When I was approached about writing an essay about our rural lab, I was initially stymied. There’s a universality about the work we do; tech work is pretty much the same wherever you go. A differential is a differential in the biggest cities and smallest towns. The thing that makes us unique is that we’re 50 miles from a city with a full-service hospital and many of our patients are elderly and don’t drive, so we try to cobble together as much care as we can give them in a clinic setting.
Our clinical laboratory is a small independent lab in Cairo, IL, midway between Memphis and St. Louis. We are attached to a regional system of rural clinics that provides care for the residents of the poorest counties in Illinois. We are the only high-complexity FQHC lab in the country, and we’re extremely proud of the work we do with our limited financial and geographical resources.
Our part in battling the COVID-19 pandemic feels a little odd compared to the work of hospital labs. We see our job as keeping our patients out of the overburdened hospitals for as long as possible. We screen everyone who presents with a fever for flu and strep. That includes the prisoners from the two local prisons, the nursing home patients in all the small towns scattered around rural southern Illinois, the teachers, daycare and home health workers. The criteria for a C-19 test is still very stringent in Illinois and most of our patients don’t yet meet it. We generally send them home with free samples of over-the-counter palliative meds, instructions about avoiding other people, and what new symptoms they should watch for.
Even so, we’re running low on basic supplies: PPE, swabs, disinfectant, etc. Like everyone else, we’re having trouble finding more. Yesterday I took a couple of hours to open every cabinet and paw through every box, hunting for overlooked supplies. There was a stash of sixty N95 masks in a closet and forty painter’s masks left over from when the lab was built. The box claims the masks “have N95 properties”…whatever that means. Hopefully we won’t have to find out. I distributed the N95 masks to the clinics that were running low and traded a box of disposable lab coats to our local clinic for 3 hazmat suits for our lab staff. I sent a few dozen more nasopharyngeal swabs to the prison with instructions to use them sparingly. We’re currently backordered until mid-April for more.
All the techs I know (locally and all around the country) are pretty fatalistic about this. We expect to be infected. We’re hoping it’ll be later rather than sooner and we’re trying to protect our more medically fragile and/or elderly colleagues. As you probably know, the average age of MTs in this country is about my age…56. A new virus brings attention to the medical lab profession, and that causes a brief uptick in new interest in our field, but we’re chronically understaffed and techs are retiring faster than we can train new ones to replace them.
In the meantime, of course, we continue to test and treat our regular patients. Mostly poor, mostly elderly, for the diabetes, hypertension, cardiovascular diseases and cancers that are the meat and potatoes of rural health. The concession they’ve made to social distancing is that less of them hug me, although a fair number say “If it’s my time, it’s my time” and hug me anyway. Many of our patients don’t drive, and they arrive one by one on the transit vans designed to seat 12 that pick them up from home. I wonder if the van driver disinfects between patients. I wonder if the patients know he ought to. I assume they hug him, too, so it probably doesn’t matter. This coronavirus crisis will eventually wind down, but the ongoing needs of medically underserved rural communities will continue unabated. Our hope is that this pandemic shines a big light on the many challenges of providing quality care to geographically large, sparsely populated rural communities.
-Evelyn Rubinas is a Medical Technologist at Community Health and Emergency Services, Inc. (CHESI) in Cairo, IL. She is a graduate of Southern Illinois University and the University of Arizona and has been a laboratory generalist for over two decades. She lives in Cairo, IL with her wife and a small menagerie of rescue animals.
I’ll get straight to the point this time: there’s a legitimate crisis happening in our world that is highlighting a multitude of things. Just to name a of few: the complex intersection of state-sponsored healthcare as a human right, the availability of resources to clinical personnel, the logistics and implications of public health measures to the average person, our global connectivity, and lack of damn tests!
And that’s our stop. Please take a minute to locate your exits, as they may be behind you, and get ready to talk about this SUPER CRITICAL aspect of the COVID-19 pandemic. What are clinical tests?
I know, this “viral” topic right now will be shared and spread to a vast array of audiences. So, I’m going to try something new here. The last four years of posts on this blog have been aimed somewhere between laboratory professionals and working clinicians. I open a rare window into our clinical world from time to time, but this pandemic is something affecting everyone. Today, we’ve got a major problem about what’s being said in the media and who understands which parts of it…so, as I discuss some major points below, I will take short pauses to highlight clinically relevant information as well as put things in plain, simple terms for all of us to get up to speed together.
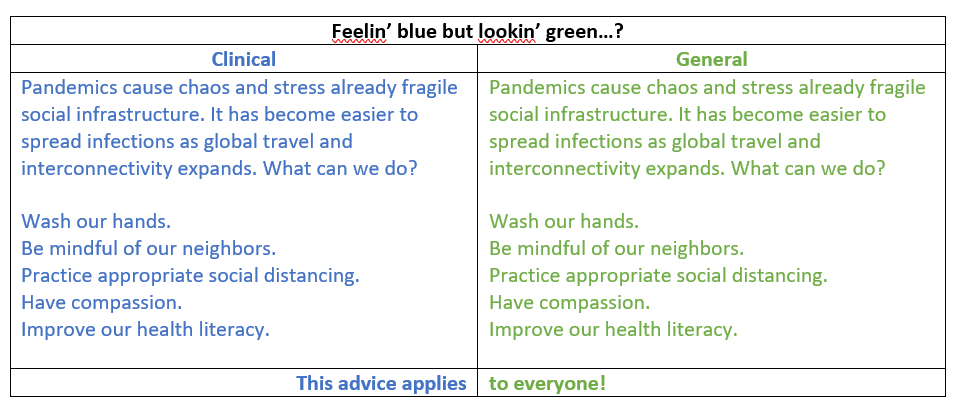
(If you are one of my clinical colleagues, from the bench to the bedside, your notes will be in BLUE. If you are not in the healthcare world, or just want some simple clarification, your notes are going to be GREEN. Let’s run an example so you can see what I mean…)
Image 1. I realize that there are people who ware blue-green colorblind, so if you have a hard time differentiating one from the other in this picture, I’ll keep the clinical/general labels. If you have no issues with these colors, the image above uses green to demonstrate where the coronavirus pandemic currently exists. Colorful humor? Fine, keep reading…
Last month I talked about the background and biology of the SARS-CoV-2 virus as a novel, emerging pathogen and potential pandemic and discussed how we must contextualize these epidemics with proper understanding of data and statistics. Numbers are important and if we’re going to combat a super bug, we’ve got to know what it is, how it acts, where it came from, and what’s happening in the field. A subsequent and fantastic post right after mine by Dr. SoRelle at UTSW, discussed how to validate a COVID-19 test in your laboratory. Basically, he presented a snapshot of the current climate of academic hospital labs now depending on LDTs to respond to the pandemic and discussed where to read more, what limitations testing might have, and how to address things like designing/purchasing primers, cross-reactivity, detection capabilities, and EUAs under the new FDA guidance.
But back to business, this month we’re talking about testing, and if you just google search “COVID-19” in the states, you’re met with a myriad of failure stories…
“As US fumbles COVID-19 testing, WHO warns social distancing not enough” (source)
“Limited access to COVID-19 tests frustrates patients, health professionals” (source)
“What went wrong with coronavirus testing in the US” (source)
“Why coronavirus testing in the US is so delayed” (source)
“America’s shamefully slow coronavirus testing threatens all of us” (source)
Image 2. This novel coronavirus pandemic has caused another pandemic of fake news. Fake cures, misinformation, false panic, mistrust, and a whole mess of non-scientifically accurate claims that have slowed the responses of public health officials in China, Italy, and even here. (Image source: BBC)
I’ll stop torturing you. You’re forced to watch and/or read enough news as it is nowadays (you’re social distancing, right? …right?) I mean, even Norway took a jab and called us “underdeveloped” citing our poorly developed healthcare delivery system—ouch. So, what’s the big problem with testing? What stark revelation exists between all these different news sources and highlights our “laboratory failures” in America? Well, luckily nearly all of these lab-fail stories aren’t aimed at our labs at all, they’re aimed at governmental decisions and red tape traps. But that’s hard to get to in a sea of clickbait. So instead of giving you more rabbit-hole lab talk, let’s talk about two main tenets of this narrative that everyone should be aware of: what laws affect lab tests and what does it mean to create a new lab test? After we clear the air for those two key points, we’ll come back around and tell you what COVID-19 looks like in the medical laboratory.
The Law of the Lab
There are SO MANY regulations and accrediting bodies that govern the way labs operate, deliver results, and function in clinical settings. Let’s name some! Various federal, state, and local laws ensure the highest calibers of safety and accountability for clinical and research laboratories; laws from OHSA, the FDA, recommendations from the CDC and local health departments; regulations for mechanical, noise, chemical, exposure, pathogen/infectious safety, pollution, radiation, blah blah blah! Trust me, there are a ton. What feels ever present to us laboratorians are the accrediting and inspection agencies that grant us authority to continue performing our clinically vital roles. Joint Commission, FDA, and other inspections make sure hospitals are up to snuff. Laws that govern what labs can do what tests fall under CLIA. They help us define high complexity to waived (not complex) testing. There’s a massive difference in a clinical office’s medical assistant obtaining a point of care (POCT) glycated hemoglobin (Hgb A1c) than a medical laboratory scientist conducting a hemoglobin electrophoresis study, and that difference highlights specialized training, laboratory ability, safety and quality requirements.
Image 3. I know we’ve had this debate a few years ago, but your average nurse probably couldn’t help too much with a bone marrow aspirate evaluation or running quality control on the chemistry analyzers before morning run. Just the same, I remember being an MLS and I wouldn’t have been the most confident IV or foley catheter placer…now I have the distinct pleasure of living in both worlds. Yay. Bottom line: the laboratory, and de facto the hospital, COULD NOT FUNCTION without the team of medical laboratory scientists that make its wheels turn! (Image source: labtestsonline.com)
Accreditations and recommendations can come from many professional societies like the CAP, ASCP, AABB, AACC, ASM, ASH, and many subspecialized groups. Laboratorian trigger warning: I’m a certified CAP inspector. No; you don’t have to put away your desktop coffee…for now. But I’ve certainly—along with all of you—been wholly immersed in the endless accreditation and regulation protocols we follow. We know exactly why these regulations exist and we should talk more about them, since they define our role as such a critical one.
Feeling Validated Yet?
Some of you lost a breath when I said CAP inspector. The rest of you may now spit out your coffee and run for the hills because I’m talking about VALIDATIONS. Rotating MLS students sometimes do their capstones or theses on validating a test or instrument, but we do them because that’s just a part of our job! So what goes into validating a test? The short answer: a whole lot. The long answer: a whole lot more! Let’s take PCR testing for example, it’s topical because we’re talking about COVID-19 testing and that’s the prime modality so let’s explore that validation.
Image 4. A LOT goes into validation. Lots of biostatistics. I know there’s labels, but let’s walk through this graph. The red line is the best line, good correlation with minimal errors. The purple/pink like is permanently off the red line, therefore its in constant error. The blue line represents errors associated with too much or too little specimen, maybe too little reagent, or some other ratio issue. The salmon line might be another test, or another method of the same test. What do you think? Is it a better test? A little sharper of a test, maybe more sensitive, should we use less specimen? Maybe just a drop or two—BAM you’ve been sued for running a sham lab test company. Trade in that black turtleneck, do not pass go, do not collect $200. A newly validated test, or a validation of a new method comes with BINDERS full of runs and analyses, not for the faint of heart. (Image source: AACC)
So, you want to add a qPCR to your lab’s test menu, eh? You first have to decide quantitative or qualitative. If its quantitative you’re in for a treat—yay statistical variant analysis! You have to prove applicability, practical application, specificity, sensitivity, efficiency, correlatable translation into useful clinical data. Detecting a number or degree of mutations? Make sure its accurate and precise (and repeatable). Buying commercial kits or making your own in-house assay? What about a qualitative test, just a simple yes or no. Easier right? Not really, you need to prove most of the same data and statistical soundness depending on methodology used, instrumentation, nature of variation, etc. AND: it all must be documented, proven, up to regulatory standards, and you better have a database FULL of data that proves your test works. Now, I have good news and bad news.
The good news: this is pretty routine, and pretty easy to follow even for simple new tests your incorporating from commercial vendors with ready-to-validate test kits. The bad news: COVID-19 is not this type of test. Say what you will about the US’s decision to NOT utilize the WHO testing model available weeks ago, the CDC responded in kind here by providing a two-control kit that SLOWLY started to break out. Using this as a model, many labs in academic hospital pulled the trigger on their LDT work. (LDT = laboratory developed tests) I’ve already revealed myself as a CAP inspector (pshh, not even my final form!) and I can tell you that there are hundreds of citations for how to validate already existing tests, compare tests across different instruments, compare them across the same instrument, prove your statistical ability to ensure quality results, and even how to make your own test from scratch! Talk about extra work!
Image 5. [MLS]: You’re a good analyzer, a smart analyzer. We all appreciate your efforts and you’ve really contributed to a positive work environment. We appreciate you, so we got you these reagents. They’re nice and fresh, what do you think? [Instrument]: *BEEP* *BEEP* *ERROR* *MORE VALIDATION REQUIRED*, [MLS]: okay, okay, have you lost weight?…**RESULTS VERIFIED** (Image source)
Running COVID-19 testing alongside B. burgdorferi: Corona…with Lyme?
Now we’ve come to the heart of the current discussion. Dr. SoRelle talked about validating a COVID-19 assay last month, so I’m letting him take point on that—read his piece, its great! What we’re talking about today is what exactly regulations and validations have to do with COVID-19 testing. Remember the regulations that say how laboratories run tests and operate clinically? Okay, well there are issues with this narrative. You’ll see plenty of news stories about the regulatory red tape that has hindered lab professionals from providing COVID testing. This makes it sound like because of “rules” we just can’t give them out to everyone, or we can’t set up testing for whatever regulatory reason. This is not the case. This is how the relationship between those aforementioned regulatory bodies work. The FDA makes sure labs operate up to federal standards and, and specifically, enforce regulations outlined in CLIA. While the FDA would like to call tests/results products of analyzers/devices to fall in their prevue, the interpretation and translation of that clinical data is not a print out but a MEDICAL SPECIALTY—hi, I’m pathologist #2465827, part of the FDA regional lab result response team—nope. Lab developed tests (LDTs) are not FDA products, but CLIA certified processes that only CLIA certified laboratories can perform. No CLIA no LDT—it’s as simple as that. You now understand that a lot goes into a single test, and that not every lab can perform high-complexity testing, thus, not every lab is CLIA certified to do LDTs… which means no COVID testing for them.
Image 6. It’s not that there aren’t enough tests. Like we ran out or something. This very fast global pandemic happened and pulled the rug out from under us. Because of a number of challenges, we’ve just been behind developing a NEW test for a NEW bug. And we’re catching up quick, but like ASCP addressed their concerns to the White House, we are in need of resources and support. Vendors can’t just jump in and help because THEIR hands are tied by the FDA even if they have readily available test kits. Other countries have done better than us, and we can still do better. (data as of 3/14/2020, source: AEI)
Okay, the other half of the narrative says that because of a lack of supplies from industry vendors, commercial kits were unavailable either from them or the CDC and if they got them, their reagents were not good. Frustrated, scorned immunology/chemistry lab specialists decide, “we’ll show them…we’ll make our own test! *evil laugh*” A bit dramatic, because it is dramatic. That’s not how LDTs work. How, then, do we get to LDTs? That answer is simple: regardless of politics, resources, or any other social concerns, medical laboratorians and clinical pathologists are part of the essential healthcare team that strives to care for the sick and hopes to prevent unnecessary infection or illness. We’re in this together and if one system can’t provide tests for the whole country, hundreds of thousands of hospitals will rise to the occasion and share partial LDTs or create their own. Just like with any other test, labs know full well how to get this done and work together to do it.
But what about the stories that say some tests take 8 hours vs others that take 4 days to turn around results? How come some kits came with 2 swabs, and some with 3? Why did other countries like South Korea do a lot better than us in testing their population? Did we wait too long to set up LDTs? Can’t I just go to my doctor and get tested now? Okay, okay, I hear you. This is where it gets heavy, especially in the media. The takeaway can be a simple comparison: look back to the Zika epidemic. Zika is an Arbovirus/Flavivirus that we knew about for roughly 60 years. As such, we had time to understand it and create tests quickly that measured exposed patients’ antibody response to acute or resolved infections. Even simpler, Zika is part of a family of mosquito-borne illnesses that we generally understand pretty well. SARS-CoV-2 is not like Zika. The word “novel” is used because it’s just that: brand spankin’ new. And, even though it’s a cousin of its predecessor in the old SARS epidemic, we’ve been racing the clock to create accurate and reliable testing. That’s why there’s so much variability happening across commercial industry to academic hospital laboratories.
Image 7. We’ve got a lot of work to do. At a rough estimate there are roughly 6000 cases of confirmed COVID-19 in the US, and we’re only testing that much…we can’t even collect this data fast enough. This is was scares most healthcare people, myself included. (Source: Medscape)
Pandemic Proportions
I love to make puns but let me be clear: this is a serious global pandemic, as defined by the CDC and WHO and we must understand this fully and appropriately. We’re still in the dark about a lot of data, mostly because of missing numbers. What we do know continues to inform our daily-changing climate of public health awareness in the US. The following images speak for themselves and I’ve collected them as a resource and snapshot for you to look through, just to get your SARS-CoV-2 bearings.
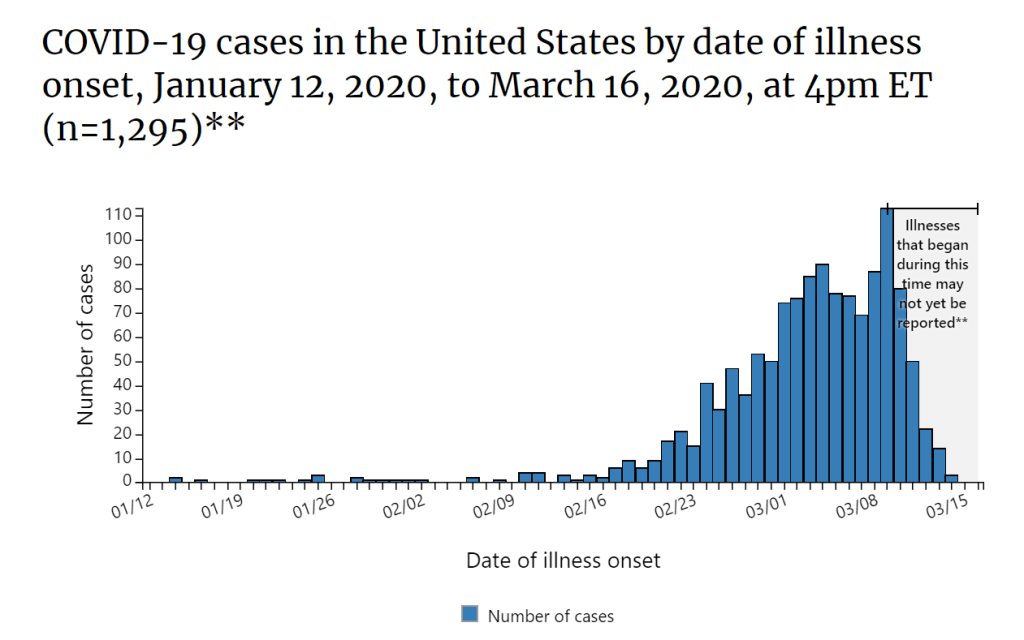
Image 8. If you haven’t yet locked this into your computer desktop, this dashboard from Johns Hopkins pulls data from various trusted sources (WHO, CDC, ECDC, NHC, and DXY) and local info to create a live, updating dashboard to follow along with the pandemic. (Source)Image 9. I posted these for my pieces on Zika in Sint Maarten, so let’s not be strangers to the epidemiological week graph. Take note, after the first week of March 2020, things get messy. Read: the great lab test debacle. (Source: CDC)Image 10. This is an uncomfortable graphic. Outside of China, the worse of the (then labeled) epidemic was Italy. Fast forward, we’re in full global pandemic mode and we’re starting to overtake the Italians a bit with cases detected/reported over time. Living, breathing, coughing data. (Source: @elipariser on Twitter)Image 11. Could I write a piece about literal lab testing and ignore this gem of a post from @TrustMeImAMedTech ? No, I could not. Very cool, clinical snapshot of an average COVID-19 patient’s labs based on data from a Clinical Chemistry Lab Medicine article from this month.Image 12. The UCSF ID working group established a diagnostic profile of a suspected COVID-19 infected patient. Anecdotally, I’ve read about cases that present with lymphocytopenia or lymphocytosis, the latter of which may correlate to prognostic factors. (Source: J Babik, UCSF)Image 13. What? I’m still on Reddit. There’s always good stuff on there. This post by u/RadOncDoc shares intensivist Dr. Nick Mark’s take on acutely infected, critical COVID-19 patients. I’m reading and absorbing… (Source: reddit, r/medicine)Image 14. You’ve heard of #FlatteningTheCurve, what does this mean? If we do nothing, the daily number of cases increases dramatically. If we take measures to preserve the capacity of the health care delivery system (social distancing) we won’t over tax the ERs and critical care units that might be needed during this pandemic, thus, flattening the curve of daily cases. (Source: Vox)
What can I say? It’s hard to write a conclusion about something that’s changing every day. I’ve been doing my best editing to keep this as up to date as it could possibly be for publication, but there are a million more resources sitting in the queue that I wish I could walk you all through. But I think, at the end of the day, what we need to remember is one simple thing: we’ve been here before and we’ll be here again. Public health epidemics and our responsiveness is one of the more serious aspects of laboratory medicine and pathology, not to mention healthcare at large. I said it last month that we’re lucky that this isn’t an influenza-type virus, because that would look a lot different. There are still some highly serious infectious etiologies out there more lethal than COVID-19, but this pandemic is bringing to light a lot of public health awareness and an opportunity to examine our population’s medical/health literacy, our policy priorities, our strength and resolve, as well as our ability to adapt.
Image 15. If you have a few minutes, please watch this CNN clip from one of my friends, colleagues, and mentors discussing how to be safe and smart during this period of social distancing and compassion-informed protective changes! (Source: CNN, video here)Image 16. “I’ve never seen anything like this before,” said the pundit, reporter, bystander, and/or concerned citizen. The sad part is, they say it every time we have a public health crisis. The time is now to break the cycle and learn from the past. (@CEKanakisMD, #PathDoodles 2020)
In the coming days, weeks, months you’re going to most likely hear about municipal infrastructures cutting back on things in order to prevent the spread of the virus. Listen to these warnings and heed the advice of the medical community. If you think you’re being a hero by braving the storm, you’re no better than a mosquito that carries malaria with no symptoms itself. Wash your hands, practice appropriate social distancing, continue your daily life with your necessary trips out being mindful of what those of us in healthcare live with on a daily basis. Practice compassion as well, just because we’re social distancing to “flatten the curve” doesn’t mean its time for martial law and cleaning supply hoarding. I know these are serious times, but humor and compassion can be infectious too.
Thank you for reading.
Please remember to follow the most updated, verified, and trusted sources on this starting with the CDC and your local public health organizations.
Wash your hands. Change your clothes. Minimize exposures. Take time to reflect and keep as close to your normal routine as possible while remembering things will get better.
If you have specific questions, comments, or concerns leave them in the comments below. Feel free to contact me anytime, and follow my social media (@CEKanakisMD on Twitter) for more/updated material.
Take care, see you next time!
-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
While washing my hands in an airport restroom, “Until the End of the World” by U2 (Achtung Baby, 1991, Island Records) was playing over the toilet speakers. As I watched several people incorrectly wash their hands during this current pandemic, the songs lyrics (which I have known by heart since 1991) rang through my brain and struck a new chord with me. There are plenty of doomsday songs that actually make us happy (Prince’s 1999, from 1999, 1982, Warner Bros.; R.E.M.’s “It’s the End of the World as We Know It,” from Document, 1987, I.R.S. Records) despite the dark images in the lyrics. And then here are a whole host of doomsday songs that are dark and brooding (“Man Comes Around” by Johnny Cash, “Waiting for the End of the World” by Elvis Costello, “It’s Not the End of the World but I Can See it from Here” by Lostprophets, and “Preaching the End of the World” by Chris Cornell, etc.). It turns out you can write a doomsday song after a breakup with your partner (“The End of the World” by Skeeter Davis) or in response to nuclear war fears (“Everyday is Like Sunday”by Morrissey).
What struck me in my new feeling of U2’s track was the dichotomy of viewpoint by the two principal voices in the song. The speaking voice is in it for the short game, in it for “me.” The listener in the song is in it for the long game, in it for “we.” Considering both the inspiration for the song personally for Bono as well as the historical character about which the song is based, this might be kind of obvious to most of us. However, in 2020, as we face what can only be described as a venomous divergence of voices, the lyrics force me to think about individuals’ motivations, agendas, messages, points of view, and goals when they speak, text, post, or otherwise communicate their opinions and that such opinions come in two flavors. There are those that are in this for themselves. There is no other valid observation than selfishness, conceit, arrogance, and disrespect for others. There are those that are in this for everyone. There is no other valid observation than collaboration, caring, selflessness, humility, and respect.
Considering that, regardless of your moral compass or who your parents were, most children are theoretically raised to be like the latter but the innate, instinctive traits of our evolution are really the former. Thus, as many great philosophers and thinkers have concluded, the intellectual evolution of the human mind and personality is such that seeing and caring for “the other”, even more than for ourselves, is a mark of high achievement while base, crude attacks on “the other” are marks of devolved, unintelligent individuals. Notice that there is no good and evil in this argument. There is only awareness of self and awareness of others and choosing one over the other. Naturally, the best life is to balance our care for ourselves and our care for others, which, some would argue, is one of the most valuable aspects of organized religion. As I am a non-religious person—despite the fact that the U2 track is one of my favorites—I strive to achieve that balance through a universal moral compass perspective which includes a great deal of importance on the safety, security, health, well-being, and happiness of others.
COVID-19 and its viral cause, SARS-CoV-2, have sent incredible ripples, waves, and tsunamis across every aspect of human life in the last 6 months. Pandemic preparedness and responsiveness is a “we” activity. China very much had a “we” approach to health (among many other sectors) which was evident by their incredible response to SARS originally in 2002. Some would argue that had SARS emerged in any other country, it would have gone pandemic at a much faster rate with horrible consequences; yet, emergence in China meant the virus was facing a huge pre-programmed response. But importantly in the 2002 outbreak, CDC officials from the US were relocated to China and work closely with the Chinese government to plan, implement, and execute daily changes to the management of the outbreak. Relationships being what they are, China did not interact as closely with the US for COVID-19 and, thus, the response was not as successful. In healthcare, as in many areas of human life, we are stronger together, and we will be more successful with transparency and communication than with secrecy and seclusion. The health of humanity should not be a geopolitical issue.
The diagnostic medical team (DMT), composed of pathologists and laboratory professionals, is the backbone of modern healthcare. However, these are also people who have underlying conditions, have elderly parents, have to ride the train to work, etc. Everyday, even when there isn’t a pandemic, members of the DMT place their own personal health and safety on the line to provide patients with rapid, accurate diagnoses and continuous care. Fortunately, laboratorians are well versed in protecting themselves within the laboratory from potential risks; however, in a pandemic situation, they must also protect themselves from external risks, else the laboratory staffing falls below the levels that insure high quality patient care is available.
COVID19 testing by RT-PCR of SARS-Cov-2, for example, is a high complexity laboratory test that is often performed by a select number of laboratorians and not by all laboratory staff. When we hear discussions of laboratory testing for COVID and money for such testing or availability of kits, it must also be noted that the laboratory is the only segment in the system who can take money and tests and turn it into data that saves lives—but only if they have sufficient people to make this happen. Healthcare facility leadership and national leadership must support those teams by providing all necessary resources to meet the needs of patients including the laboratory direct and indirect needs. Expanding the ability of personnel in the laboratory to meet this emergent need through cross-training and potential emergency staffing coverages is essential to successfully navigating this pandemic.
The DMT is always practicing the “we.” But now that the pandemic requires transparency and communication for success, the entire health system must amplify the practice of “we” and advocate with external leaders for every member of the healthcare team, but especially the laboratories. It is no time for “me” in this situation. Hand washing, social distancing, and self-quarantine may seem like things that protect “me” but it is clear that the goal is rooted in protecting “we.” Flattening the curve may prevent the healthcare systems from becoming overburden; however, laboratories are going to be massively overburdened regardless. Asymptomatic, symptomatic with other diseases, and true cases of COVID19 all have to be tested and there isn’t a precedent for the pace the disease is moving. Laboratories are coming online this week (March 16th) with testing that needed to be available in January. Laboratory staff must be enabled and mobilized to meet this current needs. We are all behind the curve on this one, but I have full confidence in our DMTs to get this done if they can be supported. There will be struggle but the tenacity and perseverance of our nation’s laboratory professionals and pathologists will see this through to its end. Because we, the DMT, don’t have a choice but to always consider the “we” in our daily practice, our patients WILL BE tested and diagnosed. We will beat this together and in being together, we will be stronger.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
In the 1986 remake of the horror film “The Fly,” the character played by actress Geena Davis has a great line. When she warns another person about the extremely unsafe behaviors of the title character, she says, “Be afraid…be very afraid!” Clearly this woman in the story understands the dangers involved in hanging out with a man whose mind is slowly being dominated by a killer creature. As a lab safety professional, one of my greatest wishes is that laboratorians would understand the danger they can be in when they permit unsafe behaviors in those around them.
Coaching fellow lab workers about safer behaviors is perhaps one of the most powerful and important tools we have to improve the overall safety culture, but it is also one of the most difficult tools to use. There are a variety of reasons we don’t do well with speaking up when we notice unsafe activities. Some laboratorians are introverts, and saying something that could be perceived as forward or direct just isn’t natural for them. There are those who do not want to correct co-workers or friends since doing so might somehow damage the relationship. Others don’t say anything because doing so in the past had no noticeable results.
The damage done by not coaching others for safety is terrible, and unfortunately, it’s easy to do. Repairing this damage, on the other hand, can be a slow and difficult process. Albert Einstein said, “The world is not a dangerous place because of those who do harm, but because of those who look on and do nothing.” That means that when we see unsafe behaviors, we have a responsibility to do take action against them. Otherwise when we do nothing, we are essentially giving permission for those dangerous behaviors to go on. That will only lead to a worsening lab safety culture, and eventually there will be increasing amounts of injuries and exposures.
With the rapid spread of COVID-19 in the Unites States, the number of questions that have arisen about lab safety has climbed exponentially. I am excited about any uptick in interest in laboratory safety issues, but I wish it didn’t take a world-wide pandemic to cause it. The Centers for Disease Control (CDC) has offered very good lab safety instruction for the processing and testing of COVID-19 specimens (https://www.cdc.gov/coronavirus/2019-ncov/lab/index.html), and virus testing is being performed in more labs each day.
It is vital for laboratorians to remember this. While the coronavirus is not to be taken lightly, the patient specimens we handle every day contain biohazards that are far more dangerous to us than COVID-19. Hepatitis, HIV, select agents, and many other pathogens reside in the blood and body fluids processed and tested in laboratories across the country, and many of the illnesses these agents can cause are very hazardous to human health. I hope we remember that when the hype about this latest virus passes.
Use Standard Precautions when working in the laboratory. Wear lab coats, gloves, and face shields. When you see a co-worker who is not properly attired, offer them the PPE they need. If you see an unsafe practice like eating, drinking, or using cell phones in the department, end it quickly. That is how infections occur, and that is how they spread into the community. Remember, unsafe behaviors can have a direct affect on the safety of the entire team. The sooner we can help everyone to understand that, the better we will all be at coaching others. In the original 1958 version of “The Fly,” the title character is caught in a spider’s web. His famous (and often imitated) last words were, “Help me! Help meeeee!” The scientist practiced unsafe behaviors until it was too late to turn back. Don’t let that be the case for anyone in your laboratory!
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
According to this recently-published study in the Journal of Histotechnology, ” … experts are confident that 70% ethanol and 0.1% sodium hypochlorite should inactivate the virus. Formalin fixation and heating samples to 56oC, as used in routine tissue processing, were found to inactivate several coronaviruses and it is believed that 2019-nCoV would be similarly affected.”
The FDA is now democratizing the testing of the novel coronavirus: SARS-CoV-2 (the virus which causes the COVID-19 disease syndrome—I will call it COVID-19 from here on as that is the colloquial name most people know) by allowing high complexity testing labs across the United States. This move will permit more labs to test for COVID-19. A previous post by contributor Constantine Kanakis describes the biology of the virus, so I will not repeat that material. Instead, I will focus on some considerations in validating a Lab Developed Test (LDT) COVID-19 molecular assay.
The president of AACC, Carmen Wiley, said there are 11,000 high complexity testing labs in the US, which could qualify for performing this testing. However, not all of these labs have molecular and virology expertise, so others have placed the number of labs with qualified staff and instrumentation at 400.
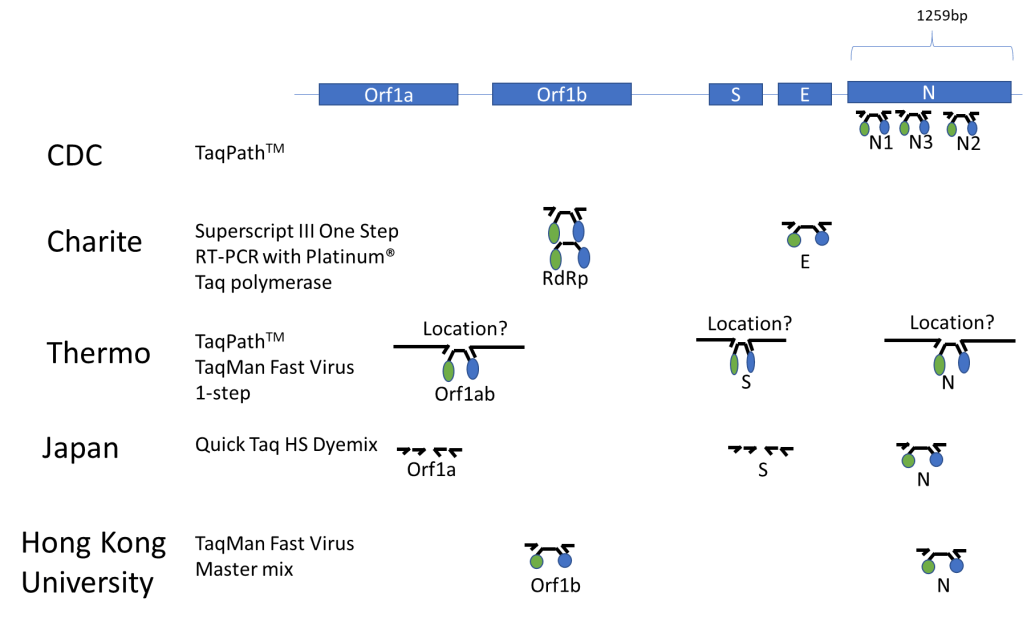
Published Assays and Targets: As an overview, the figure below (Figure 1) summarizes some published COVID-19 assays. As you can see, the major strategy involves using the TaqMan probe strategy where a short probe is degraded by Taq polymerase releasing a fluorescent molecule (green ball) from a quencher molecule (blue ball). The TaqMan approach allows for quick performance of the assay and easy interpretation. One lab from Japan is using nested PCR amplification and sequencing of the Orf1a and S genes as well.
Figure 1. The COVID-19 genetic structure is abbreviated above with the different genes targeted displayed. The names of institutions that have published their assay procedure along with the TaqMan reagents that were reportedly used with each assay are shown above. Primers are represented by small arrows with a TaqMan probe in the middle represented by a black line with green and blue circles indicative of the fluorescent molecule and its quencher. The double set of arrows for the Japanese assay represents a nested PCR strategy.
In silico Cross-reactivity:
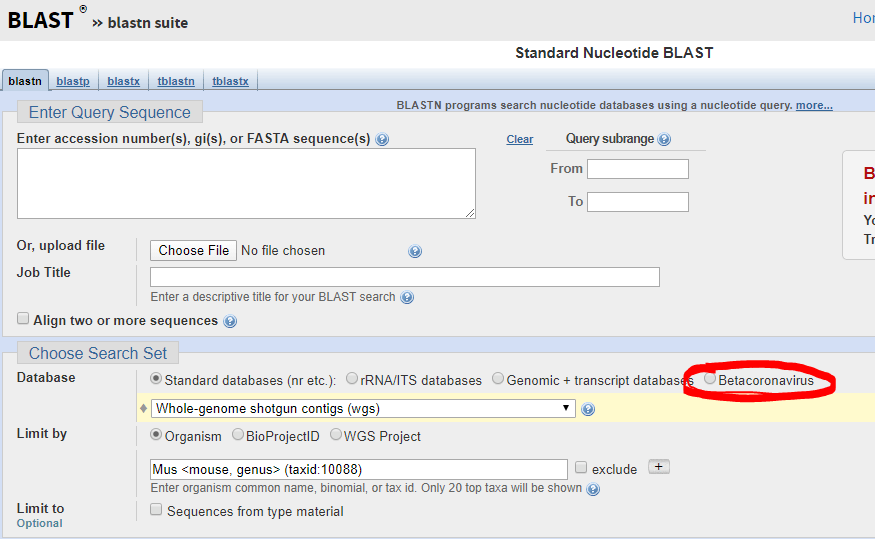
The FDA guidance allows cross-reactivity to be minimally assessed in silico by demonstrating “greater than 80% homology between primer/probes and any sequence present in the targeted microorganism.” The primer locations can be found in the publication of each protocol (except Thermo) and can be confirmed by checking the NCBI Blast site and they actually have a selection for beta-cornavirus (Figure 2) now that allows you to search for your primer’s reactivity across other related viruses- Very helpful!
Figure 2. Select Betacornavirus before entering your primer/probe sequence to confirm cross-reactivity.
Primer/Probe Design:
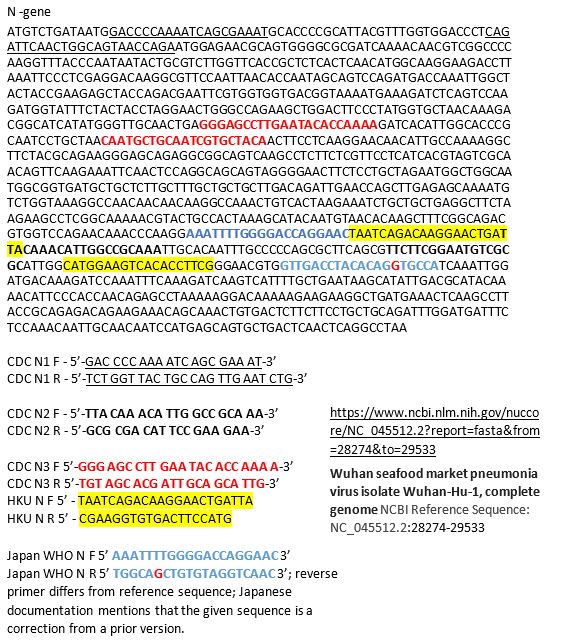
The N region is the most popular site to probe and is included in most kits once and the CDC kit three times. It was the reagent set for N3 in the CDC kit that was having difficulties, so you may decide to not include that component in your LDT. If you want to see how the different available primer sets align on the N gene sequence you can see below for the primers labeled based on their source. Many are overlapping, perhaps because many people thought the same site was a good target (Figure 3).
Figure 3. N-gene of COVID-19 along with labeled primers from some published assays. The information on the source of the sequence is shown on the bottom right with the link.
Commercially Available Assays:
An important part of validating your COVID-19 assay is to do so quickly. Thus commercially available kits would be helpful, however there are only two commercially available sources at this time: IDT and Thermo. IDT is producing a kit with the CDC design. Thermo produced their kit over the last few months and does not have any published validation information that I could find. Also Thermo when I checked just now for the catalog number, it says this product is unavailable… not sure what that means, but maybe you can try contacting them. Both IDT and Thermo list control plasmid reagents for their assays.
Controls for the Assay:
The wording of the FDA announcement was interesting in that it 1) did not require clinical samples, but allows “contrived clinical specimens.” “Contrived reactive specimens can be created by spiking RNA or inactivated virus into leftover clinical specimens.” A major difficulty is the access to actual COVID-19 RNA or inactivated virus. I noticed that the guidance didn’t say that the assay MUST use RNA. Thus most labs would have access to plasmid DNA, which could potentially be used.
Given the limited availability of RNA for validation use, a lab may consider performing much of the assay optimization with COVID-19 Plasmid DNA while waiting for access to RNA. I would like to be sure my assay could extract, amplify and detect RNA as part of the clinical validation.
Asuragen can produce Armored RNA, with synthetic RNA packaged inside of a viral capsid, which would be a useful control for extraction, amplification and detection. However, we heard this will not be available for another month.
Tom Stenzel (director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health (CDRH)) said FDA, BARDA, and the CDC will prioritize and coordinate shipments of viral materials to labs when they are ready to validate tests according to a webinar with labs on Monday. Currently, the FDA is directing inquiries to BEI, which is reportedly prioritizing requests to send out samples in 12-72 hours.
Lastly, one could try to use in vitro synthesized RNA sequences surrounding your primer targets as a control for now and may have better luck in getting the product soon. This is the control that is being shipped with the CDC kits to public labs.
Limit of Detection is an unknown for what is likely to be clinically relevant as we don’t know what the levels look like in people with early vs. late vs. severe vs. mild disease. The FDA just says you should be able to detect 95% of samples (19 of 20) that are x1-x2 the limit of detection.
FDA Notification:
This is the final and important step. Once you go live, you must notify the FDA with an Emergency Use Assay (EUA) form within 15 days. Reviewing the form, there doesn’t appear to have complex explanations or overdue requirements for reporting, which wouldn’t be found in a standard lab validation document.
Final Thoughts/Future commercial solutions:
This information is the best of what I know right now based on current information- this is not a complete guide and the FDA guidance should be read closely for all compliance details.Information is changing quickly and is likely to change more if the number of COVID-19 cases in the United States increases. Cepheid, Luminex, and BioFire are reportedly working on assays that will be out in several months and would be easy to use for many labs that already have one or both of these systems-however it may require a full validation for an LDT, but I’m not sure as it is an EUA-further clarification on this point is needed. Although there are several commercial solutions available, we don’t know how demand could impact supply from each company. Fortunately, some large reference labs like LabCorp and Quest are looking to develop a COVID19 test. Good luck, stay safe, and feel free to contact me with any questions in the comments below so that everyone can benefit from the discussion!
References
In lieu of a list of references, I’ve included web links for the most current and direct sources of information.
-Jeff SoRelle, MD is a Chief Resident of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and improving genetic variant interpretation.
The Food and Drug Administration (FDA) issued new guidance on February 29, 2020, for laboratories to be able to develop novel coronavirus (COVID-19) molecular diagnostics tests and begin use prior to obtaining Emergency Use Authorization (EUA). This permits laboratories that are CLIA certified and meet requirements to perform high complexity testing to start offering severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) molecular diagnostic testing after validation is completed as outlined in the guidance. Laboratories should submit an EUA request to the FDA within fifteen business days after validation. FDA will be hosting a webinar to provide more information on March 2, 2020, at 3 pm ET.
Clinical laboratories should contact their state health departments for guidance if they have a suspected COVID-19 case specimen. Clinical laboratories should NOT attempt viral isolation from specimens collected from COVID-19 persons under investigation (PUIs). For interim guidelines for collecting, handling, and testing clinical specimens from PUIs for COVID-19, please see the CDC Coronavirus Disease 2019 (COVID-19) website.
Patient advocates are simply people who care about patients as fellow human beings enough to act on that care. Forensic pathology fascinates many people, but hardly anyone realizes how strongly forensic pathologists advocate for patients.
Forensic pathologists have the responsibility of identifying human remains and determining the cause and manner of death for individuals that die suddenly and unexpectedly. Most often, we accomplish this mission by performing an autopsy. Death makes many people uncomfortable, and we’re accustomed to grim jokes about their work when meeting someone. Typically these comments carry an undertone that because decedents cannot talk, we don’t need interpersonal skills. Not only is this untrue, comments such as these provide an educational opportunity.
It is true that our patients have already died, but the relatives of our patients are very much alive. Those relatives have needs that we work to provide and questions we strive to answer. The most common question relatives have is “Why did my loved one die?” which is precisely what the pathologist is working to determine. We regularly talk with relatives of decedents that we’ve examined. We can tell family members why death occurred, including any implications that the death has for remaining members of the family. We can also help families begin to work through the social and bureaucratic requirements that death brings for those still living, such as the need to make arrangements for the disposition of the body and the need for a death certificate. (For example, after a person dies, that person’s financial accounts are frozen until a death certificate becomes available to unlock the accounts.)
Forensic pathologists work to develop a good relationship with the decedent’s relatives. Because anger and bargaining are part of grieving, conversations with relatives sometimes begin as though the relative and the pathologist are adversaries, but with time and compassion, the relationship usually transforms into a more appropriate professional relationship. A particularly important aspect of family interactions is listening to a grieving relative, because listening with care helps someone who is grieving. Attempting to build a good relationship with the decedent’s relatives does not mean that the pathologist is a blind advocate for the family. We won’t change the cause of death so that the family can reap more financial benefit from the death, for example. Lies will not help someone pass through the process of grieving in a healthy way – truth, time, and patient, loving care are the necessary therapeutic measures.
In the case of homicides, forensic pathologists advocate for the decedent by calling the death what it is and then testifying to the medical facts of that death when a suspect is tried in court. The pathologist testifies to the medical aspects of what caused death without trying to ensure that the suspect is either convicted or acquitted. Trying to sway the jury’s verdict is the work of attorneys; presenting the medical facts of why and how the decedent died is the work of the pathologist.
Forensic pathologists advocate for public health by providing an accurate cause of death. Death certificate data provide an essential component for assessing public health, and those data are an important determinant for allocation of medical research funds and for interventions to improve public health.
Like other pathologists, forensic pathologists typically do their work quietly in the background, advocating for their unique patients in their own special way. People give little thought to professional interactions with a forensic pathologist until forced to do so; in that difficult time we try to serve as best we can.
-Gregory G. Davis, MD, FASCP graduated from Vanderbilt Medical School and trained in pathology at Vanderbilt University Medical Center, Nashville, TN, followed by a fellowship in forensic pathology at the San Diego County Medical Examiner Office in San Diego, CA. Dr. Davis then joined the faculty at the University of Alabama at Birmingham, where he currently serves as a Professor and as Director of the Forensic Division of the Department of Pathology. Dr. Davis also serves as Chief Coroner/Medical Examiner for Jefferson County, Alabama, the county in which Birmingham is located. Dr. Davis has earned a Master of Science in Public Health from the UAB School of Public Health. His research interest is the application of epidemiology to the study and practice of forensic pathology, especially drug abuse. He has published 74 peer-reviewed manuscripts, including serving as lead author on the 2013 opioid position paper of the National Association of Medical Examiners. He is currently working as chair of a panel revising and updating the NAME opioid position paper for expected publication in 2020. He serves on the editorial boards of the Journal of Forensic Sciences and Forensic Science, Medicine, and Pathology. Dr. Davis is a Fellow At-Large Director on the Board of Directors of the American Society for Clinical Pathology.
The University Teaching Hospital of Kigali (CHUK) is the largest hospital in its District of Nyarugenge and the biggest national referral hospital in the country of Rwanda, with a 565 hospital bed capacity and 6 operating theaters. It is located in the heart of the capital of the country, Kigali, contributing to its easy accessibility by patients. Rwanda is a country of over 12.5 million people, with an estimated 70.2% of the population living in a rural setting. Per the World Bank, there is an estimated 1 physician per 10,000 people in-country. The government of Rwanda is focused on elevating the country from a low-income developing nation to a middle-income country with a robust health sector capable of ensuring a healthy people with adequate healthcare access. It provides universal healthcare, at a small cost, to all Rwandan citizens who aren’t provided health insurance through employment. In Rwanda there are a total of 14 practicing pathologists, which equates to approximately 1.1 pathologists per million people in the country. In contrast, within the United States there are an estimated 60 pathologists per million people. CHUK offers an array of outpatient, inpatient, surgical, and diagnostic medical services. Inpatient and outpatient services include surgery, accident & emergency, internal medicine, mental health, anesthesiology & critical care, gynecology, pediatrics, maternal & neonatology, ear/nose/throat, ophthalmology, neurosurgery, pediatric surgery, urology, nephrology, dialysis, oncology, and dermatology. Surgical services include general surgery, general pediatric surgery, neurosurgery, orthopaedics, ophthalmology, ear/nose/throat, and obstetrics/gynecology. Diagnostic services include ultrasound, digital x-ray, CT scan, and anatomic and clinical pathology services. In its current state, the hospital has a total of 18 divisions.
There are two facets to the pathology laboratory at CHUK: the Anatomic Pathology (AP) and the Clinical Pathology (CP) laboratories. Within the AP laboratory, also known as the histopathology laboratory, all surgical specimens are grossly examined by a pathology resident and/or pathologist, prepared by a pathology resident for processing, and processed by laboratory technicians into formalin-fixed paraffin-embedded tissue placed onto glass slides. These glass slides are then reviewed by both the pathology residents and the pathologists in order to render a diagnosis, which is communicated to the clinician in order to help direct appropriate patient management. Specimens reviewed at CHUK are predominantly “in-house” specimens generated by the surgeons and clinicians functioning within the walls of the institution. “Referral” specimens are a rarity and generally consist of small biopsies. Cytopathology specimens are also processed within the AP laboratory and include a mixture of fine needle aspiration (FNA) specimens, obtained by pathology residents via superficial FNA, as well as exfoliative cytology specimens such as effusions and urines collected by “in-house” clinicians. Cervical screening conventional pap smears are a rarity. Within the AP laboratory, Diff-Quik, Papanicolaou, and hematoxylin & eosin (H&E) staining was available for slides, as well as a limited panel of special stains: PAS-D, auramine, and a modified acid-fast stain. No immunohistochemistry was available on-site, though cases could be sent for free to nearby Butaro Hospital for IHC or consultation via digital slide scanning.
Regarding my experience at CHUK, I departed the United States on a Saturday evening and reached Kigali, Rwanda by 1AM the following Monday morning. On my first day at CHUK, I was introduced to the 5 anatomic pathology staff, 9 anatomic pathology residents, and the single visiting pathologist serving as a laboratory inspector conducting a mock inspection/assessment. I was given a tour of the pathology facilities as well as the entire hospital system.
There were two aspects to my primary job at CHUK: teaching the residents cytopathology and microscopic review of all live cytopathology cases received in the laboratory. Regarding resident education, there were four ways in which I interacted with the residents during my time to facilitate cytopathology education: lectures, multi-headed microscope unknown slide sessions (unknown case conference where I provided the residents with cases they had never seen before), multi-headed microscope “stump the chump” unknown slide sessions (where the residents presented me with unknown cases I had never seen before), and interactive practicals where we performed various hands-on aspects of cytopathology and general pathology practice.
In respect to lectures, I delivered a total of eight 1.5 hour powerpoint-based lectures covering the following topics: breast cytology, thyroid cytology, lymph node cytology, salivary gland cytology, urine cytology, effusion cytology, peritoneal washing cytology, and frozen section pathology (frozen section lecture presented as a combined effort with Dr. Raina Flores). For unknown slide sessions in which I presented cases to the residents, we had 6 sessions covering the following topics: breast, thyroid, salivary gland, urine, conventional pap, and cerebrospinal fluid. We completed a total of 5 “stump the chump” sessions, where residents gave me slides that I had never seen before and we discussed each case and its work-up as well as its associated differential diagnosis or final pathologic diagnosis at the multi-headed microscope. Topics covered included: breast, thyroid, salivary gland, lymph node, and effusions. Finally, with the assistance of “in-house” pathologists, I helped conduct 2 hands-on practicals with the residents: the first regarding fine needle aspiration technique and slide smearing technique (with Dr. Claire Nadyisaba) and the second regarding performance of frozen section intraoperative consultations using Leica CM1850 cryostats and cow liver (with Dr. Raina Flores).
The second of my duties, live cytopathology case review, was also performed at the multi-headed microscope with the residents each afternoon. On a given day, we would typically receive somewhere between 1 and 4 FNA consultations for which the residents would go to FNA clinic and perform the procedure. The laboratory also received various aspirated and exfoliative cytology specimens, such as pleural effusion and ascites fluids, from clinicians within the hospital system. In total, we reviewed 51 cytopathology cases together at the microscope. 27.5% were neoplastic, with 7.8% being malignant and 2% being lymphoma. 56.8% of cases were negative for malignancy, with 21.5% being inflammatory/infectious. In total, 9.8% of cases were interpreted as “atypical” and 5.9% of cases were non-diagnostic. Of the 51 cases, 21 (41.2%) were FNA consultations that I attended and the resident performed.
On my final day of work, I provided the residents with a 41-page cytology knowledge assessment (in PDF format) to complete at their leisure. This test covered the following topics: cervical and vaginal cytology (19 questions), urine and bladder cytology (11 questions), effusion cytology and peritoneal washings (13 questions), cerebrospinal fluid cytology (12 questions), breast cytology (8 questions), thyroid cytology (17 questions), salivary gland cytology (13 questions), and lymph node cytology (11 questions). Within the document, an answer key with associated detailed explanations was provided so it could serve as a learning aid/study guide for the trainees. On my last workday, the residents were asked to evaluate their experience with the Cytopathology Module/Course. A total of 7 of 9 residents completed the evaluation. Regarding preparation and organization of different topics, all residents found the quality of the powerpoints to be “very good” or “excellent”. The quality of the practical sessions was rated as “good,” “very good” or “excellent by all residents and the entire module was given an overall rating of “very good” or “excellent” by all of the residents. The majority of residents felt their time was used effectively during this module and that the venues for theoretical and practical learning were appropriate. In the free-text areas for additional comments, suggestions for improvement included a longer duration (at least 4 weeks) of the module, more hands-on practical time, the opportunity for residents to present information, and more microscopy sessions. For additional topics to be covered, respiratory cytology was suggested. In overarching comments regarding their module experience, the residents felt the module was well-prepared, the teaching sessions were well-organized, and that the course was interesting and helpful.
Finally, though not within the confines of my assigned “duties”, I also spent a portion of each day acting as “consultant” to the on-site pathologists for challenging surgical pathology cases, offering opinions as able for various lesions that were challenging to classify on H&E morphology alone. I also served as a “second reviewer” for new malignant diagnoses being rendered in the laboratory, offering my name to be included in the report as a board certified pathologist who has laid eyes on the case and agrees with the interpretation. Examples of some interesting surgical pathology cases I saw in “consultation” included Wilms tumor (nephroblastoma), cystic partially differentiated nephroblastoma (CPDN), pleomorphic xanthoastrocytoma (PXA), sinonasal undifferentiated carcinoma, basaloid moderately-differentiated carcinoma of the uterine cervix, high-grade large cell lymphoma of the cervical lymph node, high-grade squamous intraepithelial lesion of the vulva arising within a condyloma acuminatum, and low-grade papillary urothelial carcinoma of the bladder. I also attend a single Tumor Board Multidisciplinary Conference with two residents and 1 staff pathologist in which a resident presented a case of mucinous moderately-differentiated adenocarcinoma of the colon transmurally invading adjacent ileum. It was interesting to hear the clinicians, pathologists, and radiologists interact in addressing quality of care, efficiency of care, and clinical decision-making. The time of initial presentation to the time of surgery was greater than 1 year for this patient.
My time spent at CHUK in Kigali, Rwanda was an invaluable experience. The work setting granted me the opportunity to expand my role as an academic educator. I was offered the opportunity to present as many lectures as possible to the resident trainees, participate as the leader of multi-headed microscope slide sessions, serve as a spearheading physician in laboratory services expansion efforts, and work as an ‘attending’ physician overseeing trainees’ performance of FNAs. It was an experience that demanded personal growth, via the assumption of roles that I am not privy to as a post-graduate medical education trainee in the United States. Additionally, I was exposed to a cytopathology and surgical pathology workload for a patient population quite dissimilar from the community I am used to serving. With limited ancillary testing capabilities, I returned to a more “pure” form of rendering pathologic diagnoses, based on H&E morphology alone rather than on the synthesis of cyto- and/or histomorphologic appearance coupled with various ancillary diagnostic testing data points. In conclusion, this was an experience that expanded my understanding of the ways in which I can be useful as a board certified anatomic and clinical pathologist interested in incorporating medical mission work into my clinical practice. Beyond arriving in countries without expansive pathology laboratory systems and simply doing the work, I can also pursue opportunities where I can help educate and shape burgeoning in-country pathologists who will then go on to have productive, hopefully decades-long careers in their country, serving their countrymen. This trip certainly expanded my understanding of the role of a “visiting” pathologist. This experience was made possible by the ASCP Trainee Global Health Fellowship Award. Thank you so much to the ASCP, Dr. Dan Milner, Alpa Pandya, and the CHUK pathology department for helping to facilitate this opportunity!
Image 1. Dinner with CHUK pathologists and pathology residentsImage 2. Frozen section training with CHUK pathology residents Image 3. CHUK laboratory medicine building Image 4. CHUK hospital Image 5. CHUK hospital entranceImage 6. Small “downtown” area near CHUK hosptial–Kwibuka (“to remember”) memorial in remembrance of the 25th anniversary of the Rwandan genocide. Image 7. Overlooking Kigali. Image 8. Ferry ride to various neighborhoods in Kigali
-Kelsey McHugh, MD is a board certified anatomic and clinical pathologist, with cytopathology subspecialty certification, who is currently completing gastrointestinal, hepatic, and pancreatobiliary pathology subspecialty training. She anticipates graduating from the Cleveland Clinic Gastrointestinal, Hepatic, and Pancreatobiliary Pathology Fellowship in June 2020, after which she will remain at the Cleveland Clinic as a staff pathologist beginning July 2020.
































{kind=link}