A 38 year old female with history of endometriosis presented to emergency department complaining of heavy vaginal bleeding for 2 weeks duration. She also reported recent diarrhea, abdominal pain, nausea, fatigue, shortness of breath, fever, and chills. On physical exam, the patient had fever, tachycardia, tachypnea, and abdominal distention with a large, 32-week size uterine mass. She was found to have microcytic anemia (Hgb 9.2 g/dL, MCV 77.1 pg), diabetic ketoacidosis (glucose 522 mg/dL, ketones and glucose in urine, A1c 9.1%), and based on the above vital signs and leukocytosis (WBC 31.75/L)met sepsis criteria.
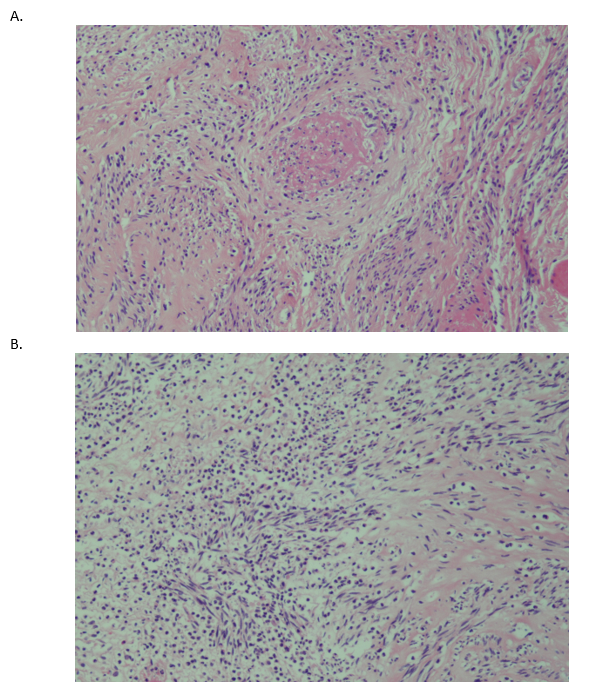
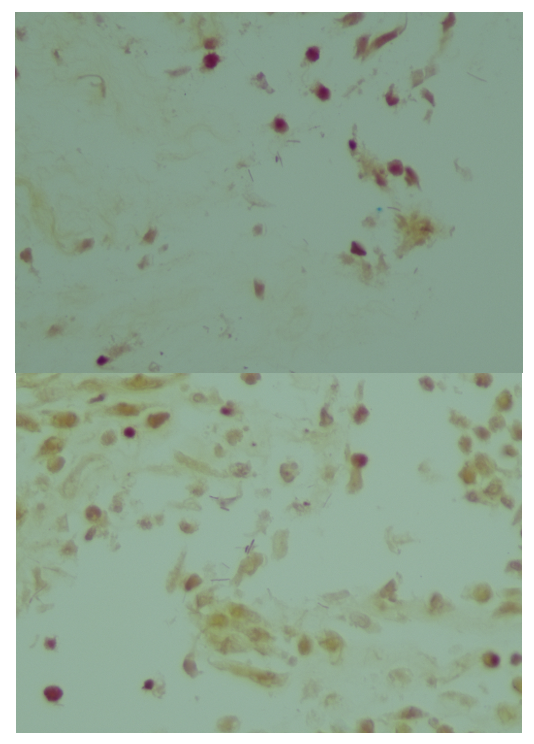
Abdominal CT revealed multiple uterine leiomyomas (fibroids), with the largest measuring up to 13.2 cm and demonstrating characteristics concerning for pyomyoma (abscess arising in leiomyoma). The patient underwent exploratory laparotomy and myomectomy. Gross images of the resected uterine mass demonstrated a circumscribed whorled nodular lesion with patchy necrosis (Image 1). Histologic examination of the resected lesion demonstrated a bland smooth muscle tumor, devoid of cytologic atypia and mitotic activity, with area of abscess formation showing necrosis and abundant neutrophils leading to a diagnosis of “Leiomyoma with severe acute inflammation, areas of necrosis and abscess formation, consistent with pyomyoma (14 cm)” (Image 2). A tissue Gram stain demonstrates multiple morphotypes of bacteria (image 3). Blood cultures, drawn on admission, flagged positive and the Gram stain revealed gram negative rods and blood, chocolate and Maconkey agars grew creamy gray non-hemolytic colonies that did not ferment lactose. MALDI-TOF mass spectrometry was performed and identified the isolate as Salmonella species. A triple sugar iron agar slant was set up to confirm the phenotype of a non-typhoidal serovar of Salmonella. Growth of the organism demonstrated abundant hydrogen sulfide production, an acidic butt, and an alkaline slant, confirming the nontyphoidal phenotype.

Discussion
Pyomyoma, also referred to as suppurative leiomyoma, is an exceedingly rare complication of uterine leiomyoma, which involves infarction of the benign tumor followed by introduction and growth of bacteria.1 Microbes can be introduced by way of ascending genitourinary infection, spread from adjacent structures, or hematogenous or lymphatic spread.2 These infections may be polymicrobial or caused by a single microorganism, and the reported causative agents vary widely, with the most common being Escherichia coli, Staphylococcus species, streptococcal species, enterococcal species, Bacterioides species, Clostridium perfringens, and Candida.3 However, there have been no reported cases of Salmonella species isolated from pyomyoma to date.
Salmonella is a gram negative bacillus belonging to the Enterobacteriacae family.4,5 Salmonella enterica, the species responsible for causing disease in humans, is sub-divided into numerous serovars, which can be broadly grouped into typhoid and nontyphoid.4,5 While the typhoid serovars cause enteric fever, the nontyphoid serovars can cause gastroenteritis and bacteremia.5 Most nontyphoid Salmonella infections are foodborne, and approximately 5% of nontyphoid Salmonella infections progress to bacteremia.4 The bacteria gain access to the bloodstream by utilizing multiple virulence factors to invade the epithelial cells of the gut.4 Salmonella can be identified in the laboratory from blood culture based on several characteristic biochemical results, including Gram stain, absence of lactose fermentation, motility, hydrogen sulfide and gas production, utilization of citrate, and decarboxylation of lysine and ornithine.
This case presents Salmonella species as the cause of sepsis in the setting of pyomyoma, a very rare entity. It is postulated that gastroenteritis caused by nontyphoid Salmonella may have been the cause of the patient’s recent diarrhea, and uncontrolled blood glucose levels in the setting of diabetes may have contributed to the progression to sepsis. We could hypothesize whether the Salmonella seeded the fibroid precipitating the abscess formation since Salmonella is known to cause abscess formation in unusual sites including having a proclivity for vascular sites (e.g., aortitis). The patient unfortunately experienced complications from her sepsis with concomitant surgery. She became unresponsive despite numerous attempts at resuscitation and died.
References
- Azimi-Ghomi O and Gradon J. Pyomyoma: Case Report and Comprehensive Literature Review of 75 Cases Since 1945. 2017. SM Journal of Case Reports. 3(4):1054.
- Obele, CC, et al. A Case of Pyomyoma following Uterine Fibroid Embolization and a Review of the Literature. 2016. Case Reports in Obstetrics and Gynecology. 2016:9835412.
- Iwahashi N, et al. Large Uterine Pyomyoma in a Perimenopausal Female: A Case Report and Review of 50 Reported Cases in the Literature. 2016. Molecular and Clinical Oncology. 5(5):527-531.
- Eng SK, et al. Salmonella: A Review on Pathogenesis, Epidemiology, and Antibiotic Resistance. 2014. Frontiers in Life Science. 8(3):284-293.
- Coburn B, et al. Salmonella, the Host and Disease: A Brief Review. 2006. Immunology & Cell Biology. 85(2):112-118.
-Heather Jones is a first year AP/CP resident at UT Southwestern.
-Katja Gwin is an Assistant Professor at UT Southwestern in the Department of Pathology and specializes in gynecologic pathology.
-Dominick Cavuoti is a Professor at UT Southwestern in the Department of Pathology and specializes in cytopathology, infectious disease pathology and medical microbiology.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.

Can you earn CME credit for reading these case studies?
Unfortunately, no.