Hello everyone. Back again!
This time, I’ve got something to talk about that’s a little more serious. I don’t like to deviate from fun lab-related memes and insights,but every now and then something really strikes a chord. Enough so to talk to all of you about it. Some of you reached out to me after my post discussing clinician burnout and suicide in healthcare and that felt great; connecting with people who had some powerful stories to share really validated that conversation. Today, I want to talk about guns. Specifically, the public health epidemic of gun violence, the current conversation about whose “lane” (read:responsibility) belongs to whom, and what role those of us in laboratory medicine play.
I was horrified to see the recent shooting and murder of three in my Chicago home at Mercy hospital in the Near South Side. I won’t rehash the details that are on the news. Emergency resident physician Dr.Tamara O’Neal, newly minted Chicago Police Officer Samuel Jimenez, and pharmacy resident Dayna Less were all shot and killed point-blank by a gunman in the Mercy Hospital emergency department. A place that is supposed to be for healing, safety, and hope. Senseless.

This now presses the start button on America’s newest tradition: a very short-lived, ill-timed, and often tone-deaf debate about the firearm subculture in our nation. Okay, bias check: you should know that I am not a fan of guns of any kind. If it were up to me, they would either belong in museums or find more useful lives melted and repurposed as metal used to reinforce hurricane-prone buildings or safe hypodermic needles for patients in need. That said, this isn’t a gun debate article; nor is it an open forum to discuss gun control, the second amendment, the NRA, or anything political. I respect opinions and educated civil discourse, but this piece today is focused on health—public health.
The epidemic of gun violence in America is a problem. The American Public Health Association (APHA) posted on their website extensively on the topic of gun related deaths which “kill more than 38,000 people and cause nearly 85,000 injuries each year. As a longtime advocate for violence prevention policies, APHA recognizes a comprehensive public health approach to addressing this growing crisis is necessary.” (Read their fact sheet here)Furthermore, the American College of Physicians (ACP) published a position paper on the topic in the Annals of Internal Medicine journal (read it here)where they establish a comprehensive set of recommendation from a conglomerate of clinical medical specialty organizations. Increasingly now more than ever does this prevalence of gun related injury and death present itself as a major health concern: a public health epidemic. I could talk to you about the number of mass shootings in our country, or the epidemiologic incidence of gun-related deaths compared to other countries, even the policy discussion around gun ownership and regional policies regarding safety and gun control—it doesn’t matter. All the charts and graphs any recycled article on the subject will just fade into the mist of “yet another shooting.” That’s not okay. I don’t want to drown you in data. Better put, I can’t. See, the problem is you’ll see the same pieces of information regarding the gun debate as you scroll through the news on your social media. Something new I want to add to this conversation is the overwhelming emphasis on the simple truth that this is a public health issue.

This unfortunate new reality is no different from other public health programs that have addressed various issues over the past decades. What do deaths from motor vehicle accidents, fires, smoking-related ung cancer, obesity and type 2 diabetes, heart attacks, antibiotic resistant bacterial infections, and traumatic brain injuries have in common? Per the American Foundation for Firearm Injury Reduction in Medicine (AFFIRM), they were all public health crises that pushed medicine past a breaking point in clinical burden and forced us to invest in research which conclusively provided results to address related mortality and morbidity. AFFIRM is a non-profit organization which is building a coalition in medicine for the purpose of researching and addressing this newest public health issue. They argue that,without medical evidence we won’t be able to find solutions to the senseless loss of life from gun violence. Death from car accidents gave us the seatbelt and tickets for disobeying its required legal usage. Death in home fires got us the smoke detector and regulations surrounding their installation. Lung cancer deaths led to smoking cessation programs, increased taxation, and policy changes regarding access to cigarettes. Sugar-related morbidities created a conversation about healthy diets, public policies addressing food deserts, and taxation programs for drinks with added sugar. Heart attack deaths gave us longitudinal studies for best care practices and lifestyle recommendations.Resistant bugs established a new discussion on antimicrobial stewardship. Brain injuries gave us new guidelines for concussions. I could go on. That’s only the tip of the public health iceberg. The point is that if there is an epidemiological trend where people are literally dying, data married with health metric-oriented research create solutions!
But let’s add deaths from gun violence to that list. What then do they all have in common, besides the concern for improving public health? Save for the tragically evident lack of a solution, the similarity becomes clear: there is lobby, interest, power, and support. Cars didn’t always have seat belts, cigarettes used to be cheap and doctors used to smoke at work,no one talked about cheeseburgers giving you heart attacks and diabetes decades ago, and helmet-clashing football players didn’t always receive the treatment they needed. Why? Because some entity—corporate, societal, etc.—wasn’t keen on“buying in.” Much like it takes justification and convincing for administration to buy your fancy chemistry analyzer, so do the public and oppositional lobby groups which require swaying toward the intervention(s) being proposed.

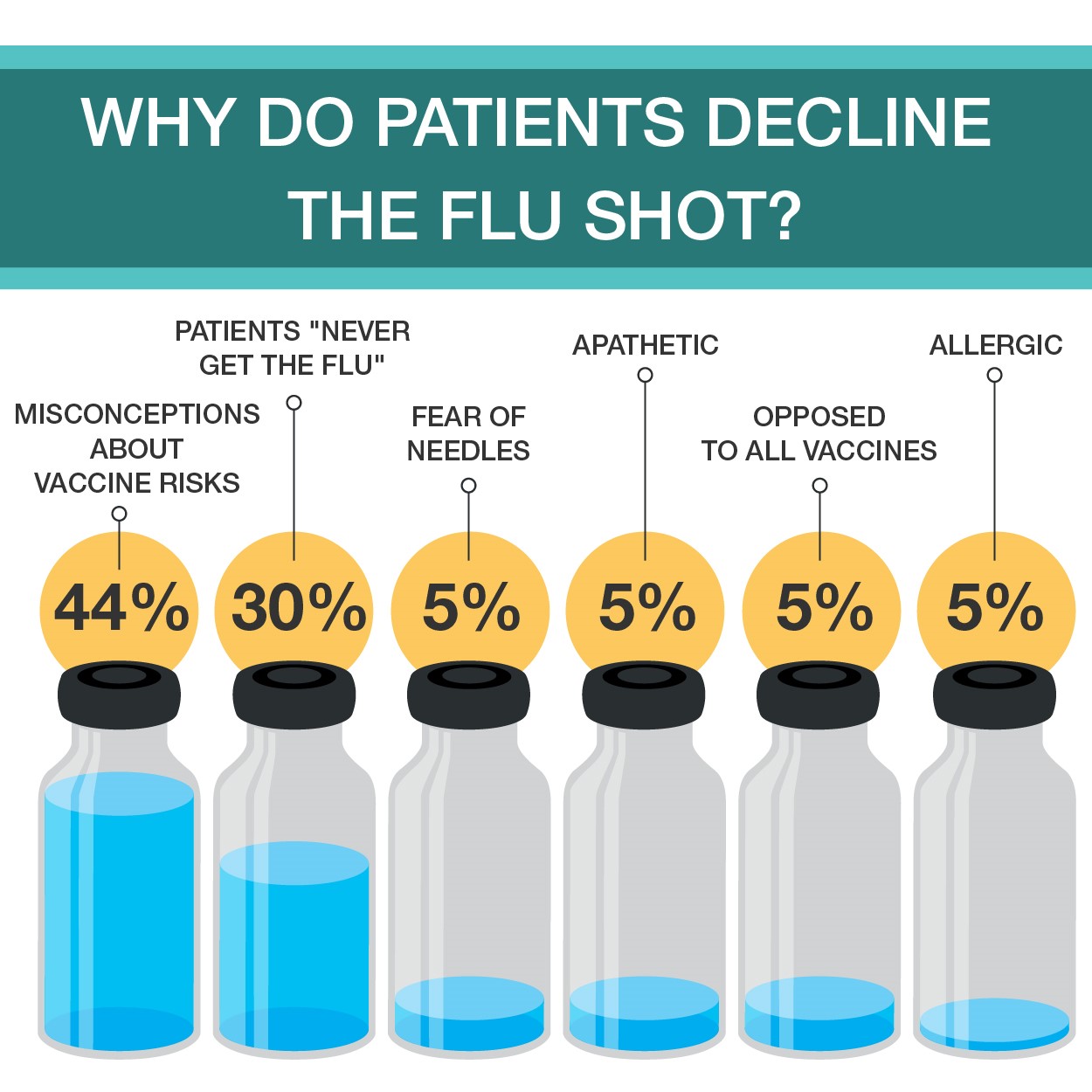
Often, the data stacks high enough to influence decisions on its own. But that isn’t the case with gun related mortality. I see gun related violence as sort of the opposite of the vaccine debate: with the flu shot there seems to be too much data and not enough stories to convince the anti-vax movement to realize the significant threat being addressed. On the other hand, gun related violence exhibits far too many stories without any significant amounts of data. Possibly, this might be related to the limitations placed upon the CDC since the mid-1990’s that forbid them from using funds “to advocate or promote gun control.” Yes, really. Just last month, I wrote about the newest advancements in influenza testing and the best practice of vaccinating annually.I cited thousands of deaths related to vaccine-preventable or epidemiologic illness; 80,000 dead from influenza last year, thousands from swine flu over a decade ago, etc. But when you try and cite proper, medical data regarding guns in public health, its … not so easy. No data, no research. No research, no change.
Many of you have undoubtedly read about the current social media “discussion” regarding whose “lane” gun violence is to navigate: The National Rifle Association (NRA) asserted in a tweet that doctors, discussing the issue only within their field should leave it to more “qualified” groups like them. That’s been a tinder box of vitriol the medical community, for lack of a better term, is up in arms about. I followed and read tons of comments about this as it unfolded, hearing from endless doctors, nurses, and laboratorians posting with blood spattered scrubs, decimated trauma bays, and emptied blood bank refrigerators that this growing epidemic is enraging clinicians about. Earlier, I highlighted similarities between public health problems and their respective solutions citing that they all shared oppositional lobby groups. What better profession to handle the topic in question than medicine—whose associated lobby power from professional societies like ours to Big Pharma amass one of the largest voices in policy making in America. And another thing, as gun violence is a public health concern, whose literal job is it to address health, mortality, and morbidity? All of ours. Nurse educators lead patients through lifestyle modifications they can employ to curtail some effects of diabetes, physicians manage patient treatment regimens balancing input from pharmaceutical tools to professional guidelines,clinicians like us strive to provide the best resources available by advancing hemoglobin A1c levels or point of care testing. We all play roles in every single healthcare matter that translates to life or death, so why not this one?
So, I touched on it a little here, but what role does the medical laboratory professional play? Besides bullets in tissue section, how does the public health epidemic of gun violence reach the lab? I wasn’t so sure, until I read a story about Dr. Julie Melinek, a forensic pathologist with UC Davis and the Alameda County Sheriff’s Department. In response to the NRA’s“stay in your lane” tweet regarding gun deaths, Dr. Melinek tweeted “Do you have any idea how many bullets I pull out of corpses weekly? This isn’t my lane. It’s my [expletive] highway.” She proceeded to turn her phone off and work for a few hours. When she returned, things were viral. In an interview with Medscape, she discussed this story and the topic at large with editor-in-chief Dr. Eric Topol. She talked about the epidemiologic role clinicians of all specialties play in risk assessment and harm reduction,saying “…if we see something that’s dangerous for the pediatric population,like a toy that breaks apart or is a choking hazard, we report it to the Consumer Product Safety Commission and it gets recalled because it’s a hazard.”She and Dr. Topol explored the ways clinicians can advocate for patients and public health at large, concluding with some poignant words, encouraging those of us in medicine to reach out to elected officials. The internet facilitates such an easy way to communicate, she says that it becomes paramount to voice the opinions held within the medical community to those in policy-making; especially clinicians who may own guns or be active NRA members! Because, ultimately, this isn’t about gun ownership or second amendment rights—its about the health, well-being, and safety of our patients.
Dr. Melinek represents a single voice within the pathology community. You’ve read my posts about lab management values, interdisciplinary team work, attainable goals, and utilization of data to make clinical decisions. Those of us in lab medicine find ourselves at the forefront of translating data into decisions. When quality control measures on instrumentation fail to correct after countless interventions, do we continue running assays? No! We work-up and investigate what root cause is the problem and fix that if possible; thinking outside the box, looking at lesser-than-obvious causes, investigating all possible solutions, etc. In pathology we’re the first to implement new, highly advanced tests and corroborate with other specialties about what the new changes mean for patient care and management of diseases (i.e. 5thgeneration high-sensitivity troponins and evolving to a new standard of care for acute coronary syndromes). We’re also the first to notice trends that impact patient outcomes and the first to provide solutions: think back to the last time you spent a few minutes reading your labs metrics and goals posted somewhere at work. Dr. Melinek collecting bullets from her autopsy patients is no different than forensic pathologists historically noting trends in mortality statistics, iatrogenic, environmental, and other causes of death.And, when those trends get published and presented, they call for further research and investment into public health interventions that may prevent those deaths in the first place. Pathology, public health, epidemiology, and laboratory medicine are built for this. We’re the tangible bridge between what gets discovered and what gets researched. We’re also in a privileged position to have a bird’s eye view of a larger clinical, epidemiologic picture as pathologists see populations of patients.
In a recent Lablogatory post, ASCP’s Lotte Mulder (ASCP Leadership Institute and Patient Champions programs) wrote about Moral Capacity, Courage, and Resiliency. Specifically, she said “It is not enough to understand and recognize a moral dilemma, it is important to act on it… it is critical for leaders to understand that culture influences moral and ethical behavior.” If America’s gun violence problem is one that desperately needs data, then why shouldn’t we, then, be professional and cultural leaders and advocate through data collection, analysis, and translation like we always do? Let’s use our tools and our talent for lab medicine, in partnership with the growing coalition of clinical professional specialties, and cultural humility for the populations we protect, and address this once and for all.
Thank you.

–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.