A 7 year old Congolese male presented with pruritic, erythematous, non-flaky rash on top of his scalp for the past 3 weeks. The rash in non-painful, but continues to spread. His mother has been applying hydrocortisone cream nightly, with no improvements.
Colony morphology on fungal media.Organism morphology on lactophenol analine blue scotch tape prep.
Laboratory Identification
A hair sample was obtained for fungal culture. Colonies were yellow and waxy with feet-like projections. Microscopic morphology on lactophenol analine blue scotch tape prep revealed broad hyphae with tortuous branches. The hyphae lacked obvious micro and macro conidia, raising the suspicion for Trichophyton violaceum.
Discussion
Trichophyton violaceum is an anthropophilic fungus seen predominantly in North Africa, East Asia and parts of the Middle East. It forms slow growing with glabrous colonies. Microscopically, broad tortuous hyphae are seen. Microconidia and Macroconidia are notably absent. T. violaceum causes Tinea Capitis, which can be acquired through scalp contact with the dermatophyte, either with direct contact with an infected individual or an object. It can also affect skin, nails and beards. It manifests clinically as pruritic scaly patches with alopecia, often producing black dots. Affected hairs demonstrate an endothrix infection.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
The U.S. Food and Drug Administration today announced the availability of an investigational test to screen blood donations for Zika virus. The screening test may be used under an investigational new drug application (IND) for screening donated blood in areas with active mosquito-borne transmission of Zika virus.
A 39 year old African American male presents to the Emergency Department with a three day history of headaches and fatigue. The patient describes his headache as a sharp, constant pain that is exacerbated by movement. He also has been experiencing blurred vision and feeling unstable on his feet. His past medical history is significant for HIV diagnosed 8 years ago. On admission, his absolute CD4 count is 104 with a viral load of 150 vc/ml. He is compliant with his anti-retroviral therapy and Bactrim prophylaxis. Physical exam is unremarkable except for oral thrush. Imaging reveals multifocal areas of enhancement throughout the brain and cerebellum with associated vasogenic edema, which was thought to most likely represent an infectious process. The patient was taken to the operating room for a brain biopsy. Tissue was sent to surgical pathology and the microbiology laboratory for evaluation.
Laboratory identification:
Figure 1. Brain tissue with pyogranulomatous inflammation and a budding yeast form (H&E 400x).Figure 2. Brain tissue with many yeast forms present exhibiting broad based budding (GMS 400x).Figure 3. Growth of a white-tan mold on Sabouraud dextrose, SAB with chloramphenicol and Mycosel agar slants (left to right).Figure 4. Narrow septate hyphae with fine conidiophores giving rise to round shaped conidia (Lactophenol cotton blue, 400x)
The histology results were reviewed first and the H&E stain showed a pyogranulomatous inflammatory response with budding yeast forms. These findings were better visualized on the GMS stain which illustrated numerous yeast forms ranging in size with frequent broad based budding. In the microbiology laboratory, a white-tan mold grew on Sabouraud dextrose, SAB with chloramphenicol and Mycosel agar slants after 18 days of incubation at 30°C. On microscopic examination, the lactophenol cotton blue prep revealed narrow septate hyphae with round conidia at the end of fine conidiophores (characterized as a lollipop appearance). These finding are consistent with a diagnosis of Blastomyces dermatiditis and were confirmed with a DNA probe. Other pertinent laboratory results included urinary antigens positive for both Blastomyces and Histoplasma and a negative cryptococcal antigen in the serum.
Discussion:
Blastomyces dermatiditis is a thermally dimorphic fungus found in the Midwest, Ohio and Mississippi River valleys and the south central portion of the United States. The infection is obtained by inhalation of spores from decaying wood along rivers and patients typically show symptoms consistent with pneumonia. In some cases, particularly in immunocompromised patients, dissemination to the skin, bone and central nervous system can occur.
Morphologic diagnosis can be made from surgical pathology specimens which show broad based, budding yeast forms with a double contoured cell wall, ranging in size from 8-15 µm. In the microbiology laboratory, the mold form grows slowly (2-3 weeks) and is characterized by narrow septate hyphae with delicate conidiophores bearing round to oval conidia which are described as lollipop-like. Due to that fact that Blastomyces is not able to be differentiated from the mold form of Paracoccidioides brasiliensis and Chrysosporium spp., confirmation of the identification is necessary. Traditionally, this was done by temperature induced culture conversion of the mold form to the yeast form but due to the availability of rapid, commercially available DNA probes specific for the exoantigen of Blastomyces dermatiditis, this test is more commonly utilized currently.
Other supplemental tests used in the diagnosis include a Blastomyces urinary antigen which shows good sensitivity in both pulmonary and disseminated disease. In our case, the positive urinary antigen for Histoplasma was considered to be a false positive result due to known cross reactivity with Blastomyces as a result of shared polysaccharides.
Cryptococcus neoformans was also included in the differential diagnosis due to the patient’s HIV status, presenting symptoms and the fact it is a common cause of fungal meningitis in individuals with CD4 counts below 200. This infection was ruled out due to a negative serum cryptococcal antigen. In addition, in tissue Cryptococcus would show variably sized (2-20 µm), narrow based yeast forms with a prominent polysaccharide capsule and grow quickly as a yeast in fungal culture.
In the case of our patient, he was started on Amphotericin B based on the histology results. He experienced resolution of his headaches and recovered well following surgery. His was discharged to an extended care facility for 6 weeks of continued IV antifungal therapy before being placed on oral voriconazole.
-Srinivasa Chekuri, MD, is a 4th year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories.
If you’re involved with molecular diagnostics, then L. J. Lee’s team at the Ohio State University would like your input. They’ve developed a new technology using molecular beacons and would love for lab directors, managers, and bench technologists to answer this short survey.
I haven’t been able to blog as much of late. It’s been a busy year with more than its fair share above the usual crises that a chief resident is expected to handle – an “August year” for me as my program director put it. But I’ve learned a lot and have been lucky to have the support of my attendings, program coordinator, and program director to help. Even when we’ve not always agreed on what is best for our residents, I’ve always been allowed to speak up for our residents and felt as if our concerns were heard and acknowledged even if policies didn’t go our way. I think that’s the biggest strength of a smaller program–the ability to form strong relationships with mutual respect, whether it is with one’s mentors, peers, or hopefully, both–and I know we will cheer each other on when we hear of each other’s accomplishments in the future even if we won’t see each other daily as we do now because of those bonds we built during these past couple of years. The lessons I’ve learned regarding “soft skills” have been equally as important as the knowledge I’ve gained about my favorite lymphomas or molecular mutations. And four years is really shorter than one might think to fit in all we need to as AP/CP pathology residents, so see it for the gift it is–protected time to grow into the physician you want to be. I see the fruits of these lessons more clearly now as I prepare to graduate. Much of it was obtained through mentorship, formal and informal, from those more experienced and with my best interests at heart.
So here are some pearls I’d like to hand down:
Know thyself as early as possible: Be honest with yourself about your strengths and weaknesses so that you can build on the one while working on the other. As we have now signed on to be life-long learners, identify what works for you early or adjust those learning habits which might have worked before but are no longer working. Designate a couple of hours on a weekend day every week to do learning above and beyond what is expected for your current rotation and consistently stick to it. If you can, designating an hour everyday would be even better and it doesn’t have to be hard core studying like our med school days—you can leisurely read a review article, watch TedMed videos, casually look over boards materials or qbanks from day 1, and so forth as long as you do set aside time consistently. Take advantage of experiential opportunities to help decide early where you see yourself as a physician (academics, private practice, commercial lab, subspecialty, etc) in the future so that you can plan as early as possible your rotations, electives, opportunities, and networking with that goal in mind. But most importantly, knowing who you are, what you believe in, how you work best, and what you want and knowing early, will help you plan and see opportunities earlier. But always, be true to yourself.
Time management is key: Learning to plan early and efficiently is a skill and it takes time to learn. Honestly, I’m not the best on a daily basis unless I take time ahead of time to plan my day, which I don’t always do, but plan to be better about during fellowship. But I do know how to plan effectively to juggle multiple long-term projects with deadlines at a time. You will constantly hear about time management – whether on rotation evaluations or during fellowship interviews. I find that those who are very good at time management, all have checklists and planners (whether hard copy or digital) so maybe they’re on to something there. Whatever works for you, being a deliberate planner ahead of time will serve you well.
Be proactive: In some way, we’ve all be conditioned in a passive learning style where those who are more experienced hand down information to us which we are expected to regurgitate or ruminate on and respond. During residency, we don’t have the strict structure we are used to from medical school as we may be only given loose guidelines but are expected to figure out how best to manage our time on our own. We no longer have every hour planned out for us and so the quicker you learn to plan ahead and effectively use your time while at work, the more time you’ll have for personal activities. Don’t just do the minimum but use gaps in your time during the day to study, to build relationships with mentors with whom to work on book chapters, abstract submissions (for posters/platform presentations at conferences), and publications, to attend conferences/tumor boards outside your rotation even in non-pathology departments, to work with others outside of pathology on interdisciplinary projects. In some ways, these activities are networking without our even realizing it. For the rest of our lives, we will constantly be judged and compared to others by our character and work ethic and that often will include tangible items on our CV whether this is fair or not. Challenge yourself on every rotation by trying to do as much as a junior attending would within the limits of what you are allowed to do and not just the minimum.
Get involved in advocacy: Participate in leadership positions at an organized level–within our professional organizations, with interdisciplinary teams within your hospital, or with volunteer organizations in your community. Bringing about change takes time but if done with a positive goal in mind, can have such a rewarding impact on those we wish to serve as well as yourself. You might discover a previously unknown passion or skill you possess that you can share. Before residency, I was heavily involved with on-the-ground, upstream-minded health equity efforts in immigrant and minority communities. And while I took a hiatus from my work due to residency training, I know that as a future public health pathologist-scientist with both public health and research training, I will return to working to change those systemic and institutionalized societal structures that maintain health inequity within those communities. So it’s now your time to find your passion and to give back. Pay it forward for every good gesture someone has shown you.
Build relationships with mentors: Since I’ve been involved with organized medicine, I’ve always heard the word “networking”. Too me, it always seemed somewhat a Machiavellian “ends justify the means” insincere word but I guess that’s all up to interpretation. What I prefer to say is focus on finding colleagues with whom you share values and passions, who you respect and would like to emulate, and with whom in the future, you might want to collaborate. If your premise is sincere, opportunities always unexpectedly follow has been my experience.
Step outside your comfort zone: As busy physicians-in-training who are used to structure and consistency, it’s good every once in a while to try something new. You never know what you may find–it may even turn out to be a new passion for you. Life is too short and you want to live it without regrets. You want to say when your time comes that you lived life to the fullest and maybe even tried some things that scared but surprisingly made you happy.
Recharge with some “me” time: All work and no play can make any of us dull and cranky. Set aside time to spend with friends (especially non-physician friends) and family and do non-work related activities. Especially when life is getting you down, some time away from thinking about work may be the recharge you need.
-Betty Chung, DO, MPH, MAis a fourth year resident physician at Rutgers – Robert Wood Johnson University Hospital in New Brunswick, NJ.
Transfusion is the most common procedure performed in our in-patient and out-patient facilities, representing a high-volume, high-risk process. Sadly enough, general knowledge regarding appropriate transfusion practice, anemia management, blood conservation modalities and other PBM strategies are notoriously lacking for most healthcare providers.
The Biomedical Excellence for Safer Transfusions (BEST-TEST) investigators highlight the need for ongoing commitment to education. This group first developed, validated and studied a transfusion medicine knowledge assessment tool in 2014 as an international collaborative for evaluation of internal medicine residents.¹ Internal medicine trainees in this original BEST-TEST study had a mean knowledge score of 45.7%. Just this February, the BEST-TEST2 results were published and, once again, reinforce the need for a focused curriculum for our physicians-in-training.² Hematology residents in the current BEST-TEST2 study had a mean score of 61.6%. Of concern is that the lowest scores were related to questions regarding transfusion reactions/transfusion-associated adverse events.
Having been 20 years in private practice and subsequently 5 years consulting with numerous facilities on Transfusion Medicine/Patient Blood Management issues, it is glaringly apparent to me that we, as laboratorians, play a vital role in the day-to-day “teachable moments”. Studies such as these, with tools that provide meaningful data, could potentially be expanded to target education for all healthcare providers, ultimately utilized for on-going updates in the field of Transfusion Medicine and PBM.
As members of ASCP, it is incumbent upon us to take an active role in the provision of education for our colleagues. Sharing the evidence and experience will promote the effort for optimal, safer patient care and potentially avoid unnecessary transfusion and their potential serious risks.
References
1. Haspel R et al. Transfus 2014; 54: 1225-1230.
2. Lin Y et al. Transfus 2016; 56: 304-310.
-Dr. Burns was a private practice pathologist, and Medical Director for the Jewish Hospital Healthcare System in Louisville, KY. for 20 years. She has practiced both surgical and clinical pathology and has been an Assistant Clinical Professor at the University of Louisville. She is currently available for consulting in Patient Blood Management and Transfusion Medicine. You can reach her at cburnspbm@gmail.com.
Science writer Maryn McKenna has a great write up about the feasibility of keeping mosquito-borne viruses–Zika in particular–out of the US blood supply. You can read about it at her blog Phenomena.
A 77 year old male with history of asthma, atrial fibrillation, and recurrent respiratory distress when visiting Vermont presented to the ED with progressive dyspnea and wheezing for the past 4 days. Two days prior, he required a “breathing treatment” at his PCP. One day ago, he saw his PCP and was prescribed prednisone and azithromycin. He denies cough, fevers, or chills. He used his albuterol and Advair inhalers which barely helped. He was found to be in Afib with RVR to the 160s, a respiratory rate in the 40s, and an oxygen saturation of 70%.
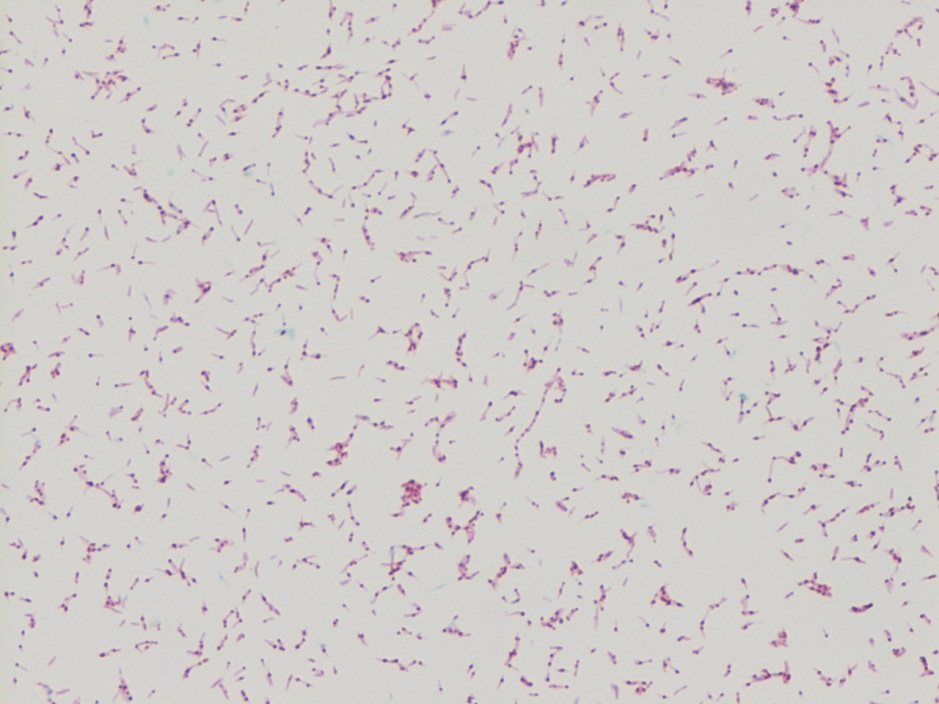
Kinyoun stain revealing broad rods with cross-barring.Colony growth on Lowenstein-Jensen medium.
Lab Identification
The organism was auramine fluorescent stain positive from the broth. The AFB culture bottle was sub-cultured to agar based medium and Lowenstein-Jensen medium, which yielded small yellow colonies. Kinyoun stain revealed broad rods with cross-barring. The organisms produced a yellow pigment when exposed to light, and a nucleic acid probe for Mycobacterium kansasii was positive.
Discussion
Mycobacterium kansasii was discovered in 1953 by Buhler and Pollack. It is an acid fast bacillus that produces yellow pigment when exposed to light (photochromogen). The bacilli are thick, long and cross-barred and have been described as ladder-like. It is prevalent in the Midwest and Southeast, and is the second most common cause of nontuberculous mycobacteria disease in patients with AIDS. Mycobacterium kansasii manifests as lung disease that clinically appears similar to tuberculosis. It can also cause local disease of the skin and subcutaneous tissue, as well as lymphadenitis and disseminated disease. Symptoms are more severe in immunocompromised hosts. Mycobacterium kansasii is generally acquired via either aspiration or local inoculation from the environment, with little evidence to support person to person transmission.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 6 year-old girl with a history of posterior fossa ependymoma presented with a one month history of fever, headaches, vomiting and more recently, neck stiffness. Additional history includes remote tumor resection followed by radiation and chemotherapy resulting in remission, with a residual ventriculoperitoneal shunt (VPS). Her parents reported she was in good health until approximately 1 month prior to presentation and is up to date on her immunizations. She was previously seen by her primary care physician for her symptoms and treated her with amoxicillin for suspected strep throat. Upon admission, she received supportive therapy for her symptoms after she was found to have tumor recurrence on imaging. The patient was scheduled for resection approximately two weeks after discharge and on post-operative day two she developed fever, vomiting and neck stiffness again. At this time, blood cultures were drawn and a lumbar puncture (LP) was performed. Cerebrospinal fluid (CSF) from both the LP and VPS submitted for fluid analysis (Table 1) and culture.
Table 1: Cerebrospinal Fluid Analysis
Spinal Fluid
LP
VPS
Appearance
Clear
Clear
Nucleated cells
1075 cells/μL
628 cells/μL
RBC
150 cells/μL
35 cells/μL
Polys
94%
87%
Lymphs
2%
6%
Mono/Macrophage
4%
7%
Glucose
68 mg/dL
13 mg/dL
Protein
69 mg/dL
164 mg/dL
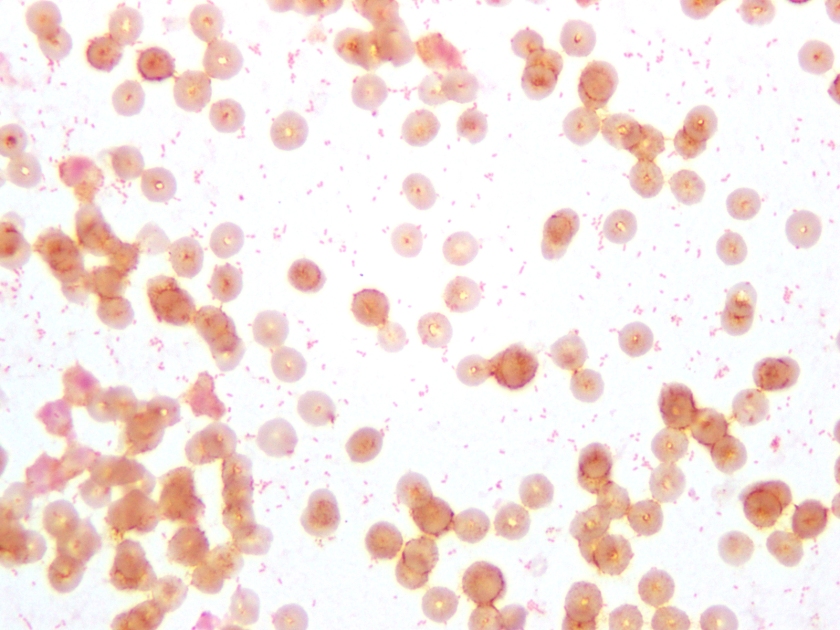
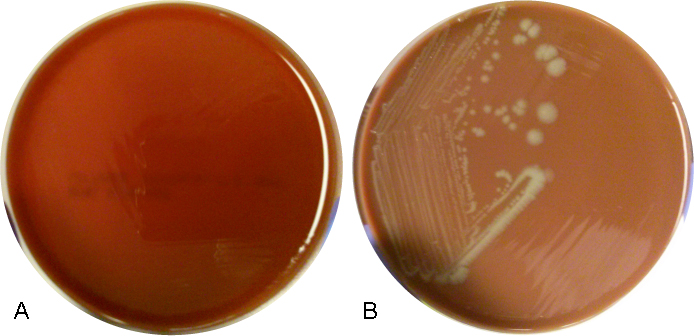
Figure 1. Gram stain of the pathogen isolated from aerobic blood culture, showing gram-negative coccobacilli, sometimes in pairs. The same organism was seen on the patient’s CSF Gram stain.Figure 2. Aerobic blood culture on (A) 5% sheep blood agar plate (BAP), showing no growth and on (B) chocolate agar plate (CAP), showing round, smooth, opaque grey-yellow colonies.
Culture results:
The CSF Gram stain showed rare, paired, Gram-negative diplococci, which could raise suspicion for Neisseria meningitidis, however the typical flattened sides of adjacent bacteria were not observed. Rather, the morphology was more consistent with Gram-negative coccobaccilli, which is better demonstrated on Gram stain of the blood culture (Figure 1). Culture of both the CSF and blood specimens grew fairly large, smooth, round, opaque grey-yellow colonies on CAP, however showed no growth on BAP (Figure 2), suggesting a fastidious organism requiring growth factors. The colonies were both catalase and oxidase positive. The organism was identified as Haemophilus influenzae by MALDI-TOF MS (matrix-assisted laser desorption/ionizations time-of-flight mass spectrometry). This H. influenzae isolate was non-typeable by slide agglutination serotyping performed at the state public health laboratory.
Discussion:
H. influenzae are small, pleomorphic, gram-negative rods or coccobacilli that are non-motile. They are facultative anaerobes that grow best between 35-37°C with 5% CO2. H. influenzae is a fastidious species, requiring hemin (X factor) and nicotinamide-adenine-dinucleotide (NAD/V factor) for growth, which are both available in chocolate agar, but not blood agar. On chocolate agar, the colonies are non-hemolytic, typically large, smooth, round and convex with an opaque, colorless or grey hue. Encapsulated strains, including H. influenzae serotype b (Hib), appear mucoid and are typically small, grey colonies on CAP. Isolates are catalase and oxidase positive. H. influenzae displays the “satellite phenomenon” when grown near Staphylococcus aureus. This occurs when colonies of S. aureus lyse nearby red blood cells releasing hemin and NAD in the media. The presence of extracellular hemin and NAD allow colonies of H. influenzae to grow in the immediate vicinity of S. aureus.
H. influenzae is widely distributed in humans, colonizing the nose and throat and is spread from person-to-person via direct contact or respiratory droplets. Severe infections, including pneumonia, bacteremia and meningitis, affect predominantly infants and children. The American Academy of Pediatrics recommends routine vaccination with the Hib conjugate vaccine for infants aged 2 through 6 months (2 or 3 doses, depending on vaccine product) followed by a booster dose at age 12 through 15 months. Hib is the only serotype preventable by vaccine. Prior to routine vaccination in the US, approximately 20,000 children under the age of 5 were infected with H. influenzae and 3-6% died each year.
-Petra Rahaman, MD is a 4th year Anatomic and Clinical Pathology resident at UT Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
Today NPR featured a write up about how to test for the Zika virus. While It didn’t delve into the diagnostic testing side of things as much as Lab Medicine’s recent podcast, it does give readers a good overview. In addition, it highlights how critical laboratory professionals and pathologists are to public health and infectious disease prevention.