A 77 year old male with history of asthma, atrial fibrillation, and recurrent respiratory distress when visiting Vermont presented to the ED with progressive dyspnea and wheezing for the past 4 days. Two days prior, he required a “breathing treatment” at his PCP. One day ago, he saw his PCP and was prescribed prednisone and azithromycin. He denies cough, fevers, or chills. He used his albuterol and Advair inhalers which barely helped. He was found to be in Afib with RVR to the 160s, a respiratory rate in the 40s, and an oxygen saturation of 70%.

Lab Identification
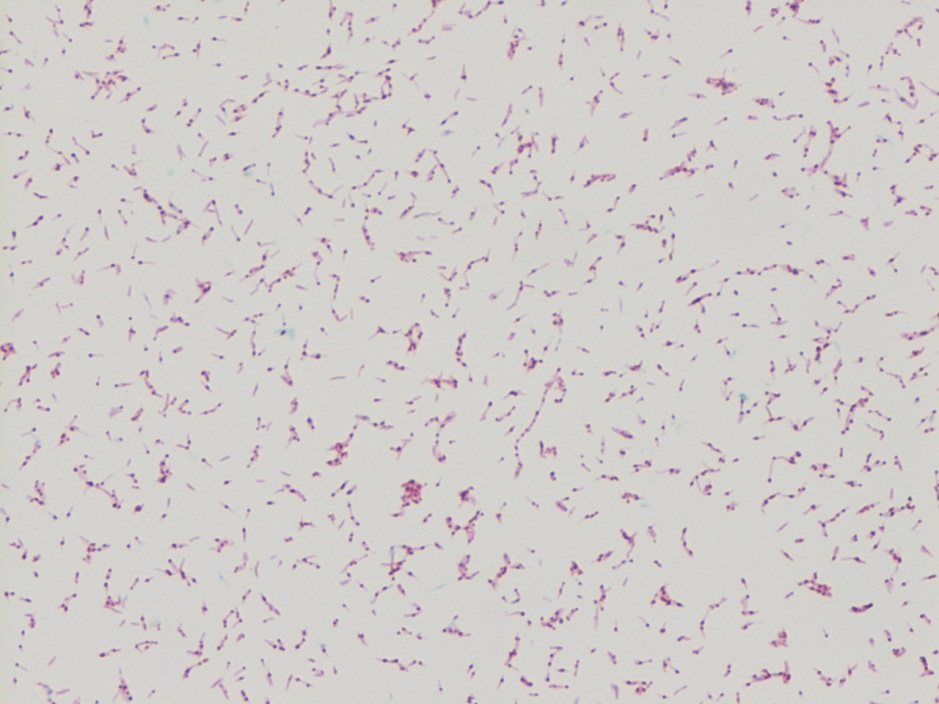
The organism was auramine fluorescent stain positive from the broth. The AFB culture bottle was sub-cultured to agar based medium and Lowenstein-Jensen medium, which yielded small yellow colonies. Kinyoun stain revealed broad rods with cross-barring. The organisms produced a yellow pigment when exposed to light, and a nucleic acid probe for Mycobacterium kansasii was positive.
Discussion
Mycobacterium kansasii was discovered in 1953 by Buhler and Pollack. It is an acid fast bacillus that produces yellow pigment when exposed to light (photochromogen). The bacilli are thick, long and cross-barred and have been described as ladder-like. It is prevalent in the Midwest and Southeast, and is the second most common cause of nontuberculous mycobacteria disease in patients with AIDS. Mycobacterium kansasii manifests as lung disease that clinically appears similar to tuberculosis. It can also cause local disease of the skin and subcutaneous tissue, as well as lymphadenitis and disseminated disease. Symptoms are more severe in immunocompromised hosts. Mycobacterium kansasii is generally acquired via either aspiration or local inoculation from the environment, with little evidence to support person to person transmission.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
