A 23 year old man presented to the hospital with recurrent fever up to 103F with associated nausea and vomiting, epistaxis, watery diarrhea, dyspnea, and decreased appetite for several days. Blood cultures from admission were positive for MSSA and a stool PCR was positive for Vibrio species. He was admitted and treated for sepsis. His CBC demonstrated a marked pancytopenia ( WBC count 0.6 K/μL) and the hematopathology team was consulted to review the peripheral blood film.
Peripheral blood smear.
Review of the peripheral blood confirmed a markedly pancytopenic picture with virtually no leukocytes in the region of best RBC “spread” (Image 1A). In the periphery of the smear (1B and C) clusters of leukocytes were noted where left-shifted granulocytes were seen. Many demonstrated nuclear irregularity and abnormal granulation (B) and some showed the presence of numerous Auer rods (Image 1C, arrows).
The presence of abnormally granulated immature neutrophilic precursors, and cells with numerous Auer rods was morphologically compatible with acute promyelocytic leukemia (APL) and a rush preliminary diagnosis was rendered. The patient was started on ATRA therapy and FISH for PML-RARA was expedited.
Discussion
Acute promyelocyticleukemia (APL) is characterized as an acute myeloid leukemia in which promyelocytes with the PML-RARA fusion predominate. The PML-RARA fusion is the result of a balanced translocation between chromosomes 15 and 17, designated ast (15;17)(q24.1;q21.2). The promyelocyte progenitor cell is the cell of origin of APL. APL occurs most frequently in middle aged individuals, but can occur at any age.
The first account of APL was originally discussed in the late 1950s in which L. K.Hillestad, a hematologist from Norway, described a disorder as “a white blood cell picture dominated by promyelocytes and severe bleeding caused mainly by fibrinolysis.” The gene fusion was elucidated in the late 1970s at the University of Chicago demonstrating the balanced translocation between chromosomes 15 and 17. Cure rates at that time were still very low, until in the mid 1980s when researchers in China demonstrated the use of all-trans retinoic acid causing complete remission in APL patients.
Two distinct subtypes of APL exist: hypergranular (typical) or microgranular. The hypergranular variant is filled with large Auer rods and with dense cytoplasmic granules that can obstruct the nucleus. In contrast, the microgranular variant has a scantiness of cytoplasmic granules or small azurophilic granules.
The immunophenotype for APL is quite distinct and characterized by low or absent expression of CD34 and HLA-DR (in keeping with the cellular differentiation from blast to promyelocyte). APL cells are positive CD33 and CD13 with most cases showing expression of CD117 (sometimes weak). APL cells are usually negative for CD15, CD65, CD11a, CD11b, and CD18. The microgranular variant may display positive staining for CD34 and CD2. For both variants, IHC with antibodies to the PML gene demonstrates a nuclear multi granular pattern with nucleolar exclusion, a finding that is unique to APL and not seen in AML or normal promyelocyte morphology.
The main clinical symptom of APL is hemorrhagic, including gingival bleeding and ecchymosis but can progress to disseminated intravascular coagulopathy (DIC). Other symptoms of APL include those related to pancytopenia, including weakness, fatigue, and infections.
The prognosis for APL is considered to be excellent. Tretinoin (ATRA) interacts with the PML-RARA fusion product allowing for maturation and differentiation to occur along the granulocytic lineage, eliminating the promyelocyte population. Combination therapy with tretinoin and arsenic trioxide has become the gold standard of care leading to excellent remission rates.
References
Kakizuka,A., et al. “Chromosomal translocation t (15; 17) in human acutepromyelocytic leukemia fuses RARα with a novel putative transcription factor,PML.” Cell 66.4 (1991): 663-674.
Lo-Coco,Francesco, and Laura Cicconi. “History of acute promyelocytic leukemia: atale of endless revolution.” Mediterranean journal of hematologyand infectious diseases3.1 (2011).
Rowley,JanetD, HarveyM Golomb, and Charlotte Dougherty. “15/17 translocation, aconsistent chromosomal change in acute promyelocytic leukaemia.” TheLancet 309.8010 (1977): 549-550.
Swerdlow,Steven H. WHO Classification of Tumours of Haematopoietic and LymphoidTissues. International Agency for Research on Cancer, 2017.
-Christopher Felicelli is an M3 at Loyola University Chicago Stritch School of Medicine. Follow Chris on Twitter at @ChrisFelicelli
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
This time, I’ve got something to talk about that’s a little more serious. I don’t like to deviate from fun lab-related memes and insights,but every now and then something really strikes a chord. Enough so to talk to all of you about it. Some of you reached out to me after my post discussing clinician burnout and suicide in healthcare and that felt great; connecting with people who had some powerful stories to share really validated that conversation. Today, I want to talk about guns. Specifically, the public health epidemic of gun violence, the current conversation about whose “lane” (read:responsibility) belongs to whom, and what role those of us in laboratory medicine play.
I was horrified to see the recent shooting and murder of three in my Chicago home at Mercy hospital in the Near South Side. I won’t rehash the details that are on the news. Emergency resident physician Dr.Tamara O’Neal, newly minted Chicago Police Officer Samuel Jimenez, and pharmacy resident Dayna Less were all shot and killed point-blank by a gunman in the Mercy Hospital emergency department. A place that is supposed to be for healing, safety, and hope. Senseless.
Image 1. Victims of the Mercy Hospital shooting: (L-R) emergency room Dr. Tamara O’Neal, Chicago police Officer Samuel Jimenez, and pharmacy resident Dayna Less. These were all new to their careers, whose lives were abruptly ended by senseless gun violence. Source: ABC7 Chicago.
This now presses the start button on America’s newest tradition: a very short-lived, ill-timed, and often tone-deaf debate about the firearm subculture in our nation. Okay, bias check: you should know that I am not a fan of guns of any kind. If it were up to me, they would either belong in museums or find more useful lives melted and repurposed as metal used to reinforce hurricane-prone buildings or safe hypodermic needles for patients in need. That said, this isn’t a gun debate article; nor is it an open forum to discuss gun control, the second amendment, the NRA, or anything political. I respect opinions and educated civil discourse, but this piece today is focused on health—public health.
The epidemic of gun violence in America is a problem. The American Public Health Association (APHA) posted on their website extensively on the topic of gun related deaths which “kill more than 38,000 people and cause nearly 85,000 injuries each year. As a longtime advocate for violence prevention policies, APHA recognizes a comprehensive public health approach to addressing this growing crisis is necessary.” (Read their fact sheet here)Furthermore, the American College of Physicians (ACP) published a position paper on the topic in the Annals of Internal Medicine journal (read it here)where they establish a comprehensive set of recommendation from a conglomerate of clinical medical specialty organizations. Increasingly now more than ever does this prevalence of gun related injury and death present itself as a major health concern: a public health epidemic. I could talk to you about the number of mass shootings in our country, or the epidemiologic incidence of gun-related deaths compared to other countries, even the policy discussion around gun ownership and regional policies regarding safety and gun control—it doesn’t matter. All the charts and graphs any recycled article on the subject will just fade into the mist of “yet another shooting.” That’s not okay. I don’t want to drown you in data. Better put, I can’t. See, the problem is you’ll see the same pieces of information regarding the gun debate as you scroll through the news on your social media. Something new I want to add to this conversation is the overwhelming emphasis on the simple truth that this is a public health issue.
Image 2. In the US, we fund approximately as much research for gun violence as we do for drowning and falls. Of the three, mortality related to gun violence is about the same as sepsis—and that’s heavily documented. Source: Journal of the American Medical Association.
This unfortunate new reality is no different from other public health programs that have addressed various issues over the past decades. What do deaths from motor vehicle accidents, fires, smoking-related ung cancer, obesity and type 2 diabetes, heart attacks, antibiotic resistant bacterial infections, and traumatic brain injuries have in common? Per the American Foundation for Firearm Injury Reduction in Medicine (AFFIRM), they were all public health crises that pushed medicine past a breaking point in clinical burden and forced us to invest in research which conclusively provided results to address related mortality and morbidity. AFFIRM is a non-profit organization which is building a coalition in medicine for the purpose of researching and addressing this newest public health issue. They argue that,without medical evidence we won’t be able to find solutions to the senseless loss of life from gun violence. Death from car accidents gave us the seatbelt and tickets for disobeying its required legal usage. Death in home fires got us the smoke detector and regulations surrounding their installation. Lung cancer deaths led to smoking cessation programs, increased taxation, and policy changes regarding access to cigarettes. Sugar-related morbidities created a conversation about healthy diets, public policies addressing food deserts, and taxation programs for drinks with added sugar. Heart attack deaths gave us longitudinal studies for best care practices and lifestyle recommendations.Resistant bugs established a new discussion on antimicrobial stewardship. Brain injuries gave us new guidelines for concussions. I could go on. That’s only the tip of the public health iceberg. The point is that if there is an epidemiological trend where people are literally dying, data married with health metric-oriented research create solutions!
But let’s add deaths from gun violence to that list. What then do they all have in common, besides the concern for improving public health? Save for the tragically evident lack of a solution, the similarity becomes clear: there is lobby, interest, power, and support. Cars didn’t always have seat belts, cigarettes used to be cheap and doctors used to smoke at work,no one talked about cheeseburgers giving you heart attacks and diabetes decades ago, and helmet-clashing football players didn’t always receive the treatment they needed. Why? Because some entity—corporate, societal, etc.—wasn’t keen on“buying in.” Much like it takes justification and convincing for administration to buy your fancy chemistry analyzer, so do the public and oppositional lobby groups which require swaying toward the intervention(s) being proposed.
Image 3. The Dickey Amendment passed in 1996 was a small rider in a bill that was part of a larger budgetary spending bill. Effectively, it completely disallows public health research into gun related deaths, gun violence, or any publication that would endorse gun control or limitations. Source: 104th Congress.
Often, the data stacks high enough to influence decisions on its own. But that isn’t the case with gun related mortality. I see gun related violence as sort of the opposite of the vaccine debate: with the flu shot there seems to be too much data and not enough stories to convince the anti-vax movement to realize the significant threat being addressed. On the other hand, gun related violence exhibits far too many stories without any significant amounts of data. Possibly, this might be related to the limitations placed upon the CDC since the mid-1990’s that forbid them from using funds “to advocate or promote gun control.” Yes, really. Just last month, I wrote about the newest advancements in influenza testing and the best practice of vaccinating annually.I cited thousands of deaths related to vaccine-preventable or epidemiologic illness; 80,000 dead from influenza last year, thousands from swine flu over a decade ago, etc. But when you try and cite proper, medical data regarding guns in public health, its … not so easy. No data, no research. No research, no change.
Many of you have undoubtedly read about the current social media “discussion” regarding whose “lane” gun violence is to navigate: The National Rifle Association (NRA) asserted in a tweet that doctors, discussing the issue only within their field should leave it to more “qualified” groups like them. That’s been a tinder box of vitriol the medical community, for lack of a better term, is up in arms about. I followed and read tons of comments about this as it unfolded, hearing from endless doctors, nurses, and laboratorians posting with blood spattered scrubs, decimated trauma bays, and emptied blood bank refrigerators that this growing epidemic is enraging clinicians about. Earlier, I highlighted similarities between public health problems and their respective solutions citing that they all shared oppositional lobby groups. What better profession to handle the topic in question than medicine—whose associated lobby power from professional societies like ours to Big Pharma amass one of the largest voices in policy making in America. And another thing, as gun violence is a public health concern, whose literal job is it to address health, mortality, and morbidity? All of ours. Nurse educators lead patients through lifestyle modifications they can employ to curtail some effects of diabetes, physicians manage patient treatment regimens balancing input from pharmaceutical tools to professional guidelines,clinicians like us strive to provide the best resources available by advancing hemoglobin A1c levels or point of care testing. We all play roles in every single healthcare matter that translates to life or death, so why not this one?
So, I touched on it a little here, but what role does the medical laboratory professional play? Besides bullets in tissue section, how does the public health epidemic of gun violence reach the lab? I wasn’t so sure, until I read a story about Dr. Julie Melinek, a forensic pathologist with UC Davis and the Alameda County Sheriff’s Department. In response to the NRA’s“stay in your lane” tweet regarding gun deaths, Dr. Melinek tweeted “Do you have any idea how many bullets I pull out of corpses weekly? This isn’t my lane. It’s my [expletive] highway.” She proceeded to turn her phone off and work for a few hours. When she returned, things were viral. In an interview with Medscape, she discussed this story and the topic at large with editor-in-chief Dr. Eric Topol. She talked about the epidemiologic role clinicians of all specialties play in risk assessment and harm reduction,saying “…if we see something that’s dangerous for the pediatric population,like a toy that breaks apart or is a choking hazard, we report it to the Consumer Product Safety Commission and it gets recalled because it’s a hazard.”She and Dr. Topol explored the ways clinicians can advocate for patients and public health at large, concluding with some poignant words, encouraging those of us in medicine to reach out to elected officials. The internet facilitates such an easy way to communicate, she says that it becomes paramount to voice the opinions held within the medical community to those in policy-making; especially clinicians who may own guns or be active NRA members! Because, ultimately, this isn’t about gun ownership or second amendment rights—its about the health, well-being, and safety of our patients.
Dr. Melinek represents a single voice within the pathology community. You’ve read my posts about lab management values, interdisciplinary team work, attainable goals, and utilization of data to make clinical decisions. Those of us in lab medicine find ourselves at the forefront of translating data into decisions. When quality control measures on instrumentation fail to correct after countless interventions, do we continue running assays? No! We work-up and investigate what root cause is the problem and fix that if possible; thinking outside the box, looking at lesser-than-obvious causes, investigating all possible solutions, etc. In pathology we’re the first to implement new, highly advanced tests and corroborate with other specialties about what the new changes mean for patient care and management of diseases (i.e. 5thgeneration high-sensitivity troponins and evolving to a new standard of care for acute coronary syndromes). We’re also the first to notice trends that impact patient outcomes and the first to provide solutions: think back to the last time you spent a few minutes reading your labs metrics and goals posted somewhere at work. Dr. Melinek collecting bullets from her autopsy patients is no different than forensic pathologists historically noting trends in mortality statistics, iatrogenic, environmental, and other causes of death.And, when those trends get published and presented, they call for further research and investment into public health interventions that may prevent those deaths in the first place. Pathology, public health, epidemiology, and laboratory medicine are built for this. We’re the tangible bridge between what gets discovered and what gets researched. We’re also in a privileged position to have a bird’s eye view of a larger clinical, epidemiologic picture as pathologists see populations of patients.
In a recent Lablogatory post, ASCP’s Lotte Mulder (ASCP Leadership Institute and Patient Champions programs) wrote about Moral Capacity, Courage, and Resiliency. Specifically, she said “It is not enough to understand and recognize a moral dilemma, it is important to act on it… it is critical for leaders to understand that culture influences moral and ethical behavior.” If America’s gun violence problem is one that desperately needs data, then why shouldn’t we, then, be professional and cultural leaders and advocate through data collection, analysis, and translation like we always do? Let’s use our tools and our talent for lab medicine, in partnership with the growing coalition of clinical professional specialties, and cultural humility for the populations we protect, and address this once and for all.
Thank you.
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
The patient is a 54 year old woman who presented to the hospital after a fall, which revealed a pathologic fracture of T1 and a spinal lesion from C6/C7 to T2. CT of the chest/abdomen and pelvis at the time showed a large mass in the anterior mediastinum with extensive lymphadenopathy and lytic lesions in the spine and ribs.
C7-T1 Soft Tissue Excision
H&E 20X H&E 50X H&E 100X CD30BSAP/PAX5KI-67
Diagnosis
Sections show sheets of large epithelioid-like cells with segmented nuclei with variably prominent nucleoli and ample amounts of eosinophilic cytoplasm.A majority of these larger cells have abundant cytoplasm and lobulated nucle iwith multiple nucleoli and a surrounding halo. They are consistent with Lacunar cells. These cells form large aggregates and are admixed with numerous neutrophils, histiocytes and scattered lymphocytes.
Occasional Hodgkin cells and multi-nucleated Reed-Sternberg cells are seen, as well as scattered medium size hyper chromatic cells with irregular nuclear contours and scant cytoplasm consistent with mummy cells.
Immunohistochemical staining revealed that the largea typical cells are immunoreactive for CD30, CD15 and PAX5/BSAP. CD45 highlighted background lymphocytes but showed infrequent dim staining in the large atypical cells. By Ki-67, the proliferation index is 50-60% in the large atypical cells. Taken together, the findings are consistent with Classic Hodgkin Lymphoma, nodular sclerosis, syncytial variant.
Discussion
Classic Hodgkin lymphoma (CHL) has four distinct subtypes including nodular sclerosis, lymphocyte-rich, mixed cellularity and lymphocyte-depleted. These subtypes differ based on characteristics of the background non-neopalastic reactive cells and the histomorphology of the Hodgkin/Reed-Sternberg cells (HRS). Nodular sclerosis Classic Hodgkin lymphoma accounts (NSCHL) for approximately 70% of all CHLs. The mediastinum is the most commonly involved site and it generally occurs in people between the ages of 15-34 years old. Generally, the histology shows nodules with surrounding fibrosis. There are a variable number of Hodgkin/Reed-Sternberg (HRS) cells mixed with other inflammatory cells. The characteristic HRS cell is called a lacunar cell. This is a type of HRS cell with more cytoplasm, less prominent nucleoli and can show retraction of the cytoplasm in formalin-fixed tissue that gives the cell a halo or “lacunae.”1
The syncytial variant (SV) of CHL, nodular sclerosis was first described in the 1980s. It presents in 5-15% of cases of NS CHL. It is characterized by sheets and clusters of “lacunar cells” typical of the type of HRS cell most commonly seen in NS CHL. Previous studies had determined the SV of CHL to have a worse prognosis and more aggressive course than other subgroups. In a more recent study by Sethi, et. al. the clinical features and response to treatment of patients with SV were compared to patients with typical NS CHL. Within the cohort, 43 patients with SV were compared to 124 patients with typical NS CHL. The study found that there was no significant difference in age, sex, performance status, stage, bulky disease, number of nodal sites and chemotherapy regimens used between the two groups.2
As far as treatment outcomes, the rate of complete response in the SV group was 74% vs. 87% in the NS group. This result approached statistical significance with a p=0.05. The medium progression-free survival in the SV group was significantly shorter compared with the NS group. The overall survival, however was not statistically different, indicating that salvage chemotherapy was ultimately able to match the clinical outcomes for patients with SV type to patients with NS type. 2
Currently, all CHLs are treated with adriamycin, bleomycin,vinblastine, decarbazine (ABVD) chemotherapy regimen plus or minus radiation therapy regardless of subtype. Patients with relapsed or refractory disease are treated with a “salvage” chemotherapy regimen followed by an autologous stem cell transplant. Emerging therapies including PD-1 inhibitor nivolumab have shown great effect in patients with CHL. PD-1 or programmed death ligand 1 is overexpressed on HRS cells. This ligand binds with receptorson T-cells to prevent the T-cell immune response and reduce cytokine activation and targeted response against the proliferating HRS cells. By using an antibody against the PD-1 ligand in CHL,the ability of the tumor to suppress the immune response is decreased and patients have been shown to have better clinical response rates.3
Patients with SV do need to be recognized as a distinct subgroup that may have a higher risk of disease progression with first line chemotherapy agents. Due to the high numbers of HRS cells seen in patients with SV and the increased failure rate of initial chemotherapy agents, antibody therapies such as PD-1 inhibitors may be even more successful in those patients.
References
Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues (Revised 4thedition). IARC: Lyon 2017.
Sethi, T.K., et al. Differences in Outcome of Patients with Syncytial Variant Hodgkin Lymphoma (HL) Compared with Typical Nodular Sclerosis HL. Blood. 2015;126(23),1441. Retrieved from http://www.bloodjournal.org/content/126/23/1441.
Bond DA, Alinari L. Emerging treatment options for the management of Hodgkin’s lymphoma:clinical utility of nivolumab. J Blood Med. 2017;8:41-54. Published 2017 May 11. doi:10.2147/JBM.S117452.
–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
#PathTweetAward is a crowdfunded award created
on Twitter by pathologists to recognize pathologists and pathology trainees who
post exemplary educational tweets in the field of anatomic or clinical pathology.
How and when
was #PathTweetAward started?
The idea for an “educational pathology Tweet ofthe year” award was proposed on Twitter on April 6, 2018.
The tweet that launched the concept of #PathTweetAward.
The hashtag#PathTweetAward was created the next day based on a suggestion by Dr. Amy Deeken (@AmyHDeekenMD), a pathologist from Ohio who is active on social media. A Twitter handle (@PathTweetAward) and a promotional video to create awareness about the award were created shortly thereafter by Dr. Muhammad Ahsan (@ahsanuitis), a pathologist from Pakistan. The award was supported online by several pathologists with a prominent social media presence, including Dr. Jerad Gardner, Dr. Kamran Mirza, Dr. Christina Arnold, Dr. Julie Teruya-Feldstein and Dr. Kalyani Bambal.
What is
crowdfunding? How was #PathTweetAward crowdfunded?
Crowdfunding is a fundraising method in which small amounts of money are contributed by a large number of people, typically via the internet. Crowdfunding for #pathtweetaward was made possible by Dr. Amy Deeken, who started up a GoFundMe account for the award on April 7, 2018 (gofundme.com/5dakxso) and created a promotional video. Incredibly, the fundraising goal of $1000 was reached within a single day of setting up the GoFundMe account. At the time of this writing, the account has raised $1550, generously donated by 26 individuals (predominantly pathologists) over a period of 6 months.
The GoFundMe account that funds #PathTweetAward.
Who is
eligible for the award?
Pathologists in practice, pathology residents,
and pathology fellows anywhere in the world are eligible for the award. To be
considered, a tweet with educational value should be posted on Twitter and
brought to the attention of the screening judges by using the hashtag
#PathTweetAward.
Who is
allowed to use the hashtag #PathTweetAward?
Anyone can use the hashtag. Any pathologist anywhere in the world can tag an educational post on Twitter in a reply or retweet. An example is shown in the image below. Pathologists can also self-tag their own tweets if they wish.
To nominate a tweet for the award, simply reply to the original tweet and type #PathTweetAward. You can also “retweet with comment” and type #PathTweetAward in your comment.
Are the
awards monetary?
Yes, the current plan is to award four
monetary prizes each year ($500, $300, $200 and $100), including two awards in
the open group and two awards for trainees. The
Pathologist magazine and the American Society for Clinical Pathology (ASCP)
have generously offered additional non-monetary support, mainly in the form of promotion
of award-winning tweets and awardees.
How are
winners selected?
Judges for #PathTweetAward are pathologists who are active on Twitter. There are three panels of judges, selected with diversity and inclusion in mind; judges include women and men, trainees and faculty, community pathologists and academics. A different panel of judges will be selected each year. The bulk of the work is shouldered by two panels of five screening judges each. One, led by Chicago hematopathologist Kamran Mirza, MD, PhD,screens tweets from trainees only. The other, led by Canadian head and neck pathologist Bin Xu, MD, screens tweets from an “open” group that includes trainees and practicing pathologists.
Screening
judges (for trainee tweets only)
Screening
judges (for “open” category, including all pathologists, including trainees)
Final
judges
Kamran
Mirza, MD (group leader)
Bin Xu, MD (group leader)
Jerad
Gardner, MD (group leader)
Elvira
Gonzalez-Obeso, MD, PhD
Eman
Aljufairi, MD
Silvija
Gottesman, MD
John
Gross, MD
Daniel
Skipper, MD
Valerie
Fitzhugh, MD
Adam L. Booth,
MD
Yiang Hui,
MD
Laura G.
Pastrian, MD
Pallavi A.
Patil, MD
Chen Yang,
MD
Geronimo
Junior, MD
Table 1. Judges for #PathTweetAward (2018)
Each week, tweets tagged with the hashtag #PathTweetAward are collated by a screening judge and posted publicly on Twitter using the “Moments” feature. These collections serve as a repository of the best tweets, from which each panel of screening judges selects a “tweet of the month” to be sent at the end of the year to the final panel of judges.The latter are tasked with selecting four final prize-winners, two from the open group and two from the trainee-only group. The final four shortlist will be posted publicly in a Twitter poll, at which time the general public can vote to determine the final ranking. The process, summarized by screening judge Dr.Elvira Gonzalez-Obeso, is shown in this image:
Summary of the process by which #PathTweetAward winners are selected.
-Sanjay Mukhopadhyay, MD is a Staff Pathologist at the Cleveland Clinic in Cleveland, OH. He is an expert thoracic pathologist,author of a lung pathology textbook, and a pioneer in the use of social media for teaching lung pathology globally, free of charge. Follow Dr. Mukhopadhyay on Twitter @smlungpathguy, and check out his freely accessible educational videos on YouTube.
Platelets are our first line of defense in controlling bleeding. Abnormally low numbers of platelets can lead to easy bruising, tiny leaks from capillaries into the skin and mucous membranes, causing petechiae, and bleeding. The platelet count is a significant parameter in the CBC and it is therefore vital to be able to report accurate and precise platelet counts. Furthermore, physicians must be able to use this information to diagnose the cause of the thrombocytopenia in order to recommend treatment.
What a platelet count alone cannot tell us is the reason for thrombocytopenia. Just as there can be many reasons for a low hemoglobin, and many causes for an increased or decreased WBC, there are numerous causes for a decreased platelet count. After ordering a CBC, the next steps in determining etiology of thrombocytopenia have historically been a thorough physical with attention to any bleeding symptoms and organ enlargements, and a medical history. The medical history should include family history, and notation of recent viruses or drug therapies. After these tests, a bone marrow aspirate and biopsy may also be necessary to clarify etiology. While modern, automated hematology analyzers produce reliable platelet counts, measuring only the circulating platelet count does not give us any information as to the etiology, so there is a need for further testing. With thrombocytopenia, platelet counts can be less reliable than with normal counts.Platelet counts were originally performed by impedance methods, then better accuracy and precision was obtained with optical platelet counts. Physicians rely on precision with very low platelet counts to make informed decisions about when to transfuse patients. The problem with the impedance counts at the low end, is that RBC fragments, schistocytes and microcytic RBCs can be counted as platelets, giving a falsely high count. On the other hand, measuring platelets by size can miss large platelets leading to a falsely low count.
Historically, the mean platelet volume (MPV) has been used along with the platelet count to aid in making a differential diagnosis. The MPV is analogous to the red cell distribution width (RDW) for red cells, and can be used to as an indicator of the maturity of platelets. Young platelets are the largest, and as they age, the size decreases. The normal ranges for MPV are generally about 9-12 femtoliters (fl).The MPV will be higher if more platelets are being released from the bone marrow, and lower if fewer are being newly released and we are counting mature platelets. Thus, the MPV can be used as an indirect marker for platelet production. However, an inherent problem with the MPV is that, similarly to the impedance platelet count, this count can be unreliable because any RBC fragments or particles may interfere with the measurement.
So, what is a physician to do?And how can the lab provide information to help them make the best differential diagnosis and transfusion decisions? In an effort to provide a parameter that could help differentiate causes of thrombocytopenia, the concept of reticulated platelet counts (retPLT) was first introduced in research in the late 1960s. The term is used to describe immature, functional platelets in the peripheral blood.Reticulated platelets are to mature platelets as reticulocytes are to mature red blood cells. These are the youngest platelets, within 24 hours of being released from the bone marrow. Reticulated platelets are large, with increased amounts of RNA, and the number in the circulation can be used to provide an estimate of the rate of thrombopoiesis. Originally, these were stained with new methylene blue and manual counts were done, much like a manual reticulocyte count; tedious,and imprecise. It wasn’t until about 30 years later that a flow cytometry method was described for measuring retPLT. Using traditional flow cytometry, reticulated platelets can be stained with a Thiazole Orange dye and passed through a flow cytometer. This method, however, has been shown to have wide normal ranges from 1-15% because of the lack of analytical standardization. Variations in the concentration of the thiazole dye used, the timing, and the gate settings all make it difficult to compare results obtained from one laboratory to another. In addition, flow cytometry is time consuming, labor intensive and costly.
Newer flow cytometry methods are now available on select hematology analyzers. There are currently 2 companies that have analyzers that can report retPLT using routine CBC reagents and controls. Reticulated platelets can be measured with the same K2 EDTA tube used for the CBC. The test is automated, simple to perform, fast, and gives standardized results with tighter normal ranges. The Abbott CELL-DYN Sapphire measures the retPLT using a fluorescent dye and flow cytometry with 2 dimensional gating. Sysmex XE and XN analyzers offer several Advanced Clinical Parameters including measures of reticulated platelets, expressedas the Immature Platelet Fraction (IPF%) and the Absolute Immature Platelet Fraction Count (IPF#). Sysmex offers a fluorescent platelet count (PLT-F) as an addition to impedance counting (PLT-I) and optical counting (PLT-O). PLT-F is more reliable because it uses a platelet specific dye which eliminates noninterference seen with other methods. The fluorescent dye labels the RNA and forward scatter is used to determine size while fluorescence is used to measure RNA content. With gating set based on cell volume and RNA content, the PLT-Fcan be measured. When there is an abnormal scattergram or a low platelet count,the PLT-F is reflexed and the IPF% and IPF# are also reported.
What’s the clinical utility of the IPF? Thrombocytopenia can have many causes.Immature platelets are functioning platelets, and an increased IPF means that we have more newly formed immature platelets circulating. The IPF helps physicians to differentiate thrombocytopenia caused by platelet destruction or consumption versus thrombocytopenia caused by deficient platelet production in bone marrow failure. It is vital to know the pathogenesis of thrombocytopenia in making decisions about treatment. With these advanced parameters, these decisions can often be made without costly, time consuming flow cytometry,without an invasive bone marrow biopsy and without waiting for the results of such biopsy. This can often save a patient an unnecessary platelet transfusion.
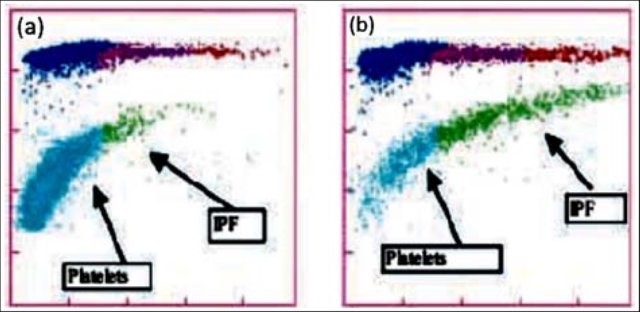
The reference range for IPF% in healthy individuals is1.0-7.0%. Together with a low platelet count, an increased IPF indicates an increase in platelet production. This is seen in patients with excessive destruction of platelets. An example of the clinical utility of the IPF can be seen in the diagnosis of immune thrombocytopenic purpura (ITP). ITP is an autoimmune bleeding disorder in which the immune system makes anti-platelet antibodies which destroy platelets. Acute forms occur more often in children while adults can have chronic ITP. ITP can be diagnosed on clinical findings but laboratory confirmation is often necessary. This can be expensive with long turnaround times using traditional flow cytometry and/or bone marrow aspirates.An IPF reported with a CBC is fast, inexpensive, and be extremely beneficial in aiding a timely diagnosis. Patients with ITP have been shown to have the consistently highest IPF values with ranges from 7-28%.1 As their platelet counts recover, the IPF% returns to the normal range, without the need for transfusions. Thus, the IPF can be used not only to help diagnose but also as an indicator of remission.
Figure1. Platelet scattergrams from a healthy individual with a normal IPF (a) and a patient with a high IPF (b). Mature platelets appear as blue dots, green dots represent the IPF with increased cell volume and higher fluorescence intensity compared to mature platelets1
In contrast to what we see with ITP, thrombocytopenia with alow normal or decreased IPF indicates decreased bone marrow production of platelets. Patients with bone marrow failure are more likely to have bleeding episodes with low platelet counts and may need transfusion. Rapid differential diagnosis using the IPF can help physicians help these patients get early treatment.
IPF may also be a reliable indicator of bone marrow recovery. Traditionally, neutrophil counts have been used as an indicator of recovery after a bone marrow transplant. IPF can be used as an indicator of imminent platelet recovery. It has been shown that,post-transplant, the IPF% increases before the platelet count. In a study done with stem cell transplant patients, it was shown that the absolute neutrophil count took an average of 13 days to recover, compared to 9 days for the IPF. The IPF was shown to recover before the Immature reticulocyte count, platelet count and absolute neutrophil count, giving physicians earlier indication that the transplant was successful.2 This is significant because it can eliminate the need for bone marrow biopsies and platelet transfusions.
Thrombocytopenia is not an uncommon finding in neonates, particularly in the neonatal intensive care unit (NICU). There are various causes for this, including sepsis, placental insufficiency and immune thrombocytopenia. The IPF% and IPF# can be used to diagnose and distinguish the cause of thrombocytopenia in neonates, and direct the treatment. When platelet count platelet count drops below 50 x 103/Lin an otherwise healthy appearing infant in the first 72 hours of life, neonatal alloimmune thrombocytopenia (NAIT) can be suspected. This condition is similar in pathogenesis to hemolytic disease of the fetus and newborn (HDFN), and is caused by an incompatibility in human platelet antigens between mother and baby. This occurs most often when the mother is HPA-1b and the father and baby are HPA-1a. The mother forms anti-HPA-1a which crosses the placenta and destroys the fetus’ platelets.This is a thrombocytopenia caused by platelet destruction, and the IPF% is high. The condition is self-limiting and resolves in 1-4 weeks. Neonatal sepsis can also present with a high IPF, but typically is found in very sick or premature babies and the degree of thrombocytopenia is not as severe as with NAIT. In contrast, neonatal thrombocytopenia due to placental insufficiency would exhibit a decreased IPF due to a deficiency in platelet production. Using the IPF% and IPF# to help differentiate the causes of neonatal thrombocytopenia can help steer the treatment and save infants from unnecessary invasive procedures and transfusions.
TheIPF has proved to be very valuable in the clinical setting. It has been used in the investigation of etiology in secondary thrombocytopenias due to chronichepatitis C, liver disease and HIV. It has been used to guide treatment in thrombocytopenias such as thrombotic thrombocytopenic purpura (TTP). IPF can also be useful in evaluation of hereditary platelet thrombocytopenias. The IPF% and IPF# can be compared after transfusion to support the theory that, after platelet transfusion, theIPF% will decrease due to the newly increased platelet count, but the IPF#remains the same. This validates that the IPF is a reflection of continual platelet production by the bone marrow.4
IPF%and IPF# are expanded CBC parameters that physicians can use to aid in differentiation of various thrombocytopenic states. Treatment for the different classes of thrombocytopenia can differ drastically, and knowing the class of thrombocytopenia helps direct the management. The IPF parameters are automated,easy to perform at the same time as the CBC, and provide standardized results that are inexpensive and available 24 hours a day in the hospital setting. Using the IPF can also reduce diagnostic costs for the patient. Many studies have been conducted on the varied applications of the IPF and research continues investigating possible further uses of this advanced clinical parameter. This is the new hematology, constantly providing the clinician with better tools for making diagnoses and treating patients. Platelet counts alone and MPVs are out. Make room for the new kid on the block; the IPF is in.
References
Arshi Naz et al. Importance of Immatureplatelet Fraction as a predictor of immune thrombocytopenic purpura. Pak J MedSci 2016 Vol 32 No 3:575-579
Zucker ML et al. Immature Platelet fraction asa predictor of platelet recovery following hematopoietic progenitor celltransplanatation. Lab Hematol 2006 12(3):125-30
Briggs,C. Assessment of an immature plateletfraction (IPF) in peripheral thrombocytopenia. Br J Haematol 2004Jul;126(1):93-9
Sysmex White Paper. The role of the ImmaturePlatelet Fraction(IPF) in the differential diagnosis of thrombocytopenia. www.sysmex.com/us
Fujii,T et al.. A new approach to detectreticulated platelets stained with thiazole orange in thrombocytopenicpatients. Thromb Res. 2000 Mar 15;97(6):431-40
Cremer Malte The immature platelet fraction(IPF) in neonates. Diagnostic Perspectives 2011 Vol1:36-42
Cremer M. et al. Immature platelet values indicateimpaired megakaryopoietic activity in neonatal early-onset thrombocytopenia.Thrombosis and Haemostasis 2010; May;103(5):1016-21
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
While Maria was working in Microbiology, she cut her finger while pulling reports off of the printer. It was a minor paper cut, so she ignored it, put her gloves on and continued her work back on the bench. A week later, the tiny cut was swollen and red. She decided to report the incident to her manager since it wasn’t healing. The manager asked Maria to report to the Occupational Health department, but was unsure if any treatment would be covered since the incident was not reported while she was at work.
Steve and Josh were bored during the night shift and they created a ball made from rubber bands to toss around. When Josh didn’t catch the ball, it hit the open tray of formaldehyde on the gross bench, and it splashed into Josh’s eye. He rinsed his eyes in the eyewash station for a couple of minutes, but both men were afraid to report the incident for fear of getting in trouble. Josh’s eye irritation continued to worsen, and he had to go to the eye doctor for treatment.
There are obvious consequences for injuries that occur in the laboratory, and reporting them is important for many reasons. Staff may be motivated in some instances to not report, but that creates problems for the individual, the department, for the facility, and even for other labs across the country! That may seem like a stretch, but it will become clearer with exploration.
The value in injury and accident reporting starts with medical follow-up. Those incidents which require treatment or abatement of infection can and should be dealt with quickly, and appropriate monitoring can be done if necessary. Some injuries may require immediate first aid, and a trip to the emergency department may even be necessary. Not reporting those types of injuries can be very dangerous for staff. Other incidents may require physician office visits or other monitoring, and employees who need it should be encouraged to comply.
In many work places the injury follow-up visits and treatment are covered financially by the institution, either via a structured occupational health program or through reimbursement. Some organizations may not offer financial coverage, however, if the incident that occurred at work is not reported as soon as possible. That reporting delay can raise suspicion as to whether or not the injury actually did occur while on the job, and since the written reporting protocol was not followed, there may also be no obligation for employer medical coverage.
Departmental issues will arise when incident reporting in not part of the overall lab safety culture. Sometimes there can be reprisals for unsafe behaviors which lead to accidents, but if the safety culture is good and if managers and employees coach against such practices, then there should be fewer overall incidents to report. That said, a culture of secrecy regarding injuries or exposures can also be dangerous. There is value in talking to all staff about an incident that occurred within the department. Staff can learn from the event and have a healthy discussion about how to keep it from reoccurring. A discussion of events can bring important safety issues to light, particularly if similar incidents happen with multiple people. This sharing of information can also promote awareness of good safety practices that can aid in the prevention of further incidents for all who work in the department.
OSHA requires the reporting of certain work place injuries, those that may have led to time away from work or that need medical follow up, for example. This injury data is compiled and reported nation-wide. It becomes a good source for benchmark data, a way to be able to compare your lab injury rates with others across the country. The U.S. Bureau of Labor Statistics provides this data as information labs can use. One way to utilize the information is to see if the number of reportable injuries you are seeing in your lab is comparable to a national average. That assessment can give you a starting point in determining whether or not your lab’s safety incidents are at typical levels. Of course, lab safety professionals want to see zero injuries, but if you see your lab injury numbers are very high compared to benchmark data, you can begin to see where to focus in on fixes for the lab physical environment or on creating specific safety training.
There is great value in talking about safety incidents that may result in injury or exposure in the lab setting. These “safety stories” raise awareness of safety issues, and they can act as a deterrent for repeat incidents. Create a culture where staff feel free and comfortable to report incidents, and be sure to discuss them with all staff, and record reportable injuries as well. Having reliable national data also provides helpful information to other labs, and better information can help to improve safety in laboratories everywhere!
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Recently, a new technology has become available for screening the esophagus for early detection of at-risk patients for cancer. Esophageal cancer has one of the highest mortality rates. Watch this interview with Rob Odze, a pathologist who works with the technology, and learn more about how this could impact the practice of clinicians, pathologists, and laboratory professionals involved in upper endoscopy services.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
For patients with gender dysphoria, the Endocrine Society has endorsed the use of hormone therapy to promote secondary sexual characteristics of the desired gender. These guidelines were first established in 2007 and revised last year, and gave the first evidence guided recommendations for clinicians treating transgender patients.
For transgender males, testosterone by itself is prescribed as an injectable oil-based solution. These doses are given as intramuscular injections- usually into the thigh. If that’s too painful, subcutaneous injections have been shown to have similar efficacy. The doses given to transgender males is much higher (50-100mg/ injection) than that given to men with testosterone deficiency (30-50 mg/ injection). Primarily because the men have more testosterone to start with. Also, whereas topical testosterone gel may be sufficient for men with “low T,” it doesn’t seem to provide enough testosterone to transgender males and is quite expensive, so it is generally not used.
Image 1. Picture of testosterone cypionate vial from mcguffmedical.com. This is used for intramuscular injections.
Upon starting testosterone injections, the frequency of injections is every one to two weeks. However, the onset of physical secondary sexual characteristics takes 3-6 months to begin. After about 3 years, most of the changes to occur will have manifested. These physical changes are outlined in the table below. You’ll notice how certain traits like cessation of menses and fat redistribution start within the first 6 months whereas muscle growth and voice change take effect after 6 months. Also, the time certain effects take maximal effect varies; the voice doesn’t deepen further after 2 years, but hair growth continues to increase through 5 years.
Physical Effect
Begins
Maximal Effect
Facial/body hair growth
6-12 mo
4-5y
Skin oiliness/acne
1-6mo
1-2y
Scalp hair loss
6-12 mo
–
Increased muscle mass
6-12 mo
2-5y
Fat redistribution
1-6mo
2-5y
Cessation of menses
1-6mo
–
Deepening of voice
6-12 mo
1-2y
Table 1. Timeframe of physical traits that manifest in transgender males while taking testosterone hormone therapy. Based on Hembree et al. 2017 (1).
Just as hormone therapy induces physical manifestations of secondary sexual characteristics for transgender men, we would suspect that internal aspects of physiology are affected too. Values measured by the laboratory provide meaningful insight into how our body and its different organ systems are functioning. Accordingly, the Endocrine Society also recommended laboratory monitoring of transgender patients starting hormone therapy.
Measure Testosterone and hemogoblin/ hematocrit every 3 months for the 1st year, then 1-2x/ year afterwards.
Monitor Lipids at regular intervals
Previous studies have monitoring these lab values found consistent increases in hemoglobin and hematocrit (2,3). This is due to the stimulation of erythropoiesis by testosterone (4). While excessive testosterone could lead to polycythemia (excessive RBCs in the blood), it is not a commonly described complication in transgender patients. Some summary results from our study for hemoglobin and hematocrit are shown in Figure 1A, which shows a clear shift in levels.
However, reports on lipids have been varied LDL and triglyceride changes (2,3). The only consistent finding was that HDL decreased in transgender males taking testosterone (2,3). In our study, we found triglycerides were increased with decreased HDL (Figure 1B). The take-away is that because cardiovascular cut-offs are based on risk and not a reference range, patients and clinicians will have to be aware of these possible metabolic changes.
Creatinine, when it was checked, increases for transgender males (5). We found creatinine was strongly increased in our study to become similar to baseline creatinine in transgender women before taking hormone therapy (Figure 1C). This topic as it relates to glomerular filtration rate is very complex and will be discussed further in a future post.
To illustrate lab value changes in transgender men, I’ll direct you to data that I found in a large study of over 300 transgender patients including about 80 transgender men. The completed manuscript is not currently available but will be printed soon:
However, this does not mean Cisgender male reference intervals are adequate for transgender men. This topic needs further exploration and ideally a prospective trial to be performed in a controlled manner. A double-blind study would not be possible as it would be unethical to perform.
References
Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. J Clin Endocrinol Metab. 2017
Wierkx K, et al. Cross-Sex Hormone Therapy in Trans Persons is Safe and Effective at Short-Time Follow-Up: Results from the European Network for the Investigation of Gender Incongruence. J Sex Med, 2014. 11(8):1999-2011.
Mueller A, Kiesswetter F, Binder H, Beckmann MW, Dittrich R. Longer-term administration of testosterone undecanoate every 3 months for testosterone supplementation in female-to-male transsexuals. J Clin Endocrinol Metab. 2007
Paller CJ, Shiels MS, Rohrmann S, Menke A, Rifai N, Nelson WG, et al. Association Between Sex Steroid Hormones and Hematocrit in a Nationally Representative Sample of Men. J Androl. 2012 33(6): 1332-1341.
Fernandez JD, Tannock LR. Metabolic Effects of Hormone Therapy in Transgender Patients. Endocr Pract. 2016;22:383–8.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
A 56 year old male presented to his PCP complaining of sinus congestion, rhinorrhea, night sweats, decreased appetite and fevers of up to 101-102 every evening. Hematologic evaluation revealed a neutropenia and a lymphopenia. An infectious disease work up was negative. His LDH was elevated. Physical examination reveals an enlarged left axillary lymph node. An excisional biopsy was performed.
Biopsy Findings
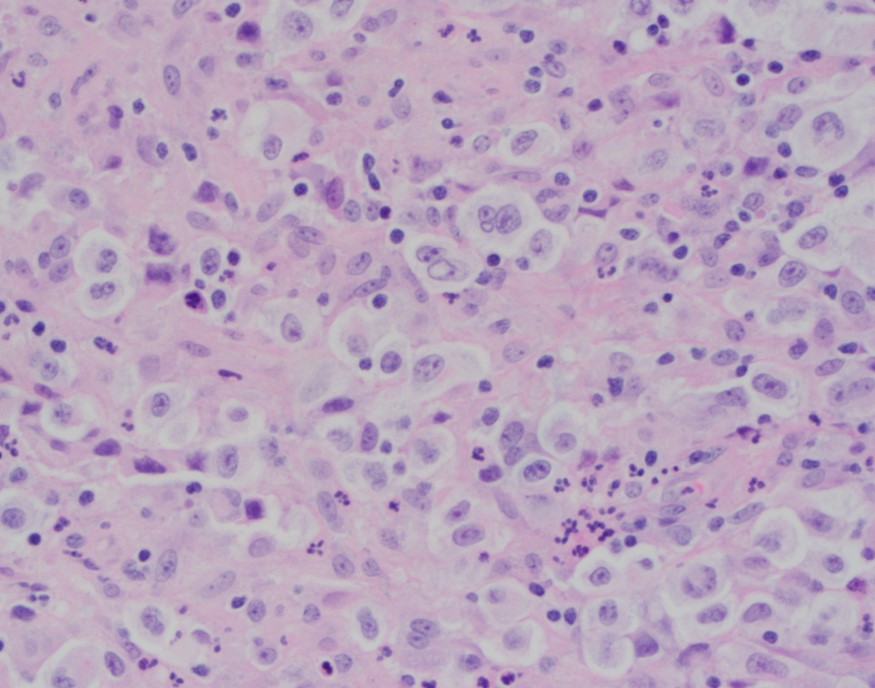
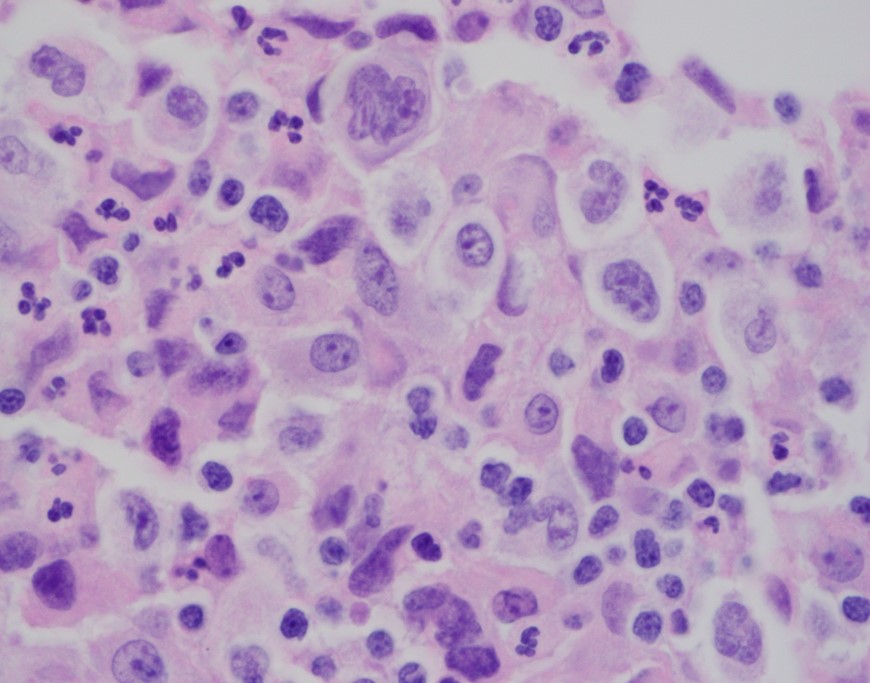
H&E stained sections demonstrate an enlarged node with effaced architecture and scattered residual follicles with small, mature cells. There is a proliferation of intermediate to large, to very large, atypical and highly pleomorphic cells many of which demonstrate bizarre forms, irregular nuclear morphology and acidophilic nucleoli. The lymphoma cells are noted to focally traverse through adipose tissue. Occasional hallmark cells are appreciated.
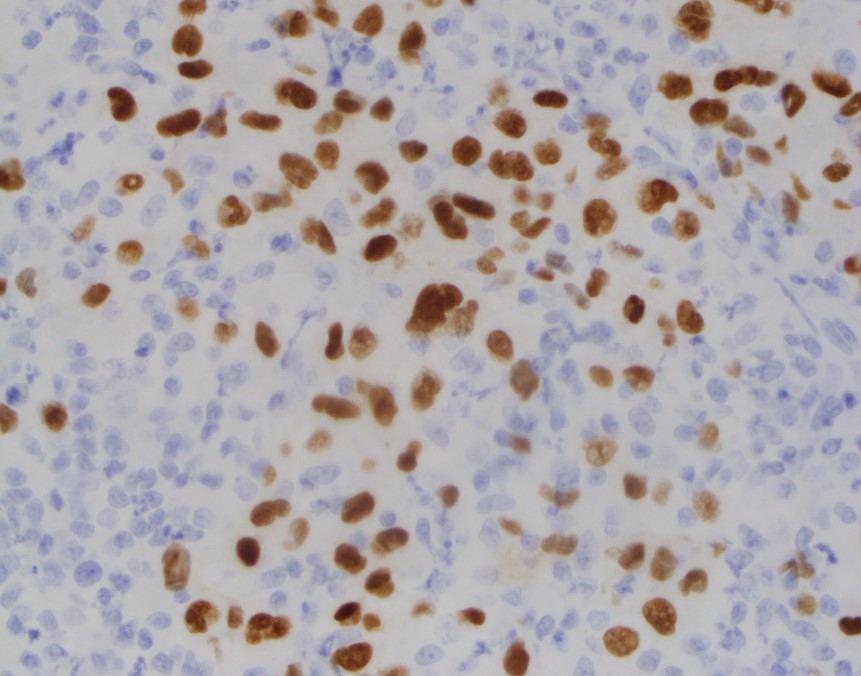
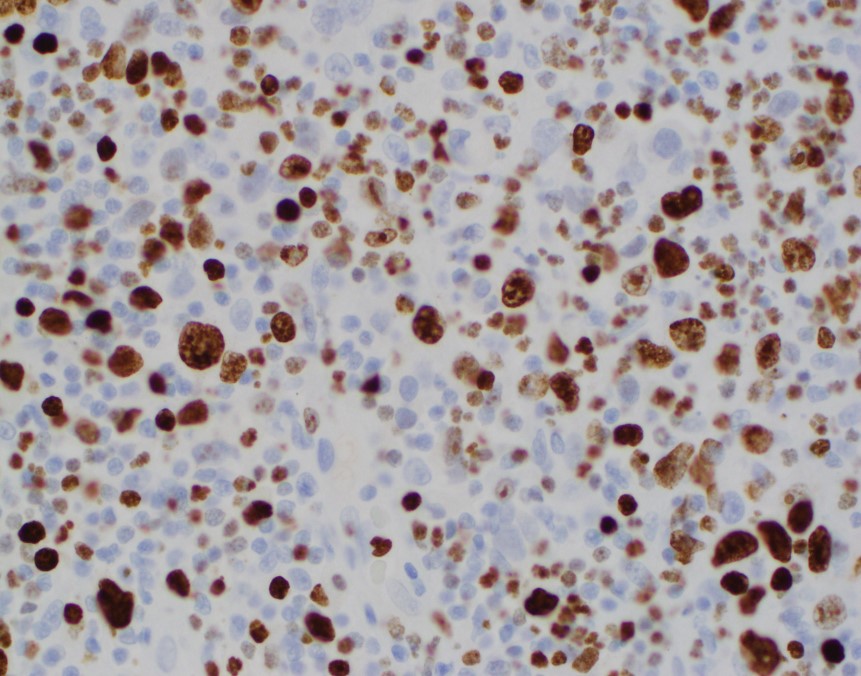
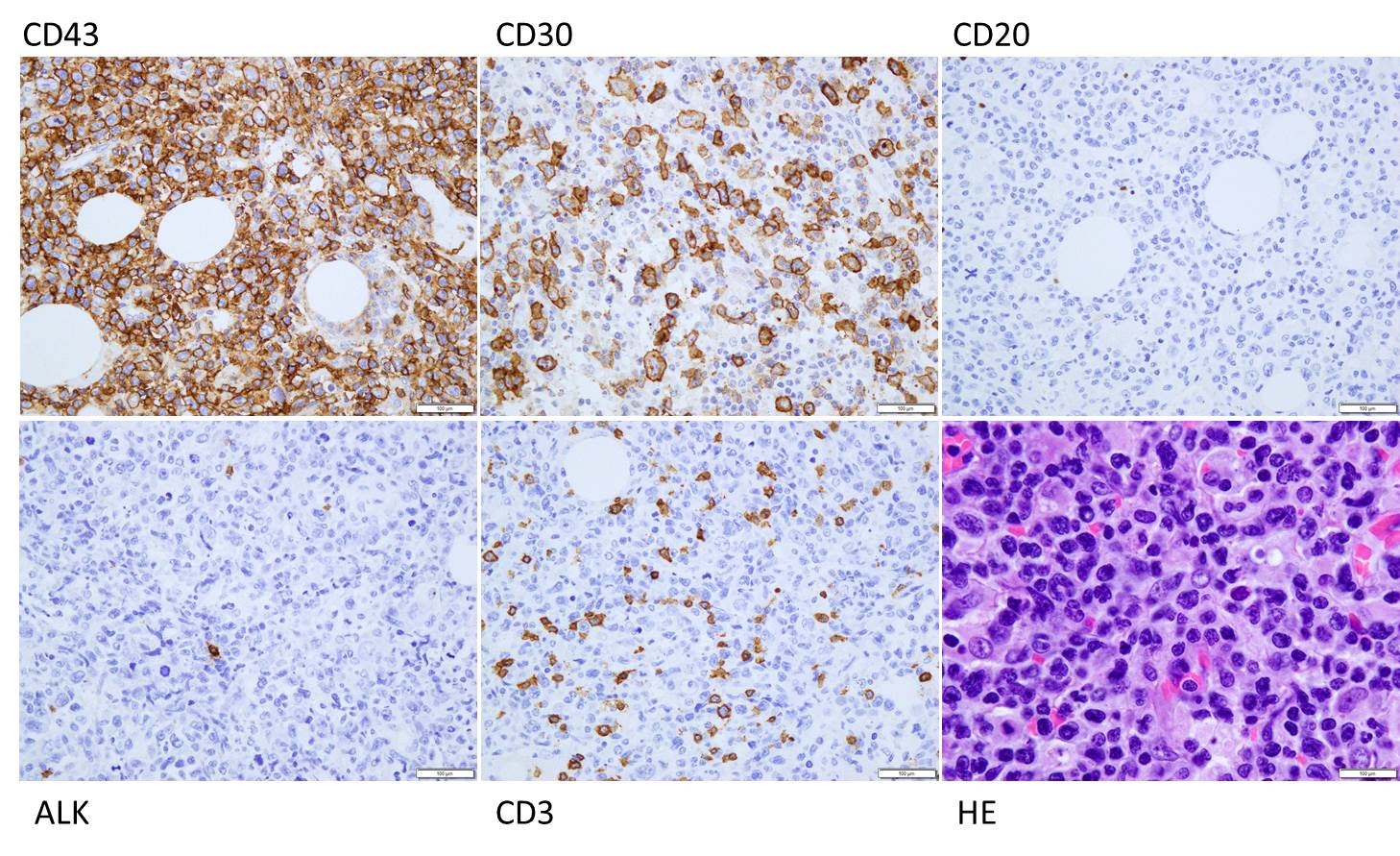
To further characterize the infiltrate, immunohistochemical stains were performed and interpreted with appropriate controls. The lymphoma cells were diffusely positive for CD45 (LCA), CD43, and CD30 (membranous and Golgi) with a Ki-67 of 80-90%. These cells were negative for CD20, PAX-5, CD3, CD4, CD8 (mostly), CD5, D10, BCl-2, BCl-6 and ALK1.
The morphologic features and immunophenotype of the cells was diagnostic of anaplastic large cell lymphoma, ALK negative.
Discussion
Anaplastic Large Cell Lymphoma (ALCL), ALK-negative (ALK-) is defined as a CD30+ T-cell neoplasm that morphologically resembles ALK-positive ALCL, but lacks ALK protein expression. It most commonly affects adults (aged 40-65 years), and has a slight male preponderance with a male-to-female ratio of 1.5:1. T. Most patients present with advanced disease (stage III-IV), lymphadenopathy and B symptoms. The most common differential diagnosis is ALK-positive ALCL.
The molecular deciphering of ALCL began in the 1990s with the discovery of a recurrent t(2;5) (p23;q35) translocation fusing the ALK gene and the nucleophosmin gene generating a NPM-ALK fusion protein, as well as other ALK translocations resulting in a high ALK kinase activity. This triggers the major oncogenic pathway in ALK-positive ALCL. Pharmacologic therapy has been developed to target ALK, and has shown efficacy. Thus, compared with ALK-negative cases, ALK-positive occurs in younger patients and has a better prognosis. ALK-negative ALCL also tends to involve both lymph nodes and extranodal tissues, although extranodal sites are less commonly involved than in ALK+ ALCL.
The other differential diagnoses of ALK- ALCL includes, primary cutaneous ALCL (C-ALCL), other subtypes of CD30+ T-cell or B-cell lymphoma with anaplastic features and classic Hodgkin Lymphoma. If a single lymph node or cutaneous cases are suggestive of ALK- ALCL, C-ALCL needs to be considered. Any cases that involve the gastrointestinal tract need to be distinguished from CD30+ enteropathy-associated and other intestinal T-cell lymphomas.
Molecular analysis of ALK- ALCL shows characteristic strong expression of CD30, in equal intensity in all the cells. Loss of T-cell markers is frequently seen, however, more than half of all cases express one or more T-cell markers. CD2 and CD3 are more commonly expressed than CD5, and CD43 is almost always expressed. CD4+ is frequently positive, while CD8+ is rare. Many cases also express cytotoxic markers TIA1, granzyme B, and/or perforin.
The genetic profile in ALK-negative ALCL has been found to be pretty heterogenous. Most notably, activating mutations of JAK1 and/or STAT3 have been shown to lead to activation of the JAK/STAT3 pathway. Chromosomal rearrangements of DUSP22 (i.e. chromosomal rearrangements in or near the DUSP22-IRF4 locus on 6p25.3) occur in 30% of the cases, and rearrangements of TP63 occur in about 8% of cases. Neither of the rearrangements have been reported in ALK+ ALCL.
From a prognostic standpoint, studies have shown that the rearrangements have effects on the survival rate. TP63-rearranged cases were shown to have an unfavorable prognosis worse than ALK- ALCL with neither rearrangement, while DUSP22-rearranged cases were shown to have favorable outcomes similar to ALK-positive ALCLs.
References
Gaulard P, de Leval L. ALK-negative anaplastic large-cell lymphoma. 2016 Jan 14;127(2):175-7.
Edgardo R. Parrilla Castellar et al., ALK-negative anaplastic large cell lymphoma is a genetically heterogeneous disease with widely disparate clinical outcomes Blood. 2014 Aug 28; 124(9): 1473–1480.
-Brandon Zelman is 4th year medical student at the Philadelphia College of Osteopathic Medicine and an aspiring pathologist. You can follow Brandon on Twitter @ZelmanBrandon.
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
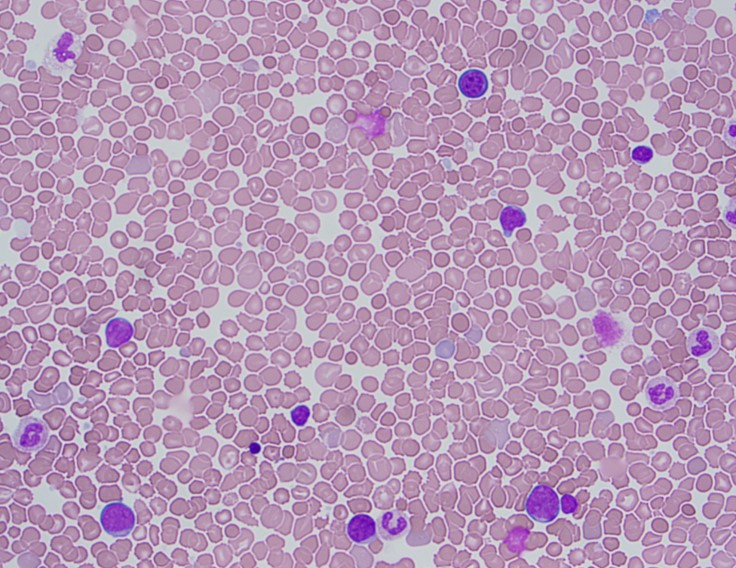
The patient is a 1 day old baby boy born at 39 weeks to a 44 year old woman. On physical examination, the baby had a mildly flattened occiput with thickened nuchal skin, downward slant of palpebral fissures with epichanthal folds and slightly low set ears. On imaging, he had a ventricular septal defect. A CBC was performed which revealed a white count of 34.2 K/uL with a differential that included 37 blasts.
Peripheral Blood Smear
Cytogenetics
Diagnosis
The peripheral blood showed an increased white count, many nucleated red blood cells as well as a population of blasts. The cytogenetic analysis confirmed the suspicion of trisomy 21. Flow cytometry showed that the population of blasts expressed myeloid as well as erythroid and megakaryocytic lineage specific antigens. The patient was found to have a GATA1 mutation. Approximately one month after birth, the patient’s white count normalized to 7.2 K/uL with only 4 circulating blasts counted.
Discussion
In a patient with trisomy 21, this presentation is consistent with a diagnosis of transient abnormal myelopoiesis associated with Down syndrome (TAM). TAM occurs in 10% of newborns with Down syndrome. Patients typically present with cytopenias, leukocytosis, an increase in blasts and hepatosplenomegaly. Less commonly, patients can have respiratory distress, bleeding, skin rash or jaundice. The blasts are morphologically and immunophenotypically similar to those seen in acute myeloid leukemia. They often have basophilic cytoplasm, coarse basophilic granules and cytoplasmic blebbing, which suggests a megakaryocytic lineage. The immunophenotype generally includes expression of myeloid markers such as CD117, CD13 and CD33 plus erythroid and megakaryocytic markers like CD41, CD42b and CD61.1
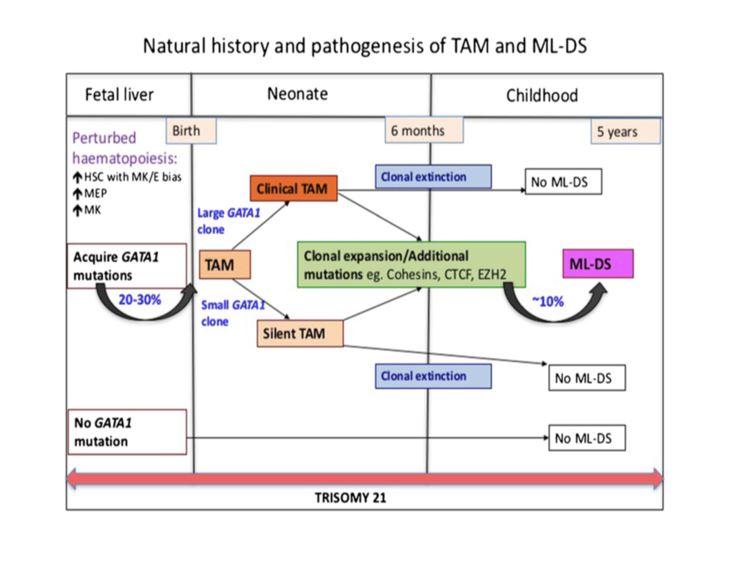
In addition to trisomy 21, mutations in GATA1 are almost always seen in the blast cells of patients with TAM. GATA1 is a hematopoetic transcription factor. Bhatnagar, et al. (see diagram below) describe a three step model to explain the evolution of TAM. The initial event is abnormal hematopoesis in the fetal liver caused by trisomy 21. This causes an increase in megakaryocyte-erythroid progenitors in the hematopoetic stem cell compartment. The second step is the acquisition of an N-terminal truncating GATA1 mutation before birth. GATA1 is a regulator of normal megakaryocyte and erythroid differentiation. The truncated mutation causes marked expansion of megakaryoblastic progenitors.
TAM has a high rate of spontaneous remission and typically resolves spontaneously in 90% of patients over several weeks to 6 months. This coincides with extinction of the GATA1 clone. However, in around 10% of these patients, myeloid leukemia of Down syndrome (ML-DS) develops within 5 years of the initial presentation. Additional mutations in cohesion component genes and epigenetic regulators occur in these patients that result in clonal expansion and non-transient leukemia. 2 Children who develop ML-DS generally have a good response to chemotherapy and a have a better prognosis than children without Down syndrome who develop AML.
References
Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues (Revised 4th edition). IARC: Lyon 2017.
Bhatnagar, Neha et al. “Transient Abnormal Myelopoiesis and AML in Down Syndrome: An Update.” Current Hematologic Malignancy Reports5 (2016): 333–341. PMC. Web. 21 Oct. 2018.
–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.



























 TAM has a high rate of spontaneous remission and typically resolves spontaneously in 90% of patients over several weeks to 6 months. This coincides with extinction of the GATA1 clone. However, in around 10% of these patients, myeloid leukemia of Down syndrome (ML-DS) develops within 5 years of the initial presentation. Additional mutations in cohesion component genes and epigenetic regulators occur in these patients that result in clonal expansion and non-transient leukemia. 2 Children who develop ML-DS generally have a good response to chemotherapy and a have a better prognosis than children without Down syndrome who develop AML.
TAM has a high rate of spontaneous remission and typically resolves spontaneously in 90% of patients over several weeks to 6 months. This coincides with extinction of the GATA1 clone. However, in around 10% of these patients, myeloid leukemia of Down syndrome (ML-DS) develops within 5 years of the initial presentation. Additional mutations in cohesion component genes and epigenetic regulators occur in these patients that result in clonal expansion and non-transient leukemia. 2 Children who develop ML-DS generally have a good response to chemotherapy and a have a better prognosis than children without Down syndrome who develop AML.
