I quickly transitioned from from learning at Jefferson to teaching at Jefferson less than 6 months after I graduated from the Cytotechnology program. Assuming this new role of teaching future cytotechnologists was a refreshing twist after continuously learning at work. I stood at the podium as an alumna in my previous classroom with a breadth of fresh material to work with, appreciate, and share. At the beginning of each lecture, I would check in on my students, ask them how their other classes were going, ask if they had any questions, and then, I would share an interesting case from my work week thus far. Aside from the weekly lecture on ancillary techniques, such as molecular and immuno-diagnostics, I assigned multiple activities such as journal club/conferences, discussions, and my personal favorite – a mock tumor board. Each student would take turns playing the role of the physician, radiologist, cytotechnologist, pathologist, and oncologist (surgical, medical, or radiation). For my first year of instruction, I had assigned the group their “tumor” of interest, but I quickly encouraged their creativity run rampant during subsequent years.
Despite working in a cancer center and being able to recognize some fairly obscure tumors with little experience, I did not realize how much I still had to learn, even as a part-time lecturer and full-time cytotechnologist. These tumor boards taught me so much more than I expected, and I am forever thankful for the experience of having such wonderfully bright students teach ME! For one very memorable tumor board, the students elected to present the diagnosis and treatment of a male patient with multiple myeloma. Yes, plasma cells! Plasma cell neoplasm, plasmacytoma, multiple myeloma. Awesome, let’s see what this group can do! The “physician” said the patient complained of widespread bone pain, malaise, and recurrent fevers and infections. The “radiologist” presented the images of osteolytic lesions throughout the skull and vertebrae, the latter of which core biopsies and FNAs were obtained. The “cytotechnologist” described a mix of plasmablastic cells, as well as mature and immature plasma cells, some with clock face chromatin and a perinuclear hof (which is my telltale feature that I now emphatically describe to everyone else). The “pathologist” bypassed flow cytometry and performed Kappa/Lambda light chain immunohistochemistry on the core biopsy, diagnosing the patient with multiple myeloma. Unfortunately, due to the extent of the patient’s disease, the “oncologist” and her team could not increase the life expectancy, and the student’s patient expired.
Now, whenever I have a plasma cell neoplasm or multiple myeloma case, I think back to my students and their mock tumor board and everything they taught me. I just recently attended an FNA on a 79-year-old male with a history of multiple myeloma who presented with a PET positive right facial mass and right cervical lymph nodes. The radiologist performed an ultrasound-guided FNA of a right peri-mandibular soft tissue mass, and it took everything in me to not tell the radiologist anything more than “adequate.” But when I saw those perinuclear hofs, I was elated to have a definitive diagnosis!

Later that afternoon, I couldn’t wait to screen my pap-stained slides. The clock face chromatin was so beautiful! My cell block the following morning highlighted the textbook perfect features diagnostic of a plasma cell neoplasm.

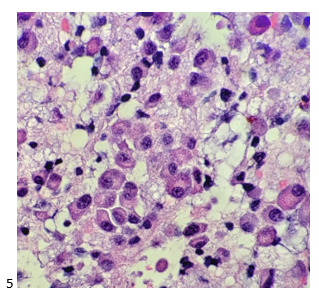
The attending pathologist ordered a routine myeloma immunocytochemistry panel, including CD138, kappa light chain, lambda light chain, CD20, CD45, and MUM1.
Immunocytochemical stains performed on the unstained paraffin sections showed the tumor to be positive for CD138, kappa light chain, and MUM1, focal equivocal staining for CD20, and negative staining for lambda and CD45. The case was signed out as a plasma cell neoplasm.

The bone marrow core biopsy was sent for Cytogenetic Microarray Analysis and Next Generation Sequencing. The CMA results revealed gains of chromosomes 3, 5, 9, 11, 15, 19, and 21 and losses of chromosome segments 1p and 2p and 7 p in mixed states. Loss of 1p is associated with a poorer prognosis for multiple myeloma. Next gen sequencing identified a tumor mutation burden of 8.4Muts/Mb with mutations detected in the following genes: FAM46C, BRAF, KAT6A, TSC1, KRAS, FLT3, and NFKBIA.

-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
