex. This affects the binding of the platelets to vWF, which subsequently interferes with primary hemostatic plug formation.4 If the platelets don’t adhere, aggregation is also affected.
Patient Results
In order to make a differential diagnosis of platelet function disorders, laboratory testing is necessary:
Tests of secondary hemostasis, PT and APTT, are normal in this patient so a disorder of primary hemostasis would be suspected.
In this patient, the platelet count was slightly decreased. In BSS, the platelet count is variable, from normal is moderately decreased, and can vary from time to time in the same patient.
Platelet adhesion tests (PFA) performed with both Col/Epi and Col/ADP were abnormal.
Light transmission aggregometry revealed platelet aggregation was normal with ADP, collogen and epinephrine. Aggregation with ristocetin was abnormal.
Giant platelets observed on peripheral smear
Flow cytometric analysis of platelet glycoproteins demonstrated reductions in CD42a (GpIX) and CD42b (Gp1bα).
Diagnosis: Bernard Soulier syndrome.
Conclusion
BSS is rare and is commonly mistaken for ITP. Reports have been published that analyze cases of BSS patients long treated as ITP. These misdiagnosed cases have been treated with immunoglobulins, steroids, IV anti-D, and other drugs used to treat refractory ITP. Splenectomies have even been reported in some cases. Platelet aggregation to ristocetin and flow cytometry have provided the correct diagnoses. Molecular studies can also be done to identify the abnormal genotype.2 Clues that can lead to a correct diagnosis are childhood ITP that does not spontaneously resolve and does not respond to treatments, other family members with bleeding problems or low platelet counts, platelet counts that are not low enough to explain bleeding or prolonged bleeding times, increased MPV and the presence of giant platelets on the peripheral smear.
This patient was diagnosed with ITP as a child, but treatments did not improve her platelets counts. She continued to have bleeding episodes which increased with the onset of menses. Her grandmother reports a history of bleeding tendencies in other family members. In addition, her parents are related. Her peripheral smears noted giant platelets. Laboratory tests confirmed a diagnosis of BSS.
Bernard Soulier syndrome (BSS) is a rare but important long-term bleeding disorder.
Patients do not require routine prophylactic treatment, so the management of BSS focuses on prophylactic treatment before certain procedures or after injuries. Patients should be advised not to take NSAIDS. The patient should be advised that treatment may be necessary prior to procedures or in response to common bleeding events such as bleeding gums, epistaxis, and menorrhagia. Antifibrinolytic therapy can be used in bleeding episodes. Platelet transfusions are considered for patients before surgery or if anti-fibrinolytics have failed. For severe cases, stem cell transplants have provided a cure. BSS may also be a candidate disorder for gene therapy in the future.1
References
Grainger JD, Thachil J, Will AM. How we treat the platelet glycoprotein defects; Glanzmann thrombasthenia and Bernard Soulier syndrome in children and adults. Br J Haematol. 2018 Sep;182(5):621-632. doi: 10.1111/bjh.15409. Epub 2018 Aug 17. PMID: 30117143.
Reisi N. Bernard-Soulier syndrome or idiopathic thrombocytopenic purpura: A case series. Caspian J Intern Med. 2020;11(1):105-109. doi:10.22088/cjim.11.1.105
Turgeon, Mary Louise. Clinical Hematology, Theory and Procedures. Fifth ed. 2012. Lippincott Williams and Wilkens. Baltimore.
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A 38 year old female with history of endometriosis presented to emergency department complaining of heavy vaginal bleeding for 2 weeks duration. She also reported recent diarrhea, abdominal pain, nausea, fatigue, shortness of breath, fever, and chills. On physical exam, the patient had fever, tachycardia, tachypnea, and abdominal distention with a large, 32-week size uterine mass. She was found to have microcytic anemia (Hgb 9.2 g/dL, MCV 77.1 pg), diabetic ketoacidosis (glucose 522 mg/dL, ketones and glucose in urine, A1c 9.1%), and based on the above vital signs and leukocytosis (WBC 31.75/L)met sepsis criteria.
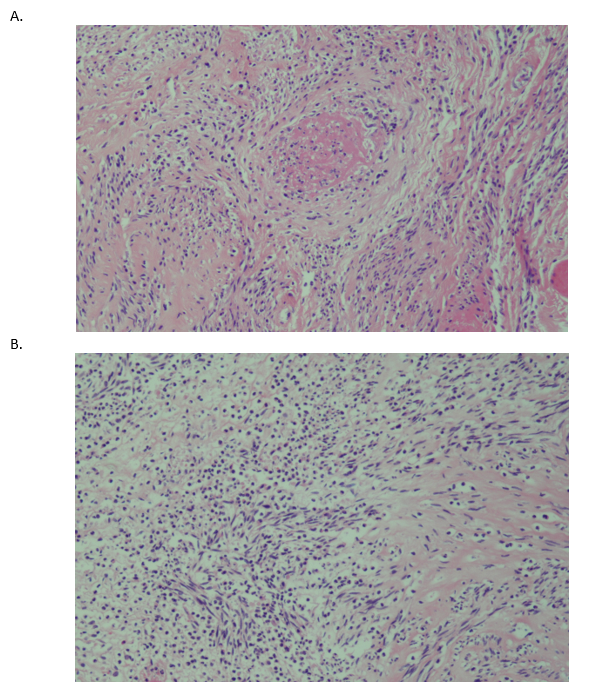
Abdominal CT revealed multiple uterine leiomyomas (fibroids), with the largest measuring up to 13.2 cm and demonstrating characteristics concerning for pyomyoma (abscess arising in leiomyoma). The patient underwent exploratory laparotomy and myomectomy. Gross images of the resected uterine mass demonstrated a circumscribed whorled nodular lesion with patchy necrosis (Image 1). Histologic examination of the resected lesion demonstrated a bland smooth muscle tumor, devoid of cytologic atypia and mitotic activity, with area of abscess formation showing necrosis and abundant neutrophils leading to a diagnosis of “Leiomyoma with severe acute inflammation, areas of necrosis and abscess formation, consistent with pyomyoma (14 cm)” (Image 2). A tissue Gram stain demonstrates multiple morphotypes of bacteria (image 3). Blood cultures, drawn on admission, flagged positive and the Gram stain revealed gram negative rods and blood, chocolate and Maconkey agars grew creamy gray non-hemolytic colonies that did not ferment lactose. MALDI-TOF mass spectrometry was performed and identified the isolate as Salmonella species. A triple sugar iron agar slant was set up to confirm the phenotype of a non-typhoidal serovar of Salmonella. Growth of the organism demonstrated abundant hydrogen sulfide production, an acidic butt, and an alkaline slant, confirming the nontyphoidal phenotype.
Image 1. Gross image of the resected leiomyoma (fibroid). Formalin fixed, serially sectioned, encapsulated smooth muscle mass with patchy areas of abscess formation and necrosis. Mass measures 14 cm in greatest dimension.Image 2. Histopathologic micrograph of hematoxylin and eosin stained leiomyoma (10x objective). A) shows spindle-shaped smooth muscle cells with admixed neutrophils. Central area of necrosis with abscess formation. B) shows edematous and necrotic smooth muscle with intermixed acute inflammation.Image 3. Tissue Gram stain showing multiple morphotypes of bacilli with poorly staining gram characteristics (40x objective).
Discussion
Pyomyoma, also referred to as suppurative leiomyoma, is an exceedingly rare complication of uterine leiomyoma, which involves infarction of the benign tumor followed by introduction and growth of bacteria.1 Microbes can be introduced by way of ascending genitourinary infection, spread from adjacent structures, or hematogenous or lymphatic spread.2 These infections may be polymicrobial or caused by a single microorganism, and the reported causative agents vary widely, with the most common being Escherichia coli, Staphylococcus species, streptococcal species, enterococcal species, Bacterioides species, Clostridium perfringens, and Candida.3 However, there have been no reported cases of Salmonella species isolated from pyomyoma to date.
Salmonella is a gram negative bacillus belonging to the Enterobacteriacae family.4,5Salmonella enterica, the species responsible for causing disease in humans, is sub-divided into numerous serovars, which can be broadly grouped into typhoid and nontyphoid.4,5 While the typhoid serovars cause enteric fever, the nontyphoid serovars can cause gastroenteritis and bacteremia.5 Most nontyphoid Salmonella infections are foodborne, and approximately 5% of nontyphoid Salmonella infections progress to bacteremia.4 The bacteria gain access to the bloodstream by utilizing multiple virulence factors to invade the epithelial cells of the gut.4Salmonella can be identified in the laboratory from blood culture based on several characteristic biochemical results, including Gram stain, absence of lactose fermentation, motility, hydrogen sulfide and gas production, utilization of citrate, and decarboxylation of lysine and ornithine.
This case presents Salmonella species as the cause of sepsis in the setting of pyomyoma, a very rare entity. It is postulated that gastroenteritis caused by nontyphoid Salmonella may have been the cause of the patient’s recent diarrhea, and uncontrolled blood glucose levels in the setting of diabetes may have contributed to the progression to sepsis. We could hypothesize whether the Salmonella seeded the fibroid precipitating the abscess formation since Salmonella is known to cause abscess formation in unusual sites including having a proclivity for vascular sites (e.g., aortitis). The patient unfortunately experienced complications from her sepsis with concomitant surgery. She became unresponsive despite numerous attempts at resuscitation and died.
References
Azimi-Ghomi O and Gradon J. Pyomyoma: Case Report and Comprehensive Literature Review of 75 Cases Since 1945. 2017. SM Journal of Case Reports. 3(4):1054.
Obele, CC, et al. A Case of Pyomyoma following Uterine Fibroid Embolization and a Review of the Literature. 2016. Case Reports in Obstetrics and Gynecology. 2016:9835412.
Iwahashi N, et al. Large Uterine Pyomyoma in a Perimenopausal Female: A Case Report and Review of 50 Reported Cases in the Literature. 2016. Molecular and Clinical Oncology. 5(5):527-531.
Eng SK, et al. Salmonella: A Review on Pathogenesis, Epidemiology, and Antibiotic Resistance. 2014. Frontiers in Life Science. 8(3):284-293.
Coburn B, et al. Salmonella, the Host and Disease: A Brief Review. 2006. Immunology & Cell Biology. 85(2):112-118.
-Heather Jones is a first year AP/CP resident at UT Southwestern.
-Katja Gwin is an Assistant Professor at UT Southwestern in the Department of Pathology and specializes in gynecologic pathology.
-Dominick Cavuoti is a Professor at UT Southwestern in the Department of Pathology and specializes in cytopathology, infectious disease pathology and medical microbiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
I have been through physical therapy for a few different issues in my life, and I must say (with apologies to the profession), I was never a believer. I had musculoskeletal issues that needed attending—a pinched nerve, neck pain, knee pain, etc. If you are past 40 years old and your body’s check engine light has blinked a few times, you know what I mean. Each time the series of physical therapy exercises seemed to be useless and a waste of time. They never really helped me. Recently, however, I subjected myself to a total knee replacement surgery. I knew PT would be a part of the recovery regimen, but I did not realize how important it was going to be for my overall recovery. Therapists taught me how to walk again, they taught me how to trust my body and that I could do things I did not believe possible until that next session. They caused pain (a necessary part of the journey), and they did all of these things with care and professionalism- despite my whining and sometimes less than positive attitude. For me, this is where the PT rubber hits the road. This is where the profession shines and has the successes that people talk about. I saw the real face of physical therapy, and I became a believer.
Then I began to wonder, what is that moment of shining for lab safety professionals? When do laboratorians become believers in lab safety? When does the safety rubber hit the road? What is that sweet spot that makes safety important to people?
I had a needle stick exposure early on in my career. It was before the advent of needle safety devices, and I picked up a used butterfly needle off of a bed and stuck myself in the finger. I was in a hurry, and not really paying attention. That event made me a much safer needle-handling phlebotomist- but would proper safety training have done the same? Would my risk tolerance have been different if someone had really explained the potential consequences of an exposure to me? Did the rubber hit the road for me because I had that experience? How does that get moved or changed so that safety behaviors become proactive instead?
I have hypothesized often that people will perform safely based on three motivators: knowledge about consequences, information about financial and environmental impacts, and punishment. Personal risk tolerance also plays a role, however. A technologist may be full well aware that an open specimen may splash, but they may also feel that the risk is low or that the result of a splash incident would not be severe, so they don’t use face protection. Sometimes, though, we make mistakes when deciding upon the risks, especially if we do not have sufficient education. Any open specimen is a potential exposure hazard, and all specimens should be treated as though hazardous.
In order for a lab safety program to have success, the working parts must be proactive. They must be in place to prevent injuries and exposures, and they should not be there only to figure out what to do after an event has occurred. When a program works in that proactive fashion, when staff is on board and participating, that’s when safety shines. That’s the safety sweet spot.
I’m thankful for professions that easily get it right- like physical therapy. People might not always see their value until they really need them, and that is when they shine. So maybe that’s true for lab safety – it shines when it is really needed. For lab safety professionals, then, the next step will be to get laboratorians to see that we need safety all the time.
A special thank you to Stephen, Audra, and the entire PT gang! You guys rock!
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
In this last part of our four-part series on pathology value chain, where we are using the patient’s best outcome as the maximized value, we examine two areas: Marketing/Sales and Service. The former has inherent challenges, some of which were mentioned in the last blog on outbound logistics. The latter is becoming an increasingly important component of oncology care for which many pathology labs are grasping for solutions.
In traditional business budgeting, the first step is for the marketing and sales department of a firm to provide a projection of revenue for a given period based on their knowledge of trends, markets, prior years, competition, competitive advantage, etc. These projections are then paired with costing exercises to shoot for a margin of profit. If we are going to sell $1,000,000 in widgets and it costs us $750,000 in total to make those widgets available to our customers (including costs of goods sold, administrative expense, taxes, and interest), we would have a $250,000 profit to use as retained equity or to distribute to our shareholders. When we look at pathology services for cancer, a new laboratory with no prior history may find this process extremely challenging without an enormous amount of data. An existing laboratory with many years of work may have a much easier time and, short of drastic changes in supply prices, inflation, and taxes, could likely use a simple percentage growth approach for this calculation.
But unlike widgets or iPhones or Quarter Pounders or golf clubs, no one wants to have a tissue biopsy and certainly no one wants to have suspected cancer. If we turn to epidemiological data, we can predict (and do so below) the expected number of patients in a given population to likely have cancer in the coming year (although this is clearly not the only data point we need). For a new laboratory in a place where there are no other laboratories (e.g., a small low- to middle-income country with a new Ministry of Health mandate to fight cancer), such an estimate is important for determining both if we should even have a lab (or use a regional approach) and, if we do have a lab, what our maximum volume would be assuming 100% access. The former part has been addressed previously such that there is a threshold below which is difficult to justify a lab because of the cost per sample. The latter part, however, is crucial because a “marketing campaign” (i.e., patient education and clinician education about cancer, how to diagnosis it, and how labs are part of this process) is the only way to have any volume in this laboratory.
We would except it to start slow and build but we have a finite endpoint for cancer cases in mind. But note, importantly, that the marketing campaign described has nothing to do with the pathology laboratory itself. In an existing, highly-developed market (e.g., Boston, London, Montreal, Sydney), there is a population that we can assume represents our cancer risk pool but there are also many competing laboratories (and health systems), transient use of services (e.g., Ms. Smith from Iowa decides to go to Boston for cancer care), and levels of care (i.e., low-stage cancer care in a community setting versus later-stage cancer with comorbidities in a tertiary care setting). None of these things can a given pathology laboratory control if they are in that market, but must they use all of this information to understand the projected revenue and create their budget? Or can they just assume a percentage increase? From the patient perspective, all of this is irrelevant because patients most commonly do not choose the pathology laboratory that is going to see their biopsy as it is a function of the health system to which they subscribe for their care. In that context, marketing and sales for cancer diagnostic services is largely a negotiation between laboratories and clients (e.g., clinicians, hospitals, health plans) which is often contractual. Such contracts are difficult to negotiate, take a long time, and usually last for an extended period like 1 year or longer. This very concept is contrary to the activities of the marketing and sales department which must constantly pivot, update, and change their strategy to achieve their projected revenue. It is worth noting that in many poorly developed cancer systems, patients do directly take their samples to pathology laboratories of their choice and examples of systems with kick backs to shift these samples away from government laboratories toward private practice facilities (at a much higher cost to patients) are well documented.
In the Value Chain model, service is the after-market activities of a firm to maintain their product(s) for a customer, create customer loyalty and resales, and enhance their competitive advantage through maximized firm-customer relationships. The popularity of subscription services (e.g., Amazon Prime, Netflix, Massage Envy, car leasing) stems from the increased opportunity to interact with customers continuously in low-cost ways that enhance the customer’s experience with the firm. Although a service like rending a definitive pathological diagnosis may appear to be a one-time event, recent evolution in the practice of oncology and increasing research needs have created unique servicing opportunities for pathology laboratories. The emergence of biomarkers that dictate treatment unrelated to the diagnostic process has created gaps in quality due to inefficient systems, entry cost barriers, volume challenges, and intellectual disconnect from the traditional diagnostic process. However, streamlining the biomarker process, for example, can create a competitive advantage for a laboratory and improve client loyalty and rapport.
Marketing and Sales
This activity focuses on “strategies to enhance visibility and target appropriate customers.” This activity in diagnostic anatomic pathology specifically for cancer speaks to the first part of the value chain for the patient; namely, the timely presentation of a patient to the clinical system for evaluation of cancer at the earliest possible time. As such, whether a patient presents incredibly early or very late makes no difference to the pathology laboratory because the customer choosing the pathology service is either an independent clinician or a health system. Private practice pathologists may advertise or market to community hospitals or hospital systems in hopes of capturing their volume (and revenue). Marketing for second opinion review by a pathologist can also occur and may be directly to patients. This activity is challenged from the beginning, however, due to the small market. For every 1,000,000 patients in the United States, there are about 5500 cancers per year. Assuming the accuracy of a clinical decision to obtain a biopsy is around 50% (i.e., the “malignancy rate” – when a clinician decides a biopsy is needed for suspected tumor, 50% of the time it is cancer and 50% of the time it is not), that’s 11,000 suspected cancer biopsies per million per year. Extrapolating to the US population, we get 3.6 million biopsies per year. Given that there are ~10,000 anatomic pathologists, that equates to, on average, 361 biopsies per year per pathologist (or, roughly 1 per day). Since most pathologists could easily sign out 20 cases every other day working Monday – Friday with 4 weeks of vacation annually, that’s a ratio of 1:8 (average:capacity).
The point of all of this math is that the volume of pathology work in the US that is for cancer is small relative to the total biopsies performed (or capable of being performed) by the pathology community and, thus, the market for cancer diagnostic services appears saturated. We can adjust the dial of this to take the malignancy rate to 5% (i.e., massive over biopsy setting), and find that pathology would be overwhelmed at 130% capacity just for suspected cancers; however, as we move back towards 50% malignancy rate, the average capacity is around 25% for volume. If we move on the other side of 50% towards lower biopsy rates or “improved clinical acumen,” capacity quickly drops to below 9% with a great excess of pathologists. With the promise of artificial intelligence to assist pathologists in faster sign out of higher volumes, the capacity for cancer diagnosis increases possibly 10-fold. But if you ask your average pathologist if they are busy, they report that they are. This is because the pathology laboratory, as all laboratorians are aware, processes more than just suspected cancer biopsies. Medical kidney, medical dermatology, screening colonoscopy, colposcopy, breast core needles, melanotic and non-melanotic skin lesions create a huge portion of the volume that is not part of the specific calculation above that adds many millions more samples per year to the pathology revenue stream. One framing of this case pool is that cancer biopsies, because they aren’t technically elective, are cross subsidized by providing all of the other services which are equally billable. However, this large bulk of cases are still not through direct marketing to the patient but rather to providers or health systems.
As we turn this activity towards LMICs, we instantly have a problem. There is no system in most places to support routine services for medical kidney, medical dermatology, screening colonoscopy, colposcopy, breast core needles, melanotic and non-melanotic skin lesions (especially in Black patient populations for the last). Without the cross-subsidization that these billable biopsies bring in, pathology laboratories are left with the low volumes of suspected cancer cases. As mentioned above, these laboratories are often overwhelmed to begin with so the marketing and sales activity, which would theoretically increase volume, is likely not to be a priority. In these settings, however, what will increase volume and improve the quality of care for patients is large pre-analytical efforts by governments and other entities to educate the public and the general practitioner about cancer screening and diagnosis, community awareness about cancer care systems, specimen transport networks from the most rural directly to pathology laboratories, and government spending on prevention of cancer.
Service
This last set of activities are to “maintain products and enhance consumer experience.” For a diagnosis of cancer, once rendered, there are many potential touch points with both the patient and the treating clinician that can enhance the outcomes for the patient. These include maintenance of tissue in repositories for future studies, performance of future studies related to newly available treatments, access to clinical trials, and, as mentioned in the outgoing logistics, increased, and enhanced communications around the diagnosis and subsequent information. In LMICs, there is a great desire to provide such enhancements especially in settings where these activities can facilitate local research and generate much-needed local clinical trials with pharmaceutical and other industry partners. As the other steps of the value chain are improved, the continue service will come into focus and can include such activities as external quality assurance, laboratory accreditation, personnel certification, documented compliance with standards, awards, and other accolades.
To conclude, from the patient framework, the maximum value for a patient with cancer involves the earliest possible detection of the tumor and a rapid, accurate diagnostic report matched to treatment options that lead to survivorship. For a pathology laboratory, the best outcomes for patients and the best revenue model for the laboratory results from a high-volume of small samples (i.e., biopsies) reported with complete clarity. Cross subsidization of cancer diagnostic services (especially those for later staged, complex cancer patients) with other non-cancer, pathology-based reporting is crucial to create a sustainable revenue stream and ensure highest quality outcomes. Competitive advantage in pathology services specific to cancer are currently and will continued to be largely tied to the after diagnostic service and support to keep the patient on the most beneficial cancer journey.
References
Porter, M. (1985). The value chain and competitive advantage, Chapter 2 in Competitive Advantage: Creating and Sustaining Superior Performance. Free Press, New York, 33-61.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.