Case History
A 64 year old man with metastatic colon cancer and a history of recent motor vehicle collision with polytrauma presented from a rehabilitation facility with fever up to 105 degrees Fahrenheit. Two months prior to admission he was hospitalized for the motor vehicle collision in which he sustained orthopedic injuries to multiple extremities. In addition to external fixation of several injuries, he returned to the operating room on multiple occasions for additional incision and drainage of a wrist wound which demonstrated gross purulence with cultures growing Enterococcus, Prevotella, and an extended spectrum beta-lactamase-producing Morganella morganii. Antimicrobial regimen initially consisted of surgically placed antibiotic beads and broad-spectrum therapy with vancomycin, piperacillin-tazobactam, and then meropenem. The patient was eventually transitioned to an oral antibiotic regimen consisting of linezolid and ciprofloxacin for an anticipated course of six weeks and he was discharged to a rehabilitation facility.
After several weeks at the rehabilitation facility, the patient became febrile and was admitted for workup of his fever. Initially the fever was of uncertain origin with malignancy (rectal cancer with metastasis to the liver), drug fever (linezolid), and wound site infection on the differential. Linezolid was discontinued, daptomycin initiated, and ciprofloxacin maintained. Fever persisted and ciprofloxacin was discontinued as another possible source of drug fever. Ertapenem was initiated. Initially, prior wounds and surgical sites appeared well-healing. Blood cultures all yielded no growth. However, on day five of this hospitalization, purulent drainage was noted from the site of a left leg surgical wound. Arthrocentesis yielded 0.5 mL of bloody fluid which was sent for cell count, differential, and culture.
Laboratory Findings
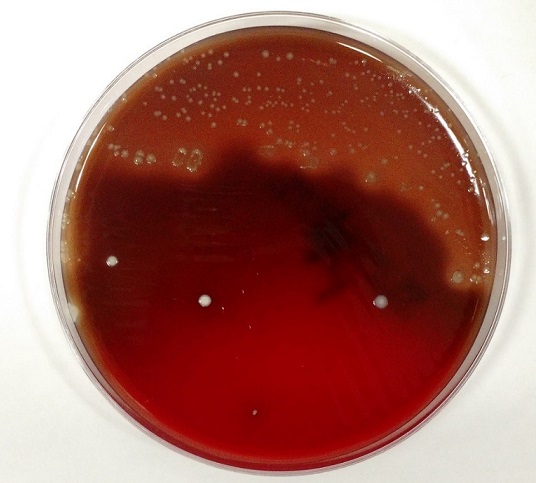
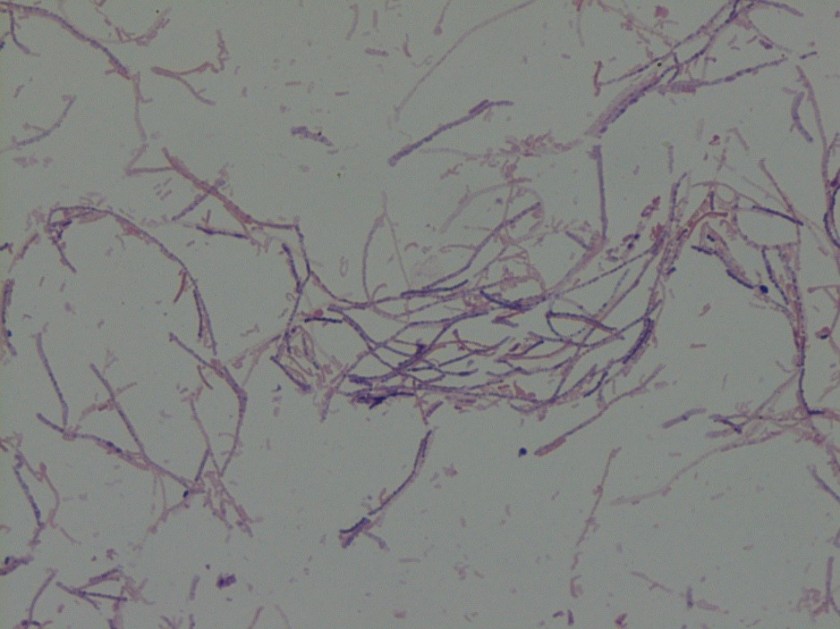
Initial Gram stain showed few polymorphonuclear leukocytes with no bacteria seen. Cell count was unable to be performed due to viscosity of the specimen but differential showed 80% neutrophils. There was no growth on aerobic blood, chocolate, or MacConkey agars. Anaerobic Schaedler (non-selective) agar grew 1-2 mm brownish colonies (Image 1). Gram stain of this isolate revealed gram variable bacilli forming long filaments (Image 2). The isolate was identified using MALDI-TOF MS (Vitek) as Clostridium ramosum.
The patient was taken to the operating room for incision and drainage of the left knee with two additional samples sent for culture which grew Clostridium ramosum.
Discussion
Clostridium species are anaerobic, spore-forming, gram positive bacilli. C. ramosum is non-motile and is normally found in the human colon and the environment. One study identified C. ramosum in the feces of 83% of sampled adults. Former names include Eubacterium filamentosum, Ramibacterium ramosum, Actinomyces ramosus, and Eubacterium ramosum. Figure 2 demonstrates a notable characteristic of C. ramosum, i.e. its variable appearance on Gram stain. The morphology here may be described as gram negative or “over-decolorized”, though gram positive bacilli are clearly seen forming many of the filaments. Its terminal endospores are often difficult to identify on Gram stain and this is true of Figure 2. These characteristics on Gram stain have historically made identification difficult, though use of MALDI-TOF MS facilitated identification in our case. Biochemically, C. ramosum ferments glucose and hydrolyzes esculin; it is negative for lecithinase and lipase.
C. ramosum possesses an IgA protease though it is not commonly pathogenic. When it is pathogenic, the spectrum of disease overlaps with that of other anaerobes and includes deep-seated abscesses, e.g. intra-abdominal abscess secondary to trauma. Osteomyelitis and primary bacteremia are also possible, particularly in immunocompromised patients. Otitis media in children is another possible clinical scenario.
Septic arthritis due to Clostridium ramosum
A 2016 case report described two cases of septic arthritis due to C. ramosum. In one case, a patient with rheumatoid arthritis on methotrexate and prednisone and history of revision knee arthroplasty eight years prior presented with knee swelling. Synovial fluid aspirate was consistent with an infectious process; the prosthesis was removed but synovial and intraoperative cultures were negative. Antimicrobial therapy with linezolid and ciprofloxacin was administered for six weeks with clinical improvement. Two weeks after discontinuation of antibiotics the patient became febrile. Blood cultures were negative but culture of synovial fluid grew C. ramosum. The patient required multiple operations due to joint destruction and was ultimately managed with intravenous penicillin and clindamycin with transition to oral metronidazole for three months of therapy. The second case of C. ramosum septic arthritis presented in this report was ultimately managed with surgical debridement and amoxicillin-clavulanate. Both cases presented in patients with immunocompromising comorbidities and the course of their septic arthritis was chronic, recurring, and destructive but non-fatal with both patients dying from other causes.
These clinical and laboratory characteristics are consistent with the case of C. ramosum septic arthritis identified at our institution. The case of septic arthritis presented here involved an immunocompromised host (malignancy) with history of trauma, foreign body placement (external fixator), and long-term antibiotic therapy. This patient’s wound required debridement in the operating room on three occasions. Once clinically stable, the patient was discharged to a subacute rehabilitation facility and continued on ertapenem with amoxicillin for an expected duration of six weeks with the plan to switch to amoxicillin-clavulanate and ciprofloxacin for suppressive therapy.
References
- Forrester JD, Spain DA. Clostridium ramosum bacteremia: case report and literature review. Surg Infect (Larchmt). 2014 Jun;15(3):343-6. doi: 10.1089/sur.2012.240. Epub 2013 Nov 27. Review. PubMed PMID: 24283763.
- García-Jiménez A, Prim N, Crusi X, Benito N. Septic arthritis due to Clostridium ramosum. Semin Arthritis Rheum. 2016 Apr;45(5):617-20. doi: 10.1016/j.semarthrit.2015.09.009. Epub 2015 Oct 1. PubMed PMID: 26546506.
- Procop, Gary W et al. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Seventh ed., 2017.
-Benjamin F. Smith is a Pathology Student Fellow at University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
