A 6 year-old girl with a history of posterior fossa ependymoma presented with a one month history of fever, headaches, vomiting and more recently, neck stiffness. Additional history includes remote tumor resection followed by radiation and chemotherapy resulting in remission, with a residual ventriculoperitoneal shunt (VPS). Her parents reported she was in good health until approximately 1 month prior to presentation and is up to date on her immunizations. She was previously seen by her primary care physician for her symptoms and treated her with amoxicillin for suspected strep throat. Upon admission, she received supportive therapy for her symptoms after she was found to have tumor recurrence on imaging. The patient was scheduled for resection approximately two weeks after discharge and on post-operative day two she developed fever, vomiting and neck stiffness again. At this time, blood cultures were drawn and a lumbar puncture (LP) was performed. Cerebrospinal fluid (CSF) from both the LP and VPS submitted for fluid analysis (Table 1) and culture.
Table 1: Cerebrospinal Fluid Analysis
| Spinal Fluid | LP | VPS |
| Appearance | Clear | Clear |
| Nucleated cells | 1075 cells/μL | 628 cells/μL |
| RBC | 150 cells/μL | 35 cells/μL |
| Polys | 94% | 87% |
| Lymphs | 2% | 6% |
| Mono/Macrophage | 4% | 7% |
| Glucose | 68 mg/dL | 13 mg/dL |
| Protein | 69 mg/dL | 164 mg/dL |
Culture results:
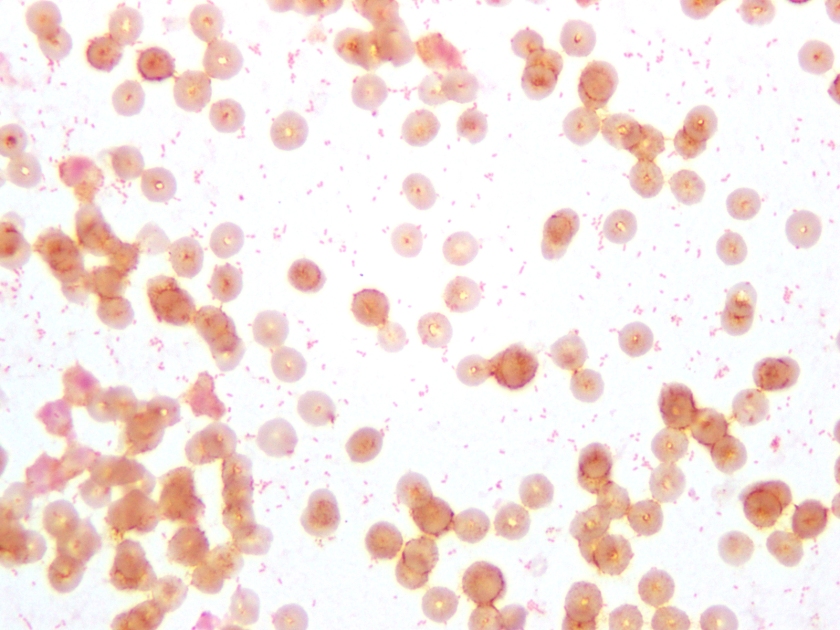
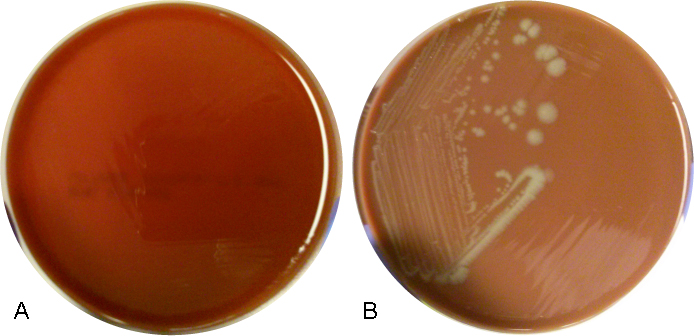
The CSF Gram stain showed rare, paired, Gram-negative diplococci, which could raise suspicion for Neisseria meningitidis, however the typical flattened sides of adjacent bacteria were not observed. Rather, the morphology was more consistent with Gram-negative coccobaccilli, which is better demonstrated on Gram stain of the blood culture (Figure 1). Culture of both the CSF and blood specimens grew fairly large, smooth, round, opaque grey-yellow colonies on CAP, however showed no growth on BAP (Figure 2), suggesting a fastidious organism requiring growth factors. The colonies were both catalase and oxidase positive. The organism was identified as Haemophilus influenzae by MALDI-TOF MS (matrix-assisted laser desorption/ionizations time-of-flight mass spectrometry). This H. influenzae isolate was non-typeable by slide agglutination serotyping performed at the state public health laboratory.
Discussion:
H. influenzae are small, pleomorphic, gram-negative rods or coccobacilli that are non-motile. They are facultative anaerobes that grow best between 35-37°C with 5% CO2. H. influenzae is a fastidious species, requiring hemin (X factor) and nicotinamide-adenine-dinucleotide (NAD/V factor) for growth, which are both available in chocolate agar, but not blood agar. On chocolate agar, the colonies are non-hemolytic, typically large, smooth, round and convex with an opaque, colorless or grey hue. Encapsulated strains, including H. influenzae serotype b (Hib), appear mucoid and are typically small, grey colonies on CAP. Isolates are catalase and oxidase positive. H. influenzae displays the “satellite phenomenon” when grown near Staphylococcus aureus. This occurs when colonies of S. aureus lyse nearby red blood cells releasing hemin and NAD in the media. The presence of extracellular hemin and NAD allow colonies of H. influenzae to grow in the immediate vicinity of S. aureus.
H. influenzae is widely distributed in humans, colonizing the nose and throat and is spread from person-to-person via direct contact or respiratory droplets. Severe infections, including pneumonia, bacteremia and meningitis, affect predominantly infants and children. The American Academy of Pediatrics recommends routine vaccination with the Hib conjugate vaccine for infants aged 2 through 6 months (2 or 3 doses, depending on vaccine product) followed by a booster dose at age 12 through 15 months. Hib is the only serotype preventable by vaccine. Prior to routine vaccination in the US, approximately 20,000 children under the age of 5 were infected with H. influenzae and 3-6% died each year.
References:
1. Ledeboer N, Doern G. 2015. Haemophilus, p 667-684. In Jorgensen J, Pfaller M, Carroll K, Funke G, Landry M, Richter S, Warnock D (ed), Manual of Clinical Microbiology, 11th Edition. ASM Press, Washington, DC.
2. http://www.cdc.gov/meningitis/lab-manual/chpt09-id-characterization-hi.html
3. http://www.cdc.gov/hi-disease/index.html
-Petra Rahaman, MD is a 4th year Anatomic and Clinical Pathology resident at UT Southwestern Medical Center.

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
