Leaders’ decisions and actions have moral ramifications, both on an individual and an organizational level. There are three factors of moral development, namely moral capacity, moral courage, and moral resiliency.
Being able to recognize a dilemma as a moral issue is one of the critical aspects of leadership. Such awareness is referred to as moral capacity, which influences the characteristics and recognition of a moral issue. There are multiple aspects that influence a leaders’ moral capacity. The first aspect is their previous experiences with moral dilemmas and how much they learned from them. The second is to what extent a leader is able to see and understand the multiple perspectives of an issue. The third is how leaders view their role and whether or not that incorporates a moral view.
It is not enough to understand and recognize a moral dilemma, it is important to act on it. Such moral courage is especially important when under pressure to act immorally. Such pressure can come from peers, supervisors, or the entire organization. Therefore, the more moral courage someone has, the more likely it is that they take a moral action or make a moral decision. One important aspect of moral courage is the notion of willpower. Willpower is a muscle that people can practice with small tasks, such as drinking a glass of water before breakfast. The more people practice it on small tasks, the more likely they are to use it during challenging situation, such as making a moral decision when pressured to do otherwise.
Moral resiliency is an extension of moral courage. While moral courage focuses on the strength to make moral decisions in the short-term, moral resiliency is a process through which leaders continuously adapt their moral compass and actions. Moral resiliency is this what creates sustainable moral decision-making.
Depending on how leadership effectiveness is defined, moral behavior can either make leaders more or less effective. When looking at effectiveness in the short term, it is possible that moral behavior can impede effectiveness if measured in terms of money or short-term success. However, when looking at effectiveness in the long term, moral behavior increases leaders’ effectiveness. The more honest, and thus morally, people behave, the more effective they are. In a world that is becoming more globalized, it is critical for leaders to understand that culture influences moral and ethical behavior. In other words, what is moral in one culture might be immoral in another. To increase leaders’ effectives it is therefore important to understand the cultural implications of behavior and to be aware of the differences in appropriate and effective behavior.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
#PathTweetAward is a crowdfunded award created
on Twitter by pathologists to recognize pathologists and pathology trainees who
post exemplary educational tweets in the field of anatomic or clinical pathology.
How and when
was #PathTweetAward started?
The idea for an “educational pathology Tweet ofthe year” award was proposed on Twitter on April 6, 2018.
The tweet that launched the concept of #PathTweetAward.
The hashtag#PathTweetAward was created the next day based on a suggestion by Dr. Amy Deeken (@AmyHDeekenMD), a pathologist from Ohio who is active on social media. A Twitter handle (@PathTweetAward) and a promotional video to create awareness about the award were created shortly thereafter by Dr. Muhammad Ahsan (@ahsanuitis), a pathologist from Pakistan. The award was supported online by several pathologists with a prominent social media presence, including Dr. Jerad Gardner, Dr. Kamran Mirza, Dr. Christina Arnold, Dr. Julie Teruya-Feldstein and Dr. Kalyani Bambal.
What is
crowdfunding? How was #PathTweetAward crowdfunded?
Crowdfunding is a fundraising method in which small amounts of money are contributed by a large number of people, typically via the internet. Crowdfunding for #pathtweetaward was made possible by Dr. Amy Deeken, who started up a GoFundMe account for the award on April 7, 2018 (gofundme.com/5dakxso) and created a promotional video. Incredibly, the fundraising goal of $1000 was reached within a single day of setting up the GoFundMe account. At the time of this writing, the account has raised $1550, generously donated by 26 individuals (predominantly pathologists) over a period of 6 months.
The GoFundMe account that funds #PathTweetAward.
Who is
eligible for the award?
Pathologists in practice, pathology residents,
and pathology fellows anywhere in the world are eligible for the award. To be
considered, a tweet with educational value should be posted on Twitter and
brought to the attention of the screening judges by using the hashtag
#PathTweetAward.
Who is
allowed to use the hashtag #PathTweetAward?
Anyone can use the hashtag. Any pathologist anywhere in the world can tag an educational post on Twitter in a reply or retweet. An example is shown in the image below. Pathologists can also self-tag their own tweets if they wish.
To nominate a tweet for the award, simply reply to the original tweet and type #PathTweetAward. You can also “retweet with comment” and type #PathTweetAward in your comment.
Are the
awards monetary?
Yes, the current plan is to award four
monetary prizes each year ($500, $300, $200 and $100), including two awards in
the open group and two awards for trainees. The
Pathologist magazine and the American Society for Clinical Pathology (ASCP)
have generously offered additional non-monetary support, mainly in the form of promotion
of award-winning tweets and awardees.
How are
winners selected?
Judges for #PathTweetAward are pathologists who are active on Twitter. There are three panels of judges, selected with diversity and inclusion in mind; judges include women and men, trainees and faculty, community pathologists and academics. A different panel of judges will be selected each year. The bulk of the work is shouldered by two panels of five screening judges each. One, led by Chicago hematopathologist Kamran Mirza, MD, PhD,screens tweets from trainees only. The other, led by Canadian head and neck pathologist Bin Xu, MD, screens tweets from an “open” group that includes trainees and practicing pathologists.
Screening
judges (for trainee tweets only)
Screening
judges (for “open” category, including all pathologists, including trainees)
Final
judges
Kamran
Mirza, MD (group leader)
Bin Xu, MD (group leader)
Jerad
Gardner, MD (group leader)
Elvira
Gonzalez-Obeso, MD, PhD
Eman
Aljufairi, MD
Silvija
Gottesman, MD
John
Gross, MD
Daniel
Skipper, MD
Valerie
Fitzhugh, MD
Adam L. Booth,
MD
Yiang Hui,
MD
Laura G.
Pastrian, MD
Pallavi A.
Patil, MD
Chen Yang,
MD
Geronimo
Junior, MD
Table 1. Judges for #PathTweetAward (2018)
Each week, tweets tagged with the hashtag #PathTweetAward are collated by a screening judge and posted publicly on Twitter using the “Moments” feature. These collections serve as a repository of the best tweets, from which each panel of screening judges selects a “tweet of the month” to be sent at the end of the year to the final panel of judges.The latter are tasked with selecting four final prize-winners, two from the open group and two from the trainee-only group. The final four shortlist will be posted publicly in a Twitter poll, at which time the general public can vote to determine the final ranking. The process, summarized by screening judge Dr.Elvira Gonzalez-Obeso, is shown in this image:
Summary of the process by which #PathTweetAward winners are selected.
-Sanjay Mukhopadhyay, MD is a Staff Pathologist at the Cleveland Clinic in Cleveland, OH. He is an expert thoracic pathologist,author of a lung pathology textbook, and a pioneer in the use of social media for teaching lung pathology globally, free of charge. Follow Dr. Mukhopadhyay on Twitter @smlungpathguy, and check out his freely accessible educational videos on YouTube.
Platelets are our first line of defense in controlling bleeding. Abnormally low numbers of platelets can lead to easy bruising, tiny leaks from capillaries into the skin and mucous membranes, causing petechiae, and bleeding. The platelet count is a significant parameter in the CBC and it is therefore vital to be able to report accurate and precise platelet counts. Furthermore, physicians must be able to use this information to diagnose the cause of the thrombocytopenia in order to recommend treatment.
What a platelet count alone cannot tell us is the reason for thrombocytopenia. Just as there can be many reasons for a low hemoglobin, and many causes for an increased or decreased WBC, there are numerous causes for a decreased platelet count. After ordering a CBC, the next steps in determining etiology of thrombocytopenia have historically been a thorough physical with attention to any bleeding symptoms and organ enlargements, and a medical history. The medical history should include family history, and notation of recent viruses or drug therapies. After these tests, a bone marrow aspirate and biopsy may also be necessary to clarify etiology. While modern, automated hematology analyzers produce reliable platelet counts, measuring only the circulating platelet count does not give us any information as to the etiology, so there is a need for further testing. With thrombocytopenia, platelet counts can be less reliable than with normal counts.Platelet counts were originally performed by impedance methods, then better accuracy and precision was obtained with optical platelet counts. Physicians rely on precision with very low platelet counts to make informed decisions about when to transfuse patients. The problem with the impedance counts at the low end, is that RBC fragments, schistocytes and microcytic RBCs can be counted as platelets, giving a falsely high count. On the other hand, measuring platelets by size can miss large platelets leading to a falsely low count.
Historically, the mean platelet volume (MPV) has been used along with the platelet count to aid in making a differential diagnosis. The MPV is analogous to the red cell distribution width (RDW) for red cells, and can be used to as an indicator of the maturity of platelets. Young platelets are the largest, and as they age, the size decreases. The normal ranges for MPV are generally about 9-12 femtoliters (fl).The MPV will be higher if more platelets are being released from the bone marrow, and lower if fewer are being newly released and we are counting mature platelets. Thus, the MPV can be used as an indirect marker for platelet production. However, an inherent problem with the MPV is that, similarly to the impedance platelet count, this count can be unreliable because any RBC fragments or particles may interfere with the measurement.
So, what is a physician to do?And how can the lab provide information to help them make the best differential diagnosis and transfusion decisions? In an effort to provide a parameter that could help differentiate causes of thrombocytopenia, the concept of reticulated platelet counts (retPLT) was first introduced in research in the late 1960s. The term is used to describe immature, functional platelets in the peripheral blood.Reticulated platelets are to mature platelets as reticulocytes are to mature red blood cells. These are the youngest platelets, within 24 hours of being released from the bone marrow. Reticulated platelets are large, with increased amounts of RNA, and the number in the circulation can be used to provide an estimate of the rate of thrombopoiesis. Originally, these were stained with new methylene blue and manual counts were done, much like a manual reticulocyte count; tedious,and imprecise. It wasn’t until about 30 years later that a flow cytometry method was described for measuring retPLT. Using traditional flow cytometry, reticulated platelets can be stained with a Thiazole Orange dye and passed through a flow cytometer. This method, however, has been shown to have wide normal ranges from 1-15% because of the lack of analytical standardization. Variations in the concentration of the thiazole dye used, the timing, and the gate settings all make it difficult to compare results obtained from one laboratory to another. In addition, flow cytometry is time consuming, labor intensive and costly.
Newer flow cytometry methods are now available on select hematology analyzers. There are currently 2 companies that have analyzers that can report retPLT using routine CBC reagents and controls. Reticulated platelets can be measured with the same K2 EDTA tube used for the CBC. The test is automated, simple to perform, fast, and gives standardized results with tighter normal ranges. The Abbott CELL-DYN Sapphire measures the retPLT using a fluorescent dye and flow cytometry with 2 dimensional gating. Sysmex XE and XN analyzers offer several Advanced Clinical Parameters including measures of reticulated platelets, expressedas the Immature Platelet Fraction (IPF%) and the Absolute Immature Platelet Fraction Count (IPF#). Sysmex offers a fluorescent platelet count (PLT-F) as an addition to impedance counting (PLT-I) and optical counting (PLT-O). PLT-F is more reliable because it uses a platelet specific dye which eliminates noninterference seen with other methods. The fluorescent dye labels the RNA and forward scatter is used to determine size while fluorescence is used to measure RNA content. With gating set based on cell volume and RNA content, the PLT-Fcan be measured. When there is an abnormal scattergram or a low platelet count,the PLT-F is reflexed and the IPF% and IPF# are also reported.
What’s the clinical utility of the IPF? Thrombocytopenia can have many causes.Immature platelets are functioning platelets, and an increased IPF means that we have more newly formed immature platelets circulating. The IPF helps physicians to differentiate thrombocytopenia caused by platelet destruction or consumption versus thrombocytopenia caused by deficient platelet production in bone marrow failure. It is vital to know the pathogenesis of thrombocytopenia in making decisions about treatment. With these advanced parameters, these decisions can often be made without costly, time consuming flow cytometry,without an invasive bone marrow biopsy and without waiting for the results of such biopsy. This can often save a patient an unnecessary platelet transfusion.
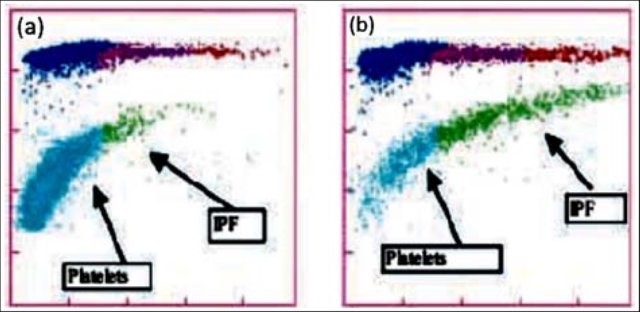
The reference range for IPF% in healthy individuals is1.0-7.0%. Together with a low platelet count, an increased IPF indicates an increase in platelet production. This is seen in patients with excessive destruction of platelets. An example of the clinical utility of the IPF can be seen in the diagnosis of immune thrombocytopenic purpura (ITP). ITP is an autoimmune bleeding disorder in which the immune system makes anti-platelet antibodies which destroy platelets. Acute forms occur more often in children while adults can have chronic ITP. ITP can be diagnosed on clinical findings but laboratory confirmation is often necessary. This can be expensive with long turnaround times using traditional flow cytometry and/or bone marrow aspirates.An IPF reported with a CBC is fast, inexpensive, and be extremely beneficial in aiding a timely diagnosis. Patients with ITP have been shown to have the consistently highest IPF values with ranges from 7-28%.1 As their platelet counts recover, the IPF% returns to the normal range, without the need for transfusions. Thus, the IPF can be used not only to help diagnose but also as an indicator of remission.
Figure1. Platelet scattergrams from a healthy individual with a normal IPF (a) and a patient with a high IPF (b). Mature platelets appear as blue dots, green dots represent the IPF with increased cell volume and higher fluorescence intensity compared to mature platelets1
In contrast to what we see with ITP, thrombocytopenia with alow normal or decreased IPF indicates decreased bone marrow production of platelets. Patients with bone marrow failure are more likely to have bleeding episodes with low platelet counts and may need transfusion. Rapid differential diagnosis using the IPF can help physicians help these patients get early treatment.
IPF may also be a reliable indicator of bone marrow recovery. Traditionally, neutrophil counts have been used as an indicator of recovery after a bone marrow transplant. IPF can be used as an indicator of imminent platelet recovery. It has been shown that,post-transplant, the IPF% increases before the platelet count. In a study done with stem cell transplant patients, it was shown that the absolute neutrophil count took an average of 13 days to recover, compared to 9 days for the IPF. The IPF was shown to recover before the Immature reticulocyte count, platelet count and absolute neutrophil count, giving physicians earlier indication that the transplant was successful.2 This is significant because it can eliminate the need for bone marrow biopsies and platelet transfusions.
Thrombocytopenia is not an uncommon finding in neonates, particularly in the neonatal intensive care unit (NICU). There are various causes for this, including sepsis, placental insufficiency and immune thrombocytopenia. The IPF% and IPF# can be used to diagnose and distinguish the cause of thrombocytopenia in neonates, and direct the treatment. When platelet count platelet count drops below 50 x 103/Lin an otherwise healthy appearing infant in the first 72 hours of life, neonatal alloimmune thrombocytopenia (NAIT) can be suspected. This condition is similar in pathogenesis to hemolytic disease of the fetus and newborn (HDFN), and is caused by an incompatibility in human platelet antigens between mother and baby. This occurs most often when the mother is HPA-1b and the father and baby are HPA-1a. The mother forms anti-HPA-1a which crosses the placenta and destroys the fetus’ platelets.This is a thrombocytopenia caused by platelet destruction, and the IPF% is high. The condition is self-limiting and resolves in 1-4 weeks. Neonatal sepsis can also present with a high IPF, but typically is found in very sick or premature babies and the degree of thrombocytopenia is not as severe as with NAIT. In contrast, neonatal thrombocytopenia due to placental insufficiency would exhibit a decreased IPF due to a deficiency in platelet production. Using the IPF% and IPF# to help differentiate the causes of neonatal thrombocytopenia can help steer the treatment and save infants from unnecessary invasive procedures and transfusions.
TheIPF has proved to be very valuable in the clinical setting. It has been used in the investigation of etiology in secondary thrombocytopenias due to chronichepatitis C, liver disease and HIV. It has been used to guide treatment in thrombocytopenias such as thrombotic thrombocytopenic purpura (TTP). IPF can also be useful in evaluation of hereditary platelet thrombocytopenias. The IPF% and IPF# can be compared after transfusion to support the theory that, after platelet transfusion, theIPF% will decrease due to the newly increased platelet count, but the IPF#remains the same. This validates that the IPF is a reflection of continual platelet production by the bone marrow.4
IPF%and IPF# are expanded CBC parameters that physicians can use to aid in differentiation of various thrombocytopenic states. Treatment for the different classes of thrombocytopenia can differ drastically, and knowing the class of thrombocytopenia helps direct the management. The IPF parameters are automated,easy to perform at the same time as the CBC, and provide standardized results that are inexpensive and available 24 hours a day in the hospital setting. Using the IPF can also reduce diagnostic costs for the patient. Many studies have been conducted on the varied applications of the IPF and research continues investigating possible further uses of this advanced clinical parameter. This is the new hematology, constantly providing the clinician with better tools for making diagnoses and treating patients. Platelet counts alone and MPVs are out. Make room for the new kid on the block; the IPF is in.
References
Arshi Naz et al. Importance of Immatureplatelet Fraction as a predictor of immune thrombocytopenic purpura. Pak J MedSci 2016 Vol 32 No 3:575-579
Zucker ML et al. Immature Platelet fraction asa predictor of platelet recovery following hematopoietic progenitor celltransplanatation. Lab Hematol 2006 12(3):125-30
Briggs,C. Assessment of an immature plateletfraction (IPF) in peripheral thrombocytopenia. Br J Haematol 2004Jul;126(1):93-9
Sysmex White Paper. The role of the ImmaturePlatelet Fraction(IPF) in the differential diagnosis of thrombocytopenia. www.sysmex.com/us
Fujii,T et al.. A new approach to detectreticulated platelets stained with thiazole orange in thrombocytopenicpatients. Thromb Res. 2000 Mar 15;97(6):431-40
Cremer Malte The immature platelet fraction(IPF) in neonates. Diagnostic Perspectives 2011 Vol1:36-42
Cremer M. et al. Immature platelet values indicateimpaired megakaryopoietic activity in neonatal early-onset thrombocytopenia.Thrombosis and Haemostasis 2010; May;103(5):1016-21
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A young adult female presents to an urgent care clinic with the chief complaint of a “bump and surrounding redness” on her right medial thigh. The patient reports the bump had been present without change for 1 year. Approximately 2 days prior to presenting at the urgent care clinic the patient states she nicked the bump while shaving, and subsequently the bump became tender with surrounding erythema and produced purulent drainage. The patient denies any similar prior lesions and denies any significant past medical history. On physical exam, the lesion measured 1 cm with the surrounding erythema measuring 5cm. The urgent care physician performed an incision and drainage and noted a scant amount of white purulent material within the lesion. A cyst wall was identified and was removed as much as possible. A swab of the purulent material was collected and submitted to microbiology for culture.
Laboratory Identification
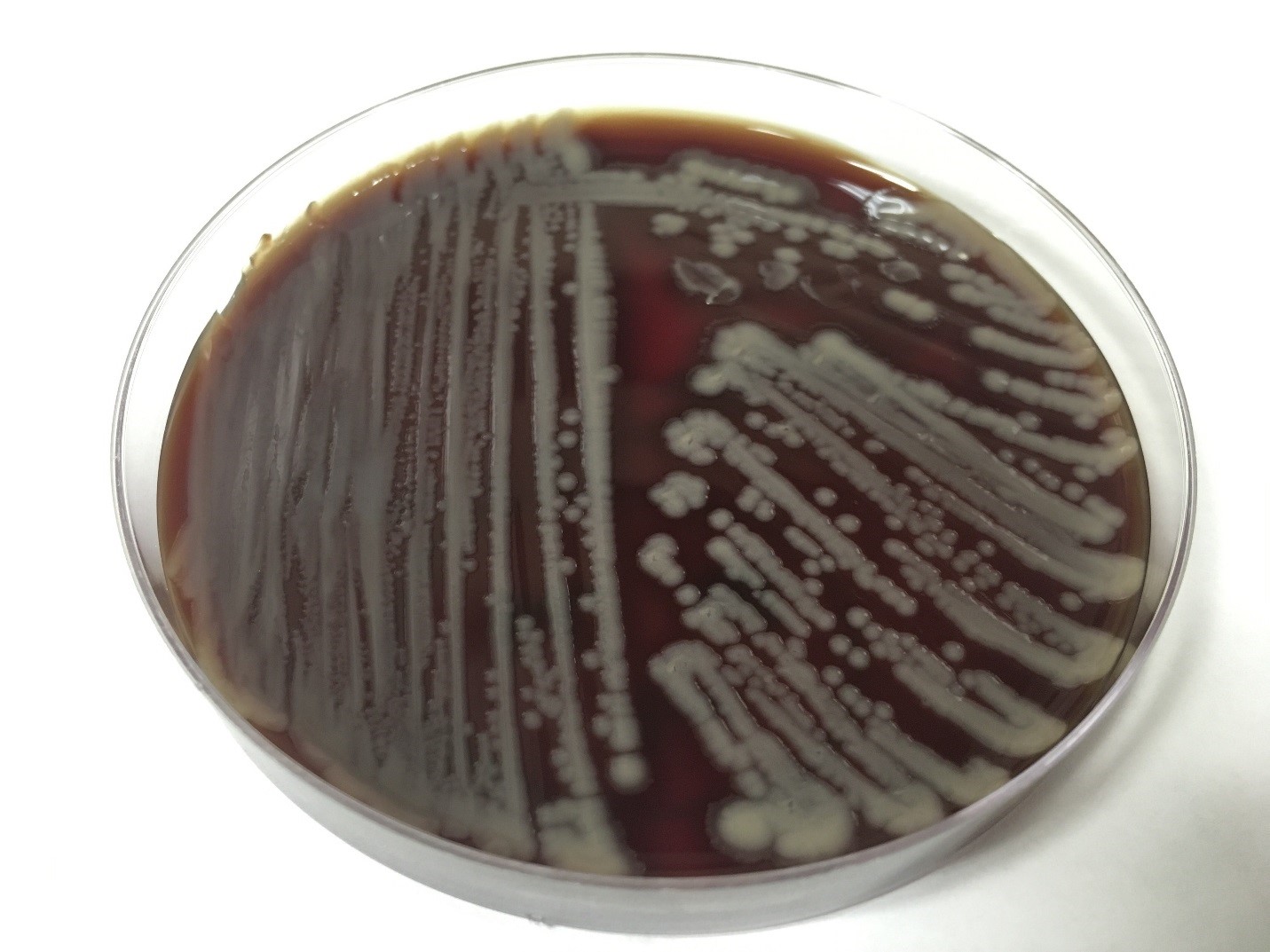
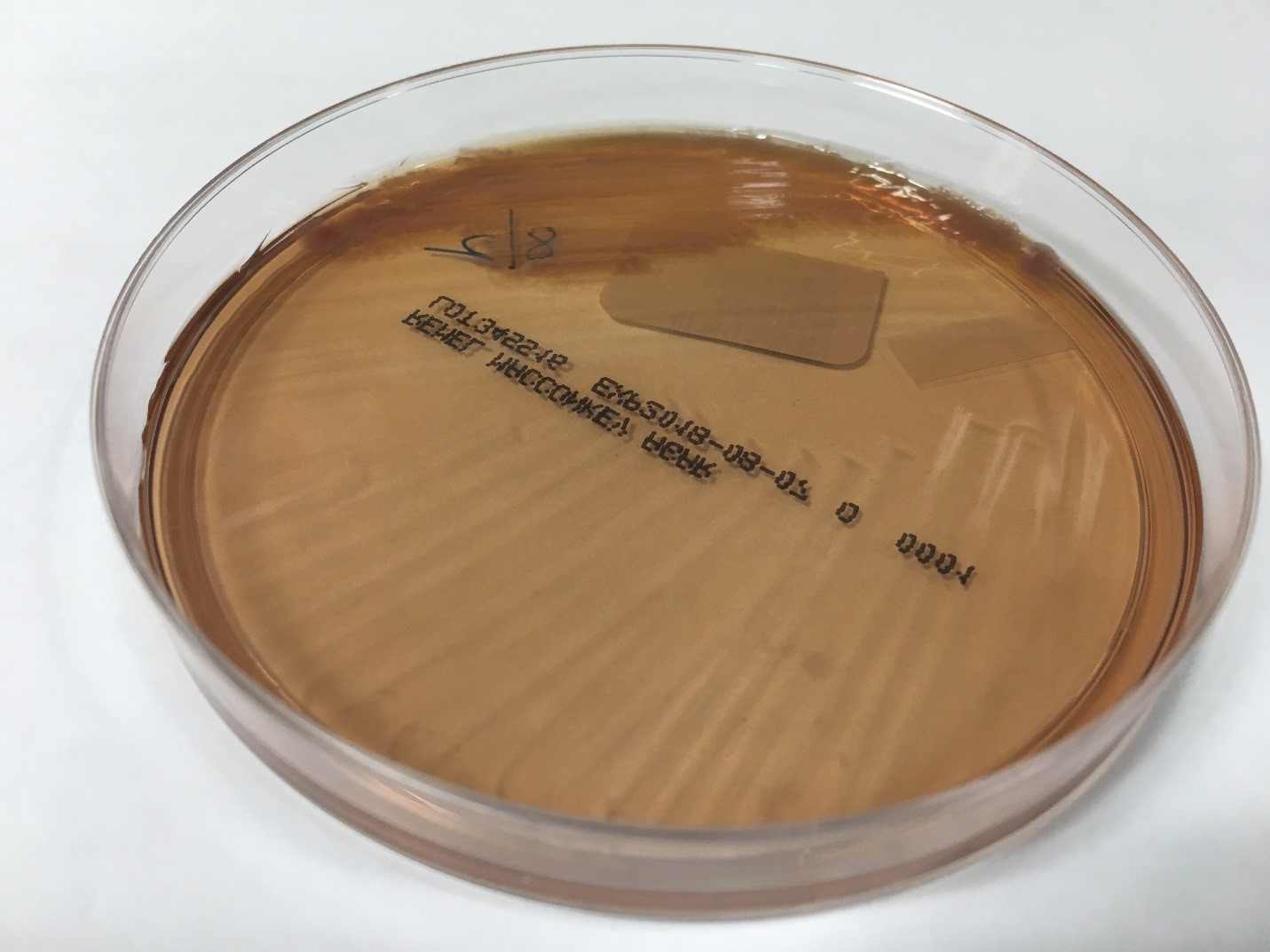
The primary gram smear of the swab specimen was interpreted as no bacteria or polys seen. Routine culture media including blood, chocolate, MacConkey, and CNA agar were inoculated and incubated aerobically. Following incubation, the blood agar showed few gram positive cocci consistent with usual skin flora and few single morphology of medium to large sized gray colonies without hemolysis. On the MacConkey agar, few single morphology non-lactose fermenting colonies were identified. The gray colonies identified on the blood agar gram stained as gram negative bacilli with unremarkable morphology. An oxidase test was performed and the bacteria was found to be oxidase positive. The key biochemical and physiologic characteristics of the isolate included: good growth on thiosulfate citrate bile salts and sucrose (TCBS) agar with yellow colonies, good growth in 6% NaCl nutrient broth, and no growth in 0% NaCl nutrient broth. The organism was identified by matrix-assisted laser desorption/ionization time of flight (MALDI-TOF) as Vibrio alginolyticus.
Image 1. Blood agar isolate of medium sized gray colonies.
Image 2. MacConkey agar with non-lactose fermenting colonies.
Discussion
Vibrio spp. are water organisms commonly found in marine or brackish water environments. These organisms are gram negative bacilli which classically have “comma” shaped morphology on gram smear, though this is not an absolute. On sheep blood agar, these organisms are variably beta hemolytic medium to large gray colonies and on MacConkey agar are non-lactose fermenting (with the exception of Vibrio vulnificus). Vibrio spp. are oxidase positive, ferment glucose, and readily grow on most isolation media with growth being enhanced with the addition of 1% NaCl to the media. The growth characteristics on media containing different concentrations of NaCl can be used in differentiating the different Vibrio spp. Thiosulfate Citrate Bile Salts and Sucrose (TCBS) agar is both selective and differential for Vibrio spp. with sucrose fermentation being detected as yellow colony formation.
Vibrio angiolyticus typically causes extraintestinal infections, with wound infections and otitis externa being the most frequent. Transmission frequently occurs via traumatic aquatic injuries in contaminated water. Vibrio angiolyticus rarely causes intestinal disease and is isolated in less than 5% of stool cultures in patients with Vibrio associated diarrhea. Growth characteristics of Vibrio alginolyticus include yellow colonies on TCBS due to its ability to ferment sucrose and good growth on 6% NaCl and no growth on 0% NaCl. Additional key biochemical characteristics of Vibrio alginolyticus include oxidase positivity, nitrite positivity, negative for myo-Inositol fermentation, negative for arginine dihydrolase, positive for lysine decarboxylase, and variable positivity for ornithine decarboxylase. Most wound infections due to Vibrio alginolyticus are non-severe, and most mild infections will clear without antibiotic therapy.
References
Procop GW, Koneman EW. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology, North American Edition. LWW; 2016.
Morris, J., Calderwodd, S., and Bloom, A. Minor Vibrio and Vibrio-like species associated with human disease. In: UpToDate, Post, TW (Ed), UpToDate, Waltham, MA, 2017.
-Justin Rueckert, DO is a 3nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
While Maria was working in Microbiology, she cut her finger while pulling reports off of the printer. It was a minor paper cut, so she ignored it, put her gloves on and continued her work back on the bench. A week later, the tiny cut was swollen and red. She decided to report the incident to her manager since it wasn’t healing. The manager asked Maria to report to the Occupational Health department, but was unsure if any treatment would be covered since the incident was not reported while she was at work.
Steve and Josh were bored during the night shift and they created a ball made from rubber bands to toss around. When Josh didn’t catch the ball, it hit the open tray of formaldehyde on the gross bench, and it splashed into Josh’s eye. He rinsed his eyes in the eyewash station for a couple of minutes, but both men were afraid to report the incident for fear of getting in trouble. Josh’s eye irritation continued to worsen, and he had to go to the eye doctor for treatment.
There are obvious consequences for injuries that occur in the laboratory, and reporting them is important for many reasons. Staff may be motivated in some instances to not report, but that creates problems for the individual, the department, for the facility, and even for other labs across the country! That may seem like a stretch, but it will become clearer with exploration.
The value in injury and accident reporting starts with medical follow-up. Those incidents which require treatment or abatement of infection can and should be dealt with quickly, and appropriate monitoring can be done if necessary. Some injuries may require immediate first aid, and a trip to the emergency department may even be necessary. Not reporting those types of injuries can be very dangerous for staff. Other incidents may require physician office visits or other monitoring, and employees who need it should be encouraged to comply.
In many work places the injury follow-up visits and treatment are covered financially by the institution, either via a structured occupational health program or through reimbursement. Some organizations may not offer financial coverage, however, if the incident that occurred at work is not reported as soon as possible. That reporting delay can raise suspicion as to whether or not the injury actually did occur while on the job, and since the written reporting protocol was not followed, there may also be no obligation for employer medical coverage.
Departmental issues will arise when incident reporting in not part of the overall lab safety culture. Sometimes there can be reprisals for unsafe behaviors which lead to accidents, but if the safety culture is good and if managers and employees coach against such practices, then there should be fewer overall incidents to report. That said, a culture of secrecy regarding injuries or exposures can also be dangerous. There is value in talking to all staff about an incident that occurred within the department. Staff can learn from the event and have a healthy discussion about how to keep it from reoccurring. A discussion of events can bring important safety issues to light, particularly if similar incidents happen with multiple people. This sharing of information can also promote awareness of good safety practices that can aid in the prevention of further incidents for all who work in the department.
OSHA requires the reporting of certain work place injuries, those that may have led to time away from work or that need medical follow up, for example. This injury data is compiled and reported nation-wide. It becomes a good source for benchmark data, a way to be able to compare your lab injury rates with others across the country. The U.S. Bureau of Labor Statistics provides this data as information labs can use. One way to utilize the information is to see if the number of reportable injuries you are seeing in your lab is comparable to a national average. That assessment can give you a starting point in determining whether or not your lab’s safety incidents are at typical levels. Of course, lab safety professionals want to see zero injuries, but if you see your lab injury numbers are very high compared to benchmark data, you can begin to see where to focus in on fixes for the lab physical environment or on creating specific safety training.
There is great value in talking about safety incidents that may result in injury or exposure in the lab setting. These “safety stories” raise awareness of safety issues, and they can act as a deterrent for repeat incidents. Create a culture where staff feel free and comfortable to report incidents, and be sure to discuss them with all staff, and record reportable injuries as well. Having reliable national data also provides helpful information to other labs, and better information can help to improve safety in laboratories everywhere!
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Recently, a new technology has become available for screening the esophagus for early detection of at-risk patients for cancer. Esophageal cancer has one of the highest mortality rates. Watch this interview with Rob Odze, a pathologist who works with the technology, and learn more about how this could impact the practice of clinicians, pathologists, and laboratory professionals involved in upper endoscopy services.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
For patients with gender dysphoria, the Endocrine Society has endorsed the use of hormone therapy to promote secondary sexual characteristics of the desired gender. These guidelines were first established in 2007 and revised last year, and gave the first evidence guided recommendations for clinicians treating transgender patients.
For transgender males, testosterone by itself is prescribed as an injectable oil-based solution. These doses are given as intramuscular injections- usually into the thigh. If that’s too painful, subcutaneous injections have been shown to have similar efficacy. The doses given to transgender males is much higher (50-100mg/ injection) than that given to men with testosterone deficiency (30-50 mg/ injection). Primarily because the men have more testosterone to start with. Also, whereas topical testosterone gel may be sufficient for men with “low T,” it doesn’t seem to provide enough testosterone to transgender males and is quite expensive, so it is generally not used.
Image 1. Picture of testosterone cypionate vial from mcguffmedical.com. This is used for intramuscular injections.
Upon starting testosterone injections, the frequency of injections is every one to two weeks. However, the onset of physical secondary sexual characteristics takes 3-6 months to begin. After about 3 years, most of the changes to occur will have manifested. These physical changes are outlined in the table below. You’ll notice how certain traits like cessation of menses and fat redistribution start within the first 6 months whereas muscle growth and voice change take effect after 6 months. Also, the time certain effects take maximal effect varies; the voice doesn’t deepen further after 2 years, but hair growth continues to increase through 5 years.
Physical Effect
Begins
Maximal Effect
Facial/body hair growth
6-12 mo
4-5y
Skin oiliness/acne
1-6mo
1-2y
Scalp hair loss
6-12 mo
–
Increased muscle mass
6-12 mo
2-5y
Fat redistribution
1-6mo
2-5y
Cessation of menses
1-6mo
–
Deepening of voice
6-12 mo
1-2y
Table 1. Timeframe of physical traits that manifest in transgender males while taking testosterone hormone therapy. Based on Hembree et al. 2017 (1).
Just as hormone therapy induces physical manifestations of secondary sexual characteristics for transgender men, we would suspect that internal aspects of physiology are affected too. Values measured by the laboratory provide meaningful insight into how our body and its different organ systems are functioning. Accordingly, the Endocrine Society also recommended laboratory monitoring of transgender patients starting hormone therapy.
Measure Testosterone and hemogoblin/ hematocrit every 3 months for the 1st year, then 1-2x/ year afterwards.
Monitor Lipids at regular intervals
Previous studies have monitoring these lab values found consistent increases in hemoglobin and hematocrit (2,3). This is due to the stimulation of erythropoiesis by testosterone (4). While excessive testosterone could lead to polycythemia (excessive RBCs in the blood), it is not a commonly described complication in transgender patients. Some summary results from our study for hemoglobin and hematocrit are shown in Figure 1A, which shows a clear shift in levels.
However, reports on lipids have been varied LDL and triglyceride changes (2,3). The only consistent finding was that HDL decreased in transgender males taking testosterone (2,3). In our study, we found triglycerides were increased with decreased HDL (Figure 1B). The take-away is that because cardiovascular cut-offs are based on risk and not a reference range, patients and clinicians will have to be aware of these possible metabolic changes.
Creatinine, when it was checked, increases for transgender males (5). We found creatinine was strongly increased in our study to become similar to baseline creatinine in transgender women before taking hormone therapy (Figure 1C). This topic as it relates to glomerular filtration rate is very complex and will be discussed further in a future post.
To illustrate lab value changes in transgender men, I’ll direct you to data that I found in a large study of over 300 transgender patients including about 80 transgender men. The completed manuscript is not currently available but will be printed soon:
However, this does not mean Cisgender male reference intervals are adequate for transgender men. This topic needs further exploration and ideally a prospective trial to be performed in a controlled manner. A double-blind study would not be possible as it would be unethical to perform.
References
Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. J Clin Endocrinol Metab. 2017
Wierkx K, et al. Cross-Sex Hormone Therapy in Trans Persons is Safe and Effective at Short-Time Follow-Up: Results from the European Network for the Investigation of Gender Incongruence. J Sex Med, 2014. 11(8):1999-2011.
Mueller A, Kiesswetter F, Binder H, Beckmann MW, Dittrich R. Longer-term administration of testosterone undecanoate every 3 months for testosterone supplementation in female-to-male transsexuals. J Clin Endocrinol Metab. 2007
Paller CJ, Shiels MS, Rohrmann S, Menke A, Rifai N, Nelson WG, et al. Association Between Sex Steroid Hormones and Hematocrit in a Nationally Representative Sample of Men. J Androl. 2012 33(6): 1332-1341.
Fernandez JD, Tannock LR. Metabolic Effects of Hormone Therapy in Transgender Patients. Endocr Pract. 2016;22:383–8.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
A 72 year old female with past medical history of stage IV ovarian adenocarcinoma treated with chemotherapy and interval debulking surgery, presented to emergency room with a one week history of confusion and worsening balance.
CT scan of the head showed new communicating hydrocephalus. A magnetic resonance imaging couldn’t be performed initially because of patient’s uncontrolled agitation. Lumbar puncture (LP) was performed. Following this procedure the patient’s mental status showed some improvement and therefore neurosurgery team decided to insert ventriculoperitoneal (VP) shunt to treat her hydrocephalus and prevent recurrence of seizures.
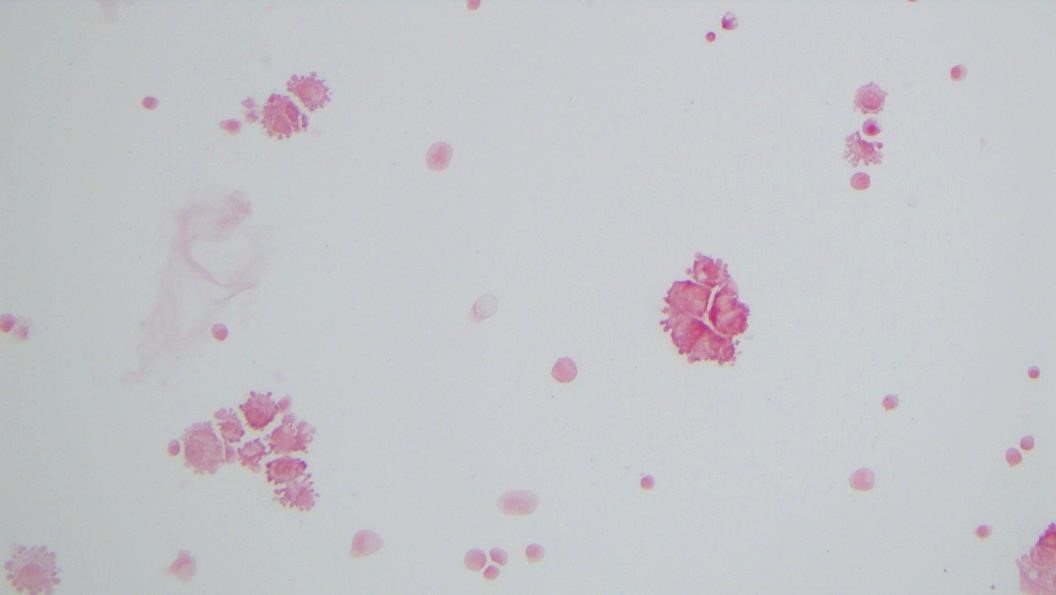
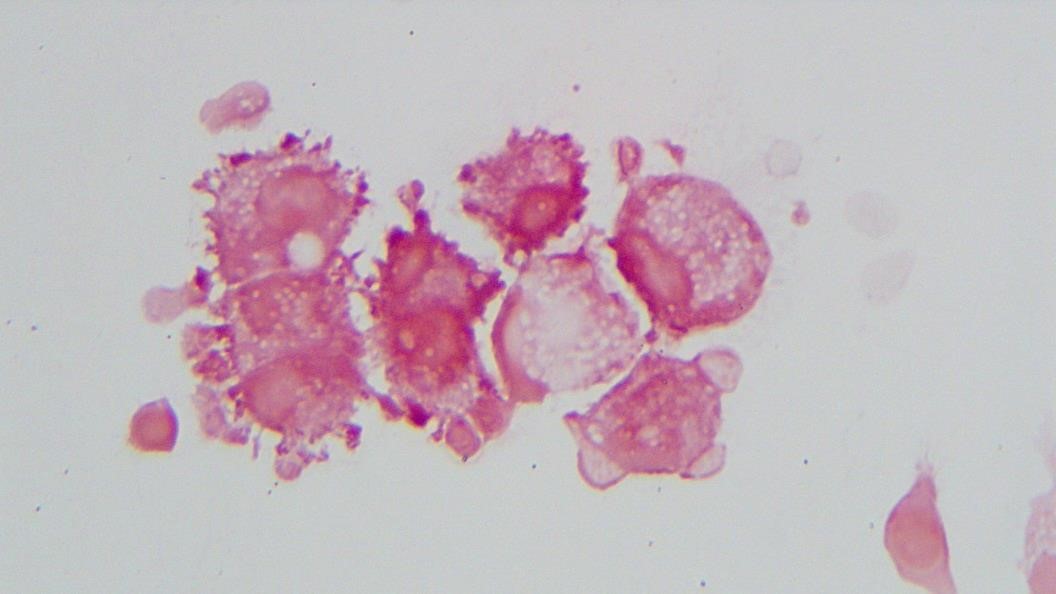
It was Friday afternoon when a microbiology technologist brought the patient’s cerebrospinal fluid (CSF) gram stain to be reviewed. It was confirmed that no inflammatory cells and organisms were present. However, cells in the background looked very atypical (Image 1a, b).
Image 1: Gram stain of CSF showing atypical epithelial cells at (a) 40x and (b) 100x with oil.
Image 1b.
Discussion
The gram stain is used to provide preliminary information about the microorganism present in the specimen. Gram stain differentiates bacteria into two fundamental varieties of cells. Bacteria that retain the initial crystal violet stain (purple) are said to be “Gram-positive,” whereas those that are decolorized and stain red with carbol fuchsin (or safranin) are said to be “Gram-negative” (1). An adequate examination of a gram-stained smear includes observing numerous representative fields and the fields containing neutrophils yield the most information (2). Gram stain provides information about number of bacteria present, gram reaction and shape of the bacteria. In background we can also see epithelial cells and inflammatory cells. However, it’s a good practice to also appreciate and investigate any odd looking findings.
To investigate further, we visited the hematology laboratory to view their CSF slide to determine if these cells were a processing artifact. After it was confirmed that hematopathology saw the same atypical cells, a cytopathologist was requested to review the gram stain since patient’s CSF cytology specimen was to be processed after the weekend. Cytopathologist favored our suspicion and decided to process the cytology specimen late in the day on Friday and it was confirmed that those atypical cells were consistent with the metastatic adenocarcinoma.
Neurosurgery team was immediately contacted to reconsider insertion of the VP shunt as the shunt would drain fluid from the CSF into the peritoneal cavity and thus there was concern for transferring of malignant cells from central nervous system into abdomen/pelvis. However, after consulting oncology team it was later decided to proceed with the procedure since patient’s primary tumor originated in abdomen/pelvis and current intraabdominal tumor burden was not significant as compared to the symptoms driven by CNS involvement. Proceeding with this procedure was considered to be palliative and the best course of action to improve the patient’s quality of life.
Barenfanger J, Drake C. Interpretation of gram stains for the nonmicrobiologist. 2001 July;32(7):368–375.
-Kiran Manjee, MD, is a 1st year anatomic and clinical pathology resident at University of Chicago (NorthShore).
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
A 56 year old male presented to his PCP complaining of sinus congestion, rhinorrhea, night sweats, decreased appetite and fevers of up to 101-102 every evening. Hematologic evaluation revealed a neutropenia and a lymphopenia. An infectious disease work up was negative. His LDH was elevated. Physical examination reveals an enlarged left axillary lymph node. An excisional biopsy was performed.
Biopsy Findings
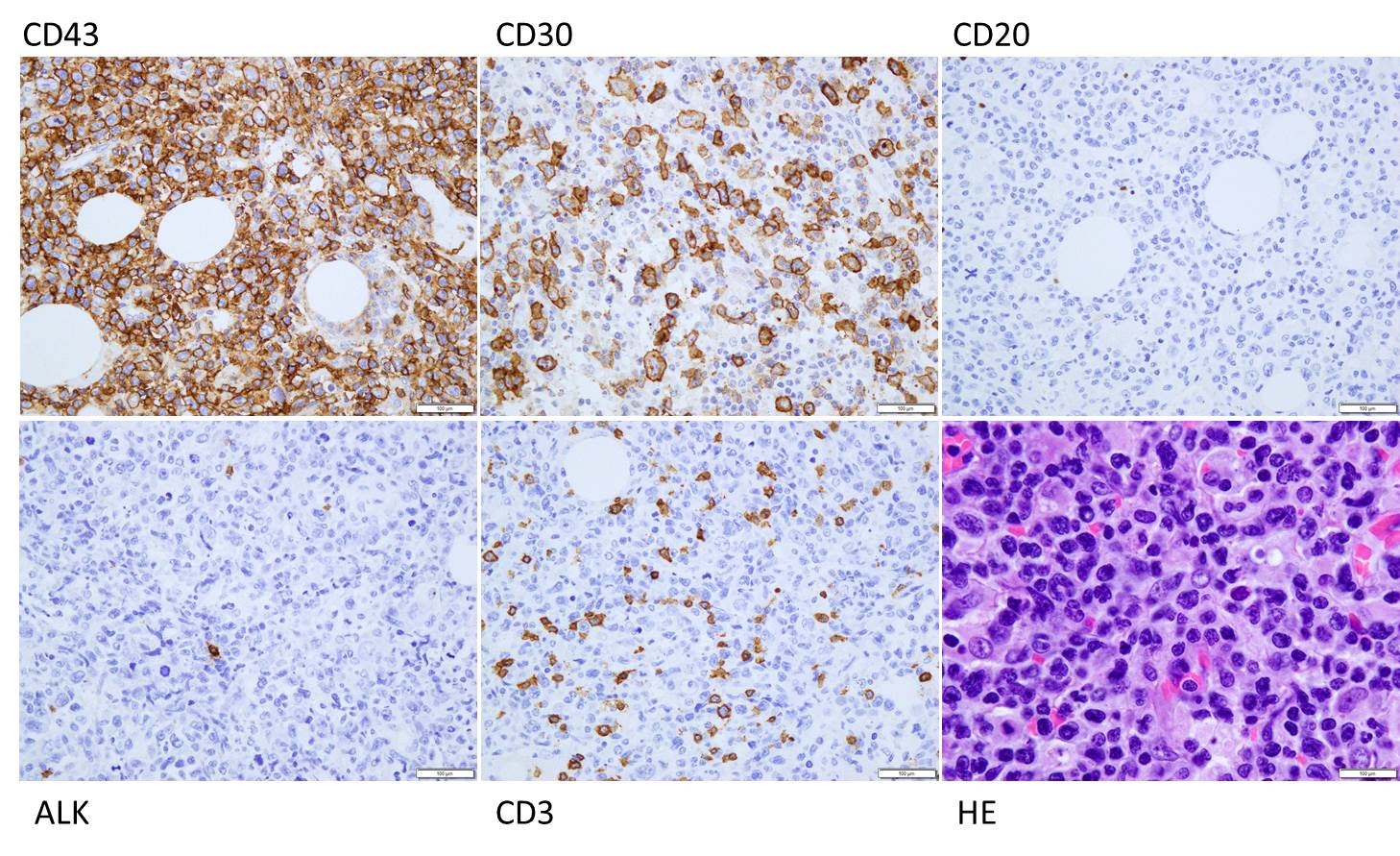
H&E stained sections demonstrate an enlarged node with effaced architecture and scattered residual follicles with small, mature cells. There is a proliferation of intermediate to large, to very large, atypical and highly pleomorphic cells many of which demonstrate bizarre forms, irregular nuclear morphology and acidophilic nucleoli. The lymphoma cells are noted to focally traverse through adipose tissue. Occasional hallmark cells are appreciated.
To further characterize the infiltrate, immunohistochemical stains were performed and interpreted with appropriate controls. The lymphoma cells were diffusely positive for CD45 (LCA), CD43, and CD30 (membranous and Golgi) with a Ki-67 of 80-90%. These cells were negative for CD20, PAX-5, CD3, CD4, CD8 (mostly), CD5, D10, BCl-2, BCl-6 and ALK1.
The morphologic features and immunophenotype of the cells was diagnostic of anaplastic large cell lymphoma, ALK negative.
Discussion
Anaplastic Large Cell Lymphoma (ALCL), ALK-negative (ALK-) is defined as a CD30+ T-cell neoplasm that morphologically resembles ALK-positive ALCL, but lacks ALK protein expression. It most commonly affects adults (aged 40-65 years), and has a slight male preponderance with a male-to-female ratio of 1.5:1. T. Most patients present with advanced disease (stage III-IV), lymphadenopathy and B symptoms. The most common differential diagnosis is ALK-positive ALCL.
The molecular deciphering of ALCL began in the 1990s with the discovery of a recurrent t(2;5) (p23;q35) translocation fusing the ALK gene and the nucleophosmin gene generating a NPM-ALK fusion protein, as well as other ALK translocations resulting in a high ALK kinase activity. This triggers the major oncogenic pathway in ALK-positive ALCL. Pharmacologic therapy has been developed to target ALK, and has shown efficacy. Thus, compared with ALK-negative cases, ALK-positive occurs in younger patients and has a better prognosis. ALK-negative ALCL also tends to involve both lymph nodes and extranodal tissues, although extranodal sites are less commonly involved than in ALK+ ALCL.
The other differential diagnoses of ALK- ALCL includes, primary cutaneous ALCL (C-ALCL), other subtypes of CD30+ T-cell or B-cell lymphoma with anaplastic features and classic Hodgkin Lymphoma. If a single lymph node or cutaneous cases are suggestive of ALK- ALCL, C-ALCL needs to be considered. Any cases that involve the gastrointestinal tract need to be distinguished from CD30+ enteropathy-associated and other intestinal T-cell lymphomas.
Molecular analysis of ALK- ALCL shows characteristic strong expression of CD30, in equal intensity in all the cells. Loss of T-cell markers is frequently seen, however, more than half of all cases express one or more T-cell markers. CD2 and CD3 are more commonly expressed than CD5, and CD43 is almost always expressed. CD4+ is frequently positive, while CD8+ is rare. Many cases also express cytotoxic markers TIA1, granzyme B, and/or perforin.
The genetic profile in ALK-negative ALCL has been found to be pretty heterogenous. Most notably, activating mutations of JAK1 and/or STAT3 have been shown to lead to activation of the JAK/STAT3 pathway. Chromosomal rearrangements of DUSP22 (i.e. chromosomal rearrangements in or near the DUSP22-IRF4 locus on 6p25.3) occur in 30% of the cases, and rearrangements of TP63 occur in about 8% of cases. Neither of the rearrangements have been reported in ALK+ ALCL.
From a prognostic standpoint, studies have shown that the rearrangements have effects on the survival rate. TP63-rearranged cases were shown to have an unfavorable prognosis worse than ALK- ALCL with neither rearrangement, while DUSP22-rearranged cases were shown to have favorable outcomes similar to ALK-positive ALCLs.
References
Gaulard P, de Leval L. ALK-negative anaplastic large-cell lymphoma. 2016 Jan 14;127(2):175-7.
Edgardo R. Parrilla Castellar et al., ALK-negative anaplastic large cell lymphoma is a genetically heterogeneous disease with widely disparate clinical outcomes Blood. 2014 Aug 28; 124(9): 1473–1480.
-Brandon Zelman is 4th year medical student at the Philadelphia College of Osteopathic Medicine and an aspiring pathologist. You can follow Brandon on Twitter @ZelmanBrandon.
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
A 64 year old man with metastatic colon cancer and a history of recent motor vehicle collision with polytrauma presented from a rehabilitation facility with fever up to 105 degrees Fahrenheit. Two months prior to admission he was hospitalized for the motor vehicle collision in which he sustained orthopedic injuries to multiple extremities. In addition to external fixation of several injuries, he returned to the operating room on multiple occasions for additional incision and drainage of a wrist wound which demonstrated gross purulence with cultures growing Enterococcus, Prevotella, and an extended spectrum beta-lactamase-producing Morganella morganii. Antimicrobial regimen initially consisted of surgically placed antibiotic beads and broad-spectrum therapy with vancomycin, piperacillin-tazobactam, and then meropenem. The patient was eventually transitioned to an oral antibiotic regimen consisting of linezolid and ciprofloxacin for an anticipated course of six weeks and he was discharged to a rehabilitation facility.
After several weeks at the rehabilitation facility, the patient became febrile and was admitted for workup of his fever. Initially the fever was of uncertain origin with malignancy (rectal cancer with metastasis to the liver), drug fever (linezolid), and wound site infection on the differential. Linezolid was discontinued, daptomycin initiated, and ciprofloxacin maintained. Fever persisted and ciprofloxacin was discontinued as another possible source of drug fever. Ertapenem was initiated. Initially, prior wounds and surgical sites appeared well-healing. Blood cultures all yielded no growth. However, on day five of this hospitalization, purulent drainage was noted from the site of a left leg surgical wound. Arthrocentesis yielded 0.5 mL of bloody fluid which was sent for cell count, differential, and culture.
Laboratory Findings
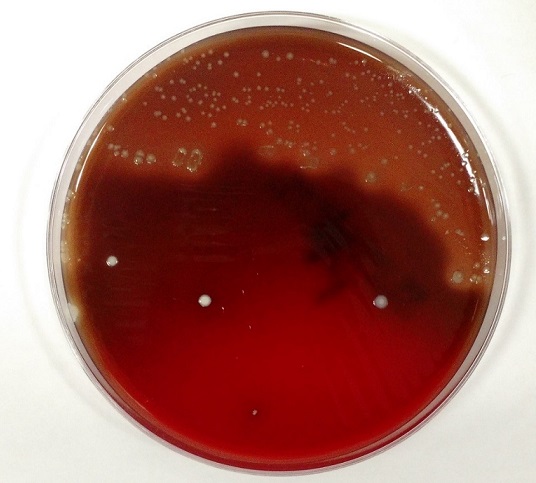
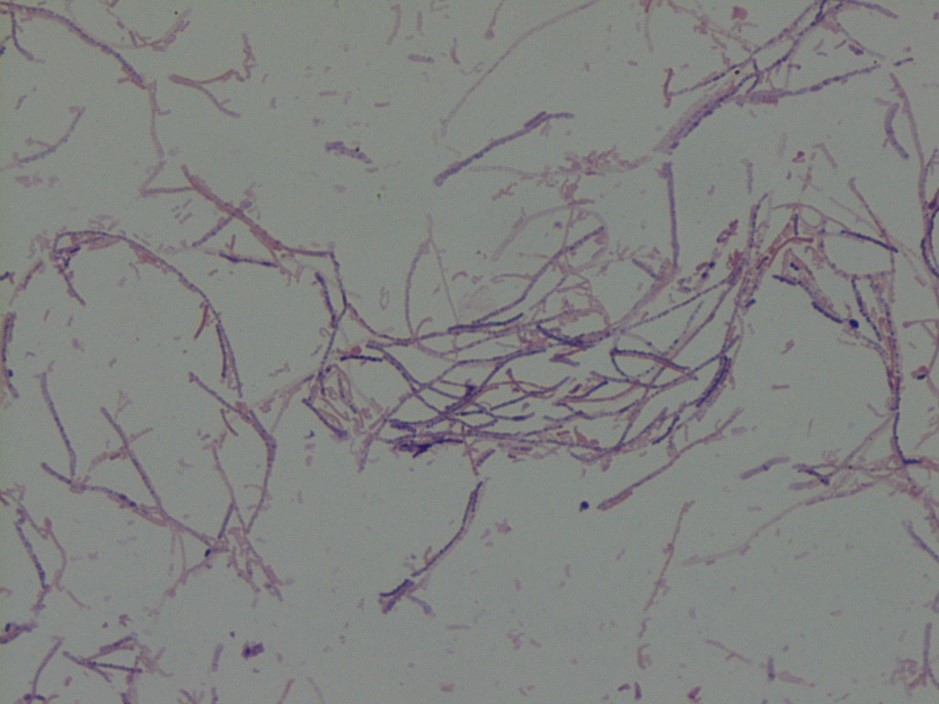
Initial Gram stain showed few polymorphonuclear leukocytes with no bacteria seen. Cell count was unable to be performed due to viscosity of the specimen but differential showed 80% neutrophils. There was no growth on aerobic blood, chocolate, or MacConkey agars. Anaerobic Schaedler (non-selective) agar grew 1-2 mm brownish colonies (Image 1). Gram stain of this isolate revealed gram variable bacilli forming long filaments (Image 2). The isolate was identified using MALDI-TOF MS (Vitek) as Clostridium ramosum.
Image 1. 1-2 mm brownish colonies on anaerobic Schaedler agar
The patient was taken to the operating room for incision and drainage of the left knee with two additional samples sent for culture which grew Clostridium ramosum.
Discussion
Clostridium species are anaerobic, spore-forming, gram positive bacilli. C. ramosum is non-motile and is normally found in the human colon and the environment. One study identified C. ramosum in the feces of 83% of sampled adults. Former names include Eubacterium filamentosum, Ramibacterium ramosum, Actinomyces ramosus, and Eubacterium ramosum. Figure 2 demonstrates a notable characteristic of C. ramosum, i.e. its variable appearance on Gram stain. The morphology here may be described as gram negative or “over-decolorized”, though gram positive bacilli are clearly seen forming many of the filaments. Its terminal endospores are often difficult to identify on Gram stain and this is true of Figure 2. These characteristics on Gram stain have historically made identification difficult, though use of MALDI-TOF MS facilitated identification in our case. Biochemically, C. ramosum ferments glucose and hydrolyzes esculin; it is negative for lecithinase and lipase.
C. ramosum possesses an IgA protease though it is not commonly pathogenic. When it is pathogenic, the spectrum of disease overlaps with that of other anaerobes and includes deep-seated abscesses, e.g. intra-abdominal abscess secondary to trauma. Osteomyelitis and primary bacteremia are also possible, particularly in immunocompromised patients. Otitis media in children is another possible clinical scenario.
Septic arthritis due to Clostridium ramosum
A 2016 case report described two cases of septic arthritis due to C. ramosum. In one case, a patient with rheumatoid arthritis on methotrexate and prednisone and history of revision knee arthroplasty eight years prior presented with knee swelling. Synovial fluid aspirate was consistent with an infectious process; the prosthesis was removed but synovial and intraoperative cultures were negative. Antimicrobial therapy with linezolid and ciprofloxacin was administered for six weeks with clinical improvement. Two weeks after discontinuation of antibiotics the patient became febrile. Blood cultures were negative but culture of synovial fluid grew C. ramosum. The patient required multiple operations due to joint destruction and was ultimately managed with intravenous penicillin and clindamycin with transition to oral metronidazole for three months of therapy. The second case of C. ramosum septic arthritis presented in this report was ultimately managed with surgical debridement and amoxicillin-clavulanate. Both cases presented in patients with immunocompromising comorbidities and the course of their septic arthritis was chronic, recurring, and destructive but non-fatal with both patients dying from other causes.
These clinical and laboratory characteristics are consistent with the case of C. ramosum septic arthritis identified at our institution. The case of septic arthritis presented here involved an immunocompromised host (malignancy) with history of trauma, foreign body placement (external fixator), and long-term antibiotic therapy. This patient’s wound required debridement in the operating room on three occasions. Once clinically stable, the patient was discharged to a subacute rehabilitation facility and continued on ertapenem with amoxicillin for an expected duration of six weeks with the plan to switch to amoxicillin-clavulanate and ciprofloxacin for suppressive therapy.
References
Forrester JD, Spain DA. Clostridium ramosum bacteremia: case report and literature review. Surg Infect (Larchmt). 2014 Jun;15(3):343-6. doi: 10.1089/sur.2012.240. Epub 2013 Nov 27. Review. PubMed PMID: 24283763.
García-Jiménez A, Prim N, Crusi X, Benito N. Septic arthritis due to Clostridium ramosum. Semin Arthritis Rheum. 2016 Apr;45(5):617-20. doi: 10.1016/j.semarthrit.2015.09.009. Epub 2015 Oct 1. PubMed PMID: 26546506.
Procop, Gary W et al. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Seventh ed., 2017.
-Benjamin F. Smith is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.