Cigarette smoking can affect both innate and adaptive immunity, and introduces concerns when evaluating a patient’s eligibility for surgery. It has been shown to hinder time required for healing and long-term survival of patients. It can promote vascular complications, increase the rates of hepatocellular carcinoma and reduce lung function.1 For lung transplantation, one of the common requirements of eligibility is smoking abstinence for at least 6 months. Smoking post-surgery is associated with worse outcomes for the patients including complications and higher rates of mortality.2 Relapse to smoking post lung transplantation has been reported to range from 11% to 23% in various patient populations.3 As a result, clinical testing for cigarette smoking abstinence is an important part of initial workup and follow-up of transplant patients.
In some situations, the burden of lung allocation weighs heavily on a single clinical laboratory result that is perceived to definitively confirm or exclude active cigarette smoking. This subsequently factors into the decision by the physicians to deem the patient eligible to receive a lung transplant. The perception of nicotine testing as definitive proof of smoking is misleading and does not reflect the complexity of situations that can lead to a positive test result.
How can we assess smoking?
Ideally, many factors should weigh into the final smoking status determination including self-reporting (used historically), witnesses to behavior, odor, and past history including cessation attempts. Clinical laboratory testing is important and thought to be more reliable means for smoking assessment. It can involve testing for nicotine (originating from tobacco or nicotine replacement therapy, NRT) and its metabolites: cotinine, 3-hydroxycotinine (3-OH-cotinine), and nornicotine. Moreover, nicotine contains a number of alkaloids that are not usually present in nicotine-replacement therapies (NRTs) including anatabine and anabasine.4 Nicotine testing can involve a combination of metabolites such as cotinine as well as alkaloids like anabasine. Various sample types have been used including saliva, blood and urine.5 In addition, measurements of the exhaled carbon monoxide (CO) have been used to assess recent smoking status (within the last 8 hours).6
Clinical case: patient with detectable nicotine metabolites
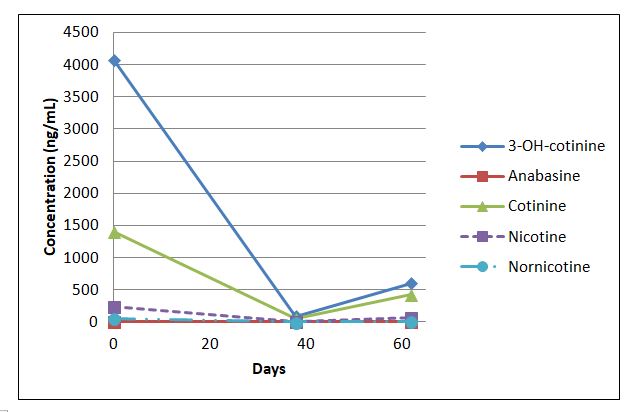
A case involving a patient being considered for lung transplantation was received by our department. The patient had been tested for anabasine, nicotine, and its metabolites in urine. Testing of random urine specimens was performed by liquid chromatography tandem mass spectrometry (LC-MS/MS) at different time points from samples collected during hospital visits (days 0, 38, and 62). The urine contained variable concentrations of nicotine and its metabolites, with anabasine concentrations below the detection limit in 2 out of the 3 testing instances. Testing at day 0 showed an interfering substance that prevented the determination of accurate anabasine concentration. The nicotine and its metabolite concentrations in the random urine specimens were lower from day 0 to day 38, but a noticeable increase of 3-OH-cotinine and cotinine concentrations was observed in the specimen collected on day 62. The physician was seeking information about the current smoking status of the patient and was planning to use this information to determine the patient’s lung transplant eligibility.
| Days | 0 | 38 | 62 |
| Analyte concentration (ng/mL) | |||
| 3-OH-cotinine | 4074 | 89 | 603 |
| Anabasine | interf. subst. | < 3 | < 3 |
| Cotinine | 1404 | 47 | 425 |
| Nicotine | 241 | < 2 | 72 |
| Nornicotine | 58 | < 2 | 6 |
Figure and table 1. Nicotine, metabolite and anabasine concentrations (ng/mL) at different time points for a patient evaluated for lung transplantation eligibility. Anabasine was not detected on days 38 and 62, with an interfering substance preventing quantitation on day 0.
How definitive are these results?
No information was available regarding self-reported smoking or NRT use history for this patient. The physician had high suspicion that the patient was an active smoker and was attempting to use higher concentrations of nicotine and metabolites observed on day 62 as evidence of recent tobacco use.
For cotinine, values can range from 20-550 ng/mL for daily tobacco use.5 Nicotine concentrations in urine can approach over 5000 ng/mL with daily use. Together, high nicotine and cotinine can support tobacco or high-dose nicotine patch use. Furthermore, presence of nornicotine above 30 ng/mL along with anabasine greater than 10 ng/mL would be consistent with current tobacco use rather than NRT.7
Given that these were random urine specimen and the urinary creatinine values are not routinely measured, it’s important to consider the possible contributions of the variable urine concentration to the analyte concentrations. It has previously been reported that individuals abstaining from smoking for at least two weeks should present with nicotine of <30 ng/mL, cotinine of < 23 ng/mL, 3-OH-cotinine of <120 ng/mL, nornicotine < 3 ng/mL, and anabasine of < 2 ng/mL in urine.7 Based on these cut-offs, all analytes except anabasine would suggest new nicotine intake within the last two weeks.
In general, a positive anabasine result, in combination with the presence of nicotine metabolites, is consistent with active use of a tobacco product, whereas anabasine values of < 2ng/mL may suggest that NRT is the likely source.8 This can imply that the patient is abstinent from smoked or chewed tobacco if anabasine is not detected. However, anabasine is not a sensitive marker of smoked tobacco. It has been reported that the compound may not be detectable in 60% of self-reported smokers (N=51; 3 ng/mL cut-off in urine)9 and its urinary concentrations do not correlate well with self-reported tobacco use.8
As a result, anabasine has low sensitivity for determining eligibility for UNOS (United network for organ sharing) listing. There are some recommendations that this marker should not be used alone. Given that other alkaloids can originate from tobacco plant, it has been proposed that anatabine should be added to analysis due to higher expected concentration.9 However, this alkaloid is not completely specific to tobacco as it has been proposed to also arise from other plant sources 10,11 leading to possible implications for the patient that may be misclassified. In addition, anatabine sensitivity in detecting smoked tobacco use varies depending on the tobacco source and the clinical cut-off used. Clinical tests that include anatabine are not routinely available.
Can we improve this process?
Unfortunately, there is no definitive marker distinguishing smoking from NRT.
The determination of smoking status has advanced from reliance on self-reporting to quantitative and specific measurements of metabolites of nicotine and minor components of tobacco. Additional analyte incorporation into a test panel leads to additional complexities and considerations in interpretation of the results. Therefore, it is important to educate the physicians about various nicotine sources causing a positive nicotine and/or metabolite test result including NRT or e-cigarettes. It is also important to convey the limitations of tobacco alkaloid testing in such scenarios. Both the lab and the physician need to be cautious about implying active smoking in the absence of indirect supporting evidence and/or positive clinical test results.
At the same time, there is a need to improve the utility and availability of other tobacco alkaloid testing in distinguishing cigarette smoking from NRT in specific transplant populations and consider the value of testing alternative specimens. This may lead to a more effective implementation of secondary markers of tobacco use.
References
- Qiu, F.; Fan, P.; Nie, G. D.; Liu, H.; Liang, C.-L.; Yu, W.; Dai, Z., Effects of Cigarette Smoking on Transplant Survival: Extending or Shortening It? Frontiers in Immunology 2017, 8, 127.
- Zmeskal, M.; Kralikova, E.; Kurcova, I.; Pafko, P.; Lischke, R.; Fila, L.; Valentova Bartakova, L.; Fraser, K., Continued Smoking in Lung Transplant Patients: A Cross Sectional Survey. Zdravstveno varstvo 2016, 55 (1), 29-35.
- Vos, R.; De Vusser, K.; Schaevers, V.; Schoonis, A.; Lemaigre, V.; Dobbels, F.; Desmet, K.; Vanaudenaerde, B. M.; Van Raemdonck, D. E.; Dupont, L. J.; Verleden, G. M., Smoking resumption after lung transplantation: a sobering truth. The European respiratory journal 2010, 35 (6), 1411-3.
- Hukkanen, J.; Jacob, P., 3rd; Benowitz, N. L., Metabolism and disposition kinetics of nicotine. Pharmacological reviews 2005, 57 (1), 79-115.
- Raja, M.; Garg, A.; Yadav, P.; Jha, K.; Handa, S., Diagnostic Methods for Detection of Cotinine Level in Tobacco Users: A Review. Journal of clinical and diagnostic research : JCDR 2016, 10 (3), Ze04-6.
- Sandberg, A.; Skold, C. M.; Grunewald, J.; Eklund, A.; Wheelock, A. M., Assessing recent smoking status by measuring exhaled carbon monoxide levels. PloS one 2011, 6 (12), e28864.
- Moyer, T. P.; Charlson, J. R.; Enger, R. J.; Dale, L. C.; Ebbert, J. O.; Schroeder, D. R.; Hurt, R. D., Simultaneous analysis of nicotine, nicotine metabolites, and tobacco alkaloids in serum or urine by tandem mass spectrometry, with clinically relevant metabolic profiles. Clinical chemistry 2002, 48 (9), 1460-71.
- Jacob, P., 3rd; Hatsukami, D.; Severson, H.; Hall, S.; Yu, L.; Benowitz, N. L., Anabasine and anatabine as biomarkers for tobacco use during nicotine replacement therapy. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 2002, 11 (12), 1668-73.
- Feldhammer, M.; Ritchie, J. C., Anabasine Is a Poor Marker for Determining Smoking Status of Transplant Patients. Clinical chemistry 2017, 63 (2), 604-606.
- Lanier, R. K.; Gibson, K. D.; Cohen, A. E.; Varga, M., Effects of dietary supplementation with the solanaceae plant alkaloid anatabine on joint pain and stiffness: results from an internet-based survey study. Clinical medicine insights. Arthritis and musculoskeletal disorders 2013, 6, 73-84.
- von Weymarn, L. B.; Thomson, N. M.; Donny, E. C.; Hatsukami, D. K.; Murphy, S. E., Quantitation of the minor tobacco alkaloids nornicotine, anatabine, and anabasine in smokers’ urine by high throughput liquid chromatography mass spectrometry. Chemical research in toxicology 2016, 29 (3), 390-397.

-Dr. Valentinas Gruzdys developed interest in clinical chemistry early in his academic training which led him to pursue and obtain a PhD in Clinical and Bioanalytical Chemistry at Cleveland State University. Valentinas is enthusiastic about teaching and helping improve the understanding of limitations and utility of clinical laboratory testing. He is currently enrolled in a clinical chemistry fellowship program at the University of Utah. He enjoys learning more about various aspects of clinical chemistry and cannot wait to make his own contributions to the field after his training.