A 28 year old female with a history of Ulcerative Colitis on humira and azathioprine presented with proctitis and a recent perirectal abscess. The patient reported a two week history of progressively worsening pain and swelling in the perianal region. In addition, she reported recent purulence excreted with bowel movements. On physical exam, the patient was afebrile and negative for rash, oral lesions, joint pain, or abdominal pain. A perirectal abscess was identified and drained. Abscess culture was positive. Patient reported recently engaging in high-risk sexual behavior with multiple male sexual partners often without protection.
Lab Identification
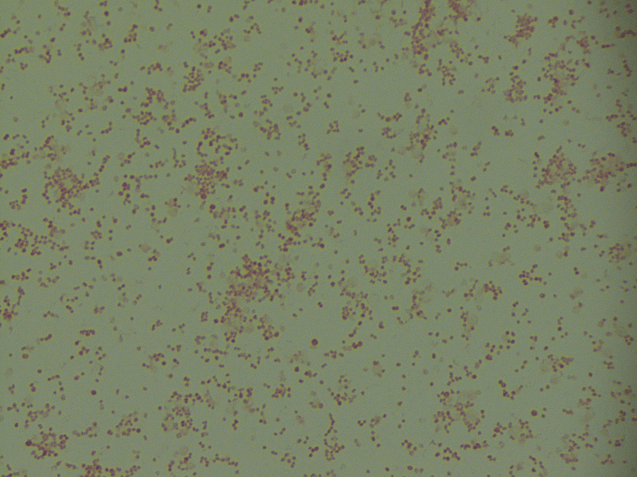
Image 1. Kidney-bean shaped gram negative cocci identified on Gram staining of perirectal abscess culture (100x oil immersion). Image 2. Aerobic growth of flat, gray-white, and moist colonies from perirectal abscess on chocolate agar plate.
Abscess culture grew kidney-bean shaped gram negative diplococci. Colonies on chocolate agar plate appeared medium sized, flat, gray-brown, and moist. The organism was oxidase positive and identified by MALDI to be Neisseria gonorrhoeae.
Discussion
Neisseria gonorrhoeae is a kidney-bean shaped gram negative diplococci for which humans are the only host. The organism causes gonorrhea, a common sexually transmitted disease, among young people between the ages of 15-24 years. Gonorrhea is spread by sexual contact or through the birth canal. The most common site of infection is the urogenital tract.2 Males commonly present with dysuria with penile discharge.2 Females commonly present asymptomatically or with symptoms such as mild vaginal mucopurulent discharge and severe pelvic pain2. In addition, gonorrhea can cause infections of the anus, conjunctiva, pharynx, ovary and uterus.2 In the neonate, the culprit organism can lead to ophthalmia neonatorum.2 Lastly, gonorrhea causes disseminated disease such as arthritis, endocarditis, meningitis, and skin lesions on extremities.2 CDC currently recommends treating gonorrhea with dual therapy, a single dose of 250 mg intramuscular ceftriaxone and 1g of oral azithromycin.1
Antibiotic resistance in gonorrhea is an increasing public health concern. The World Health Organization has a program that monitors the global antimicrobial resistance of gonorrhea.3 The data from 77 countries between 2009 and 2014 showed that 66% of reporting countries had encountered gonorrhea strains with either resistance or reduced susceptibility to ceftriaxone.3 81% of reporting countries had encountered gonorrhea strains resistant to azithromycin.3 Given these data, it is important to improve gonorrhea prevention and continue to monitor gonorrhea antibiotic resistance at both the national and global levels.
Miller KE. Diagnosis and Treatment of Neisseria gonorrhoeaeAm Fam Physician. 2006 May 15:73 (10): 1779-1784.
Wi T, et al. Antimicrobial resistance in Neisseria gonororheae: Global surveillance and a call for international collaborative action. PLoS Med 14(7): e1002344.https://doi.org/10.1371/journal.pmed.1002344
-Ting Chen, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
Traditionalists make up the smallest percentage involved in the current workforce, but they are the organizational historians as they know and remember the organization’s past and founding goals. Traditionalists are typically born between 1927 and 1945 and grew up during the Great Depression, which was from 1933 to 1938. After that, the second World War started and the U.S.A got involved after the attack on Pearl Harbor in 1941.
These years had a significant effect on this generation. Traditionalists are known to work collaboratively, know how to do more with less, and are task-oriented. They typically have a strong sense of what is right and wrong, which was fueled by the historical events in their childhood and early adulthood. They have a strong sense of patriotism and respect for authority figures.
This generation is also one of the first major innovators; they created space travel, vaccination programs, and the foundation for modern-day technological innovations. They were the driving force of the civil rights movement of the 50s and 60s and were also the ones that started moving to suburbs. Currently, the are serving on many Board of Directors, as Presidents of organizations or as executive leaders. They have generally moved up in the hierarchy of organizations that they have spent years working for. They are loyal employees who require little feedback from their managers.
Because this is the era of pre-feminism women, the majority of women raised children and only had a job before marriage as teachers, nurses, or secretaries. This generation is self-disciplined, cautious, and self-sacrificing.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
This generation was born before 1945 and is the oldest generation in the American culture. However, not all of those born before 1945 are alike. They either fought in WWII or were children through those war years. The Traditionalist generation are really the first strong innovators and if they are still working they act as the historians of the organization because they have been there for a long time. They often serve on Board of Directors and are Presidents because of their organizational knowledge and expertise. They are typically very disciplined, consistent in their behavior and opinions, and are known for their loyalty.
The majority of Traditionalists are retirees and are the largest lobbyist group, which is the AARP. If your parents or grandparents were of the Traditionalist Generation, you might have experienced a “waste not, want not” attitude with strong family values, conformity, and team players.
The Traditionalists are often referred to as the “Silent Generation.” This term came from the fact that during this era, the children were often expected to be seen and not heard.
As I pondered this generational topic, I found myself searching for an example of an “Active Working Traditionalist” that I could talk about because they might not have yet retired! To my surprise I found myself thinking about my Uncle Tom. This man has taken care of me and his family of five children with my Aunt Pat my whole life. He is a strong family man and then realized he is still working! Uncle Tom (he prefers to remain nameless) turned 83 year’s old this past April 16th. He is still the principle owner of his own CPA firm and worked those long and hard CPA hours during this 2018 tax season. As I mentioned early in this blog, all Traditionalists are not alike, and Uncle Tom never expected children to be “silent.” He valued their opinions, and my Aunt Pat was both a stay home mom and a partner in their CPA firm.
Uncle Tom values the old-time morals of family first, safety, conservatism, patience and financial security. I encourage you to look around for your Traditionalist at home, or maybe even in the workplace. Let’s appreciate our Traditionalists while we still have the opportunity to learn from them!
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.
Hi everyone! Back with another piece about the life between the lab and medical school. This time, I’d like to take a minute to talk about some new and exciting developments in laboratory diagnostics happening right now: immunoassays for critical troponins are undergoing an evolution. Fourth generation testing is slowly developing into its fifth-generation upgrade. Labs across the country are starting to discuss the relatively new FDA approved fifth-gen cardiac troponin T assay which has been shown to be a high-sensitivity test. But what does this mean for labs? Specifically, what does it mean between the bench and the bedside? The hospital I’m currently on service at is rolling out the first beta-test of this assay in New York City right now, and as it turns out—it’s going to change a lot. Not only will the new understanding of cardiac enzyme reference ranges need a complete overhaul but tailoring appropriate clinical responses to those values will need to be looked at as well. I’m not a sales rep and this isn’t going to be an adventure in comparative statistical analytics, but I think it’s a great time to have a conversation early on about what these new generation assays could mean for us in the lab.
A Whole New World
When I was in graduate school, doing my MLS training we were taught the same cardiac enzyme assay history that was developed over the last 50 or so years. Early acute markers of inflammation relating to acute myocardial infarctions (AMIs) with respect to acute phase reactants AST, LDH, CRP, etc. As more technology advanced, specific biomarker analyses of individual detection of things like CK or myoglobin became useful. The WHO criteria for AMI then established (and re-established since the 1970s) the laboratory requirements for CK-MB and detectable levels of troponin to correlate with clinical findings. Further sensitivity and specificity developments, and clinical research like the GUSTO and APACE trials, showed us just how sensitive newer (then troponin T and I) cardiac assays could be. Not to mention, instead of rule-in/rule-out criteria, we had the development of risk stratification. And as instrumentation developed so did our testing—CK and LDH replaced with CK-MB and its isoforms, AST went the way of Myoglobin, and LD ratios became reliable troponins!
Table 1. In each stage of acute coronary syndrome (ACS) various biomarkers are available and detectable in peripheral blood. The challenge has been to find the most reliable and time-sensitive cardiac enzyme(s) to reflect appropriate staging and risk stratification. Research is helpful, but clinical intervention required critical timing.
Ask most clinicians today about cardiac enzyme, cardiac injury studies, or other related markers and you’ll hear about CPK, CK-MB 1, 2, 3 and other isoenzymes, LDH electrophoresis, and of course troponins T and I. What’s more is that the reference ranges for most of these tests haven’t really changed much either. If I called you and said your patient in 706-W has a Troponin of <0.03 you might be relieved for now. If I said that same patient’s troponin was 0.560—we might have a different story unfold. But what if I told you your patient’s troponin was 13, and was trending down from 15? What do you do with that? What if I only called to report a troponin-DELTA which was 0.0? Was there an in-service you missed? Possibly. Sounds like your institution might have 5th-gen on board.
What was wrong with the old troponin?
In a word: nothing, really. This really isn’t about buy-in for a “better” test or a better detection method. This is about creating a dialogue about improving risk stratification for our patients with coronary disease. Let’s go back to Chicago, specifically the last hospital I worked in before starting medical school: Swedish Covenant Hospital. Having been through a few hospitals in my time, I can say you’d be hard pressed to find a more streamlined, albeit small community hospital, laboratory service. Running a full gamut of SIEMENS instrumentation and critical middleware-software, the management there ran a tight ship—which included critical troponins. We ran the TnI-Ultra assay on the ADVIA Centaur/XP platform. It was your standard three-part immunoassay sandwich test with a biotin-streptavidin antigen-antibody detection. It was fast, used little reagents, was relatively stable, had a great system of QC, and was calculably-flexible between heparinized and ETDA plasma samples. Two-point calibration kept it tight between (and this is from memory, loosely) 0.006 and 0.50 ng/mL, and I believe we called our critical values at 0.40 ng/mL. This was a good test, and it’s used in many labs today still. It’s got great stability and has room to interpret ACS risk stratification based on population data in each location. People understand those results, too. But exactly how much room between, let’s say 0.10 ng/mL and >0.50 ng/mL, is there to stratify that risk? Complex decision algorithms then become hybrids of institutional cardiology recommendations, American College of Cardiology (ACC) recommendations, emergency department input, and, of course, laboratory management recommendations.
Here at Bronx Care Hospital Center (BCHC), I spoke with a laboratory manager about rolling out this brand new high-sensivity troponin (hs-cTn), and we discussed their vaildation and policies. Along with this new project, the hospital has been a vocal part of American College of Cardiology ACC17 Acute and Stable Ischemic Heart Disease program addressing topics including marijuana use and ACS, stable angina risk stratification, NSTEMI sex differences in revascularization and outcomes, treating cocaine related ACS with beta blockers, and research Anticoagulation Therapy After Anterior Wall ST-Elevation Myocardial Infraction in Preventing LV Thrombi. So, it seems fitting that this is as good as any a pilot location for cardiology departments city-wide to watch and learn from the hs-cTn roll-out!
Tell me more about this new test…
This hs-cTn assay is an electrochemiluminescence immunoassay (ECLIA) that uses two monoclonal antibodies against human cardiac troponin T. At this institution, they are using this immune sandwich assay on a Roche Cobas E with a similar biotin-streptavidin coated microparticle complex as with the previous generation testing. This is a short test with similar reagent use and stability as before, and only for lithium heparinized samples. With a relatively quick turn-around in less than 10 minutes, the new hs-cTn offers critical information for clinical correlations on the fly from potential STEMI codes coming into the ED.
Without going into horrific details about validating data on old and new troponins across patient populations, there is something interesting to note here which came up in discussion with the lab manager: new reference ranges. Now, with testing sensitivity, cross-reactivity, ranges, and interfering substances, the ranges are no longer the decimal-place values reported that we’re all used to. The ranges we work with now at BCHC are cutoff between <12 ng/L for positives and >52 ng/L for critical values suggestive of acute coronary syndrome. The analytical measuring range is much larger now between 6-10,000 ng/L. With the adjustments for limits of detection and blanks on instrumentation, the specificities of these values are normalized on a larger index for reflecting differences in male and female cardiac enzyme activity to a common cutoff of that <12 ng/L value. But more so than just a value, a new part of trending troponins becomes much more important: the delta values. These are more acutely indicative of the cardiac necrosis and/or condition of other non-specific heart tissue damage en vivo occurring in patients. Taking all this into account, you now have a much wider and broader range of values to interpret and incorporate into your clinical decision making, which brought up a few questions when I spoke with lab staff as well as cardiologists.
So, what’s wrong with the new troponin?
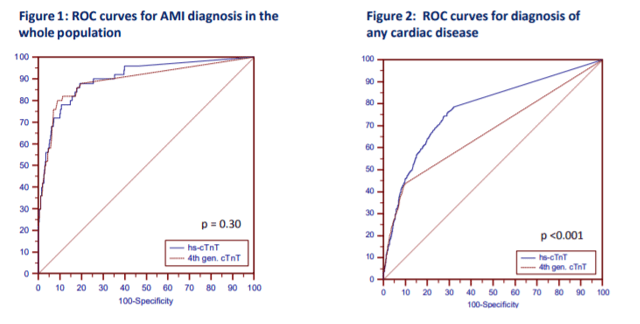
Okay, that’s a fair question at this point. And my answer is still: probably nothing. Sorry to be so inconclusive, but it’s still early days. There is a lot of data to support moving toward newer generation hs-cTn testing since it has been available outside of FDA-approval in Europe before January 2017. Research done in the Department of Internal Medicine and Central Institute for Medical Laboratory Diagnostics at Innsbruck Medical University in Austria show that new troponins might not be that different (read: better) than their 4th generation counterparts, at least with regard to emergency room visits. T. Ploner, et. al, argue that diagnosing AMI in the ED doesn’t really benefit from the heightened sensitivity offered by the new Roche 5th gen assay (Figure 1, Figure 1). But, when they compared the detection of other cardiac disease including AMI, unstable angina, heart failure, arrythmias, pulmonary emboli, pulmonary disease, anemia, renal disease, and several other entities, the 5th generation assay could more readily detect changes early and provide clinicians with critical data quickly (Figure 1, Figure 2).
Figure 1. Ploner et al. demonstrate here that there isn’t really any difference in the sensitivity of 4th generation vs. 5th generation troponins for detecting acute MI in the emergency room. However, there is a significant advantage in the detection of any cardiac disease, generally. (Source: Ploner et al. (2017) High-Sensitivity cardiac tropnonin assay is not superior to its previous 4th cTnT assay generation for the diagnosis of acute MI in a real-world emergency department, link: http://spo.escardio.org/eslides/view.aspx?eevtid=48&fp=P4177)
Finally, I think a review paper from the American Journal of Medicine last year summarized it best. Coming from the Department of Cardiovascular Diseases and Department of Laboratory Medicine and Pathology at Mayo Clinic in Rochester, MN, the authors discussed concern over the troubling over-sensitivity and potential pitfalls of reaching too far with hs-cTn testing. Their bottom line: collaborating on data and accuracy between cardiology, laboratory medicine, and emergency medicine, there is a great potential for this super sensitive test to provide clinicians with very useful data in the near future. We just have to process that data correctly. As always, results should be interpreted in conjunction with clinical presentation including medical history and laboratory data. But in the case of new and coming advances in critical care, there seem to be some common themes between my conversations here at BCHC and in what I read in the literature regarding how to ensure we move forward appropriately.
Multidisciplinary educational efforts are critical. The ER, the lab, and the cardiology department at each institution utilizing 5th gen troponins need to understand the new ranges, the new triaging cutoffs, the clinical correlations for consulting the ICU/CCU, and how to understand the deltas for their patient populations.
Create clear communications for your laboratory values. Will you normalize for gender or provide sex-specific confidence interval reporting? Will you provide tables for suggested value correlations with AMI/ACS protocols?
Order sets and in-service training. You’d be surprised how much the nitty gritty details of lab draws and ordering appropriate tests/tubes could slow down your institution’s advancement.
Figure 2. How the authors at Mayo Clinic establish the use of new hs-cTn assays in diagnosing and triaging potential AMI patients. (Source: Sandoval, Jaffe (2017) Using High-Sensitivity Cardiac Troponin T for Acute Cardiac Care, The American Journal of Medicine (2017) 130, 1358–1365, doi:10.1016/j.amjmed.2017.07.033)
At the very end of the day, it’s up to the institution. Clinical centers have to follow their own guidelines for cardiac pathology. ACC/ESC/AHA guidelines and Universal MI definitions are for clinical correlation across locations, but a single roll-out of a fancy new test can’t make a better ER. It really does take communication, collaboration, and accountability. We all have to push the envelope and practice at the top of our scopes in order to make health care better every day. One of the ways we might be able to do that now is by considering these new high-sensitivity troponins as a useful new clinical tool to improve patient outcomes.
Thanks for reading! See you next time!
Disclosure: I am no longer affiliated with Swedish Covenant Hospital in Chicago as an employee, and any recount of policy and/or procedure(s) specifically regarding their cardiology protocols and troponin resulting are a historical and anecdotal account of my time working there in the past. I have no affiliations with SIEMENS, Advia, Roche, or any other medical laboratory instrumentation institution. I am only affiliated with Bronx Care Hospital System as a current rotating medical student and my account of their transition to 5th gen testing is anecdotal from discussions with in-house staff, cardiologists, and laboratory management.
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
Most laboratories (and clinicians) utilize and rely on microscopic observation as the first step in the detection and identification of microorganisms. In some cases, direct microscopic analysis is used to determine the immediate clinical course of action. For example, if during a surgical procedure infection is suspected, then it is possible for the surgeon to submit a specimen to the laboratory for rapid (STAT) analysis. If polymorphonuclear leukocytes (PMN) and organisms are observed, then the differential diagnosis of infection is confirmed. Assuming proper specimen collection; if no PMN and no organisms are seen, then infection is less likely (true in most cases; there are always exceptions). These direct microscopic observation results thus drive the surgeon’s decision to either remove the infected area or perhaps advises on the use of intraoperative antimicrobials.
In part 1 of this series we discussed the pre-analytical problems associated with tissue culture; specifically, how specimen processing can affect whether or not organism is detected and recovered (1). In part 2 we will consider methods used for the direct observation of microorganisms in tissue specimens.
The Issue
Let’s take a step back to review our previous “culture-negative” endocarditis case (1). Recall that the blood cultures were negative at first, no organisms were observed on the Gram stain and the culture was also negative of the valve tissue. However, when we evaluated the frozen tissue that was “split” and saved for sequencing, the organism was observed via acridine orange (AO).
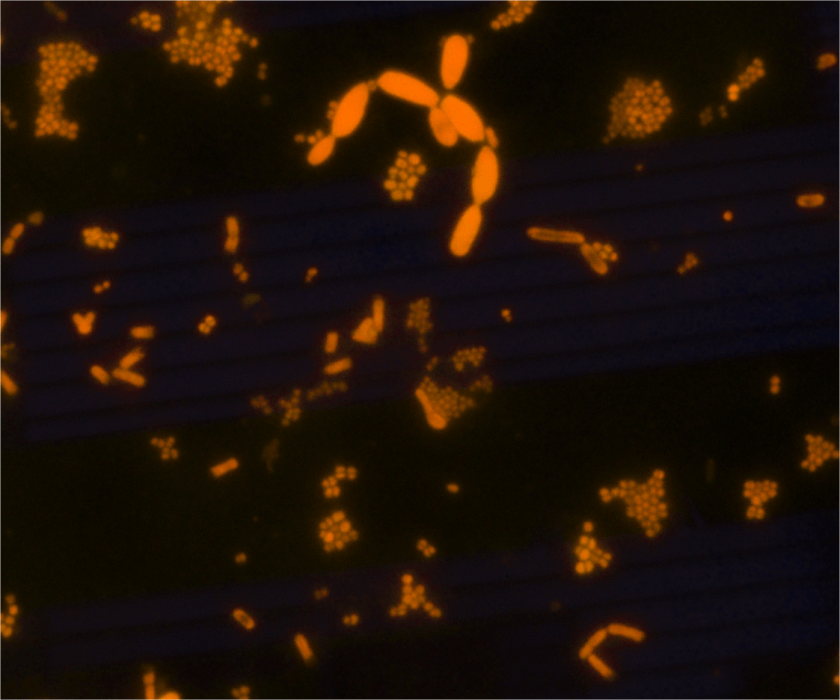
Image 1. AO of a positive broth culture from a homogenized tissue specimen. The AO stain displays cocci, bacilli, and yeast. The DNA-containing cells fluoresce orange.
The Solution
AO is a fluorescent dye that intercalates nucleic acids. It is a rapid, inexpensive, and most importantly- it is a sensitive alternate dye that can aid in microorganism detection in a variety of specimen types (2, 3 ,4, 5). AO is more specific than Gram stain (2, 3). Because bacterial DNA is not contained in a nucleus, but freely contained within the cell, the AO-stained cell takes the shape of the organism’s cellular morphology (Image 1). For example, if the organism is Staphylococcus aureus, then the AO would exhibit Gram positive cocci in clusters. Similarly, if the organism in question is Escherichia coli, then Gram negative bacilli would be observed, etc.
Some organisms (Campylobacter, Mycoplasma, etc.) do not stain well with Gram stain and as such they can be difficult to detect in direct specimen observations. The presence of many PMN and no organisms may be a clue that the organism is present in low numbers or that the organism does not stain well with the Gram stain. In cases such as these, the use of AO has proven to be very useful. Additionally, if the morphology of an organism in a Gram stain is difficult to interpret, then AO can also provide a more clear-cut answer. Lastly, the presence of artifact(s) can be problematic when reading Gram stains. “Is that Gram positive cocci or junk?”. Junk usually does not contain DNA and therefore does not fluoresce. Therefore, the information provided by the AO stain can aid in your decision to report cocci or not.
One disadvantage is that a fluorescent microscope is required to visualize the stain. Implementing AO may require the purchase of new equipment as not all laboratories have access to a fluorescent microscope. Because AO stains nucleic acid, anything with DNA or RNA will stain positive. This is another disadvantage because too much material that is positively stained can make interpreting the stain difficult at times. Another disadvantage is that a Gram stain is still required because the AO only allows the visualization of DNA-containing cells, it does not determine the Gram stain reaction.
Thinking back to our original case, the organism was present in the frozen tissue piece. It was not detected in the direct Gram stain, but rare organisms were noted in the AO. Because the AO was positive, we then reviewed the Gram stain and found rare Gram negative bacilli. This suggests that the organism was initially missed in the Gram stain because of the low abundance present. Bottom line, the AO was positive and we were thus able to provide the clinical team with relevant information.
The Conclusion
There are many stains used to aid in the observation of microorganisms. The AO stain is easy to perform, inexpensive, rapid, sensitive, and versatile. AO can be used on direct specimen smears, isolated colonies, and formalin-fixed paraffin embedded sections. Although there are limitations to using AO, the benefits considerably outweigh the shortcomings. AO is a great tool that laboratories should consider implementing as an alternate method for the direct observation of microorganisms.
Mirrett, S., Lauer, B.A., Miller, G.A., and Reller, B. 1982. Comparison of Acridine Orange, Methylene Blue, and Gram stains for Blood Cultures. J. Clin Microbiol. 15; 4: 562-566.
Lauer, B.A., Reller, B., and Mirrett, S. 1981. Comparison of Acridine Orange and Gram Stains for Detection of Microorganisms in Cerebrospinal Fluid and Other Clinical Specimens. J. Clin Microbiol. 14; 2:201-205.
Martinez, R.M., Bowen, T.R., and Foltzer, M.A. Prosthetic Devise Infections. Diagnostic Microbiology of the Immunocompromised Host. 2016 (Book chapter, chapter 27. Pages 711- 733. ASM Press.
Cooper, J.D., Dometita, D., Hasan, A., Dorion, P., Wolk, D.M. and Martinez, R.M. Orange you glad you checked the buffy coat? Clin. Microbiol. Newslett. 37: 9-13.
-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
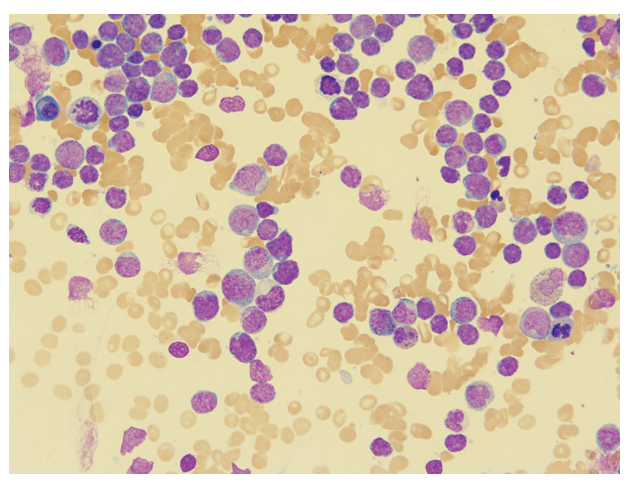
16 year old male with a history of chronic pilonidal cyst presented with fatigue, fevers and weight loss. He was febrile and noted to have cervical and inguinal adenopathy. Labs were significant for a white count of 77,000 with 85% peripheral blasts, anemia and thrombocytopenia.
The bone marrow aspirate shows cellular spicules with sheets of intermediate-to-large sized mononuclear cells with irregular nuclei, distinct nucleoli, dispersed chromatin, and scant to generous amphophilic cytoplasm, with occasional vacuoles, consistent with blasts.
The bone marrow core biopsy shows a greater than 95% cellular marrow, hypercellular for age with approximately 90% of the cellularity composed of an interstitial population of intermediate-to-large sized mononuclear cells with irregular nuclei, distinct nucleoli, dispersed chromatin, and scant to generous amphophilic cytoplasm, with occasional vacuoles, consistent with blasts.
Flow cytometry shows leukemic cells that express immaturity markers (TdT, CD34, CD117, HLA-DR), T cell lineage markers (CD2, CD7 cCD3), and multiple myeloid markers (CD13, CD117, and variable CD15 and CD11b as well as MPO in a small subset).
Bone marrow core biopsy staining (not shown) had similar findings with blasts showing dim-to-strong positivity for myeloperoxidase, lysozyme, CD34 and CD117, as well as strong positivity for TdT. CD7 was weakly positivity, as well as CD3. CD4 and CD5 were negative.
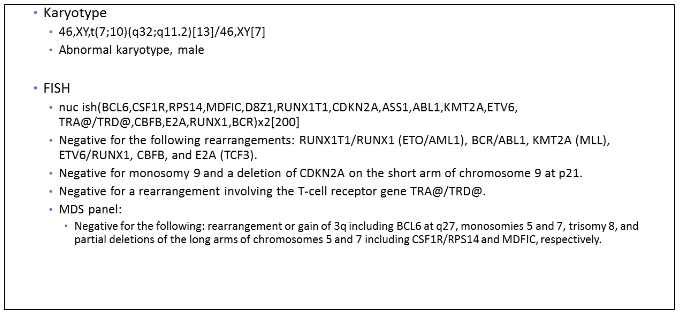
Genetics diagnosticsNGS panel
With the expression of MPO by flow cytometric analysis and immunohistochemistry, a final diagnosis of acute leukemia with myeloid and T lymphoid phenotypic features, most consistent with T/Myeloid Mixed Phenotype Acute Leukemia (MPAL) was rendered.
Discussion
Most acute leukemias are definitively assigned to either myeloid, T or B lymphoid lineages. However, approximately 2-5% of patients diagnosed with acute leukemia display an ambiguous lineage after immunophenotyping. A portion of these cases are classified under the category of mixed phenotype acute leukemia (MPAL) by the current WHO nomenclature.1
In a study of 117 MPAL patients by Yan et al, 55% of the cases had combined B/Myeloid, while 33% had T/Myeloid, and 12% had B/T/Myeloid. CD34 was strongly positive in 82% of cases, which reinforces the idea that the cell of origin is a multi-potent stem cell capable of differentiating into both myeloid and lymphoid progenitors. Cytogenetic analysis revealed no chromosomal abnormality in 36% of the patients with MPAL, while 64% had complex karyotypes (>3 aberrations). Translocation (9;22) was the most common abnormality, found in 15% of patients. Monosomy 7, a common finding in myelodysplastic syndromes as well, was found in 7.6% of patients. Mutational analysis revealed IKZF1 deletions in 13% of patients, ASXL1 in 6.5% of patients and a variety of other mutations including ETV6, NOTCH1 and TET2.2
In 2016, Eckstein and colleagues demonstrated epigenetic regulatory genes such as DNMT3A, IDH2, TET3 and EZH2 are the most commonly mutated in MPAL. RAS mutations including NRAS and KRAS and tumor suppressors, such as TP53 and WT1, were frequently identified as well.3
Interestingly enough, the genetic features of MPAL often overlap with early T-cell precursor acute lymphoblastic leukemia (ETP-ALL). ETP-ALL is a high-risk subgroup, representing 10% of adult T-lineage acute lymphoblastic leukemia. It is defined by a characteristic immunophenotype (CD1a/CD8 negative with weak CD5) and distinct gene expression associated with early arrest in T-cell development. This subgroup, called the LYL1 group, expresses the early hematopoietic marker CD34 as well as myeloid antigens (CD13 or CD33), but lacks expression of both CD4 and CD8. These leukemias are associated with a poor prognosis, with a 10- year overall survival of 19% compared to 84% for all other T-ALLs.4
Zhang et al in 2012 performed whole genome sequencing on ETP-ALL cases and found a high frequency of mutations in factors mediating cytokine receptor, tyrosine kinase and RAS signaling. It also showed inactivating mutations in genes encoding transcription factors (GATA3, ETV6, RUNX1, IKZF1) as well as genes involved in histone modification, such as EZH2.5
Overall, the genetic features of both ETP-ALL and MPAL display an identical genomic pattern that involves multiple pathways, including tyrosine kinase signaling, cytokine receptor response, RAS pathway activation, and loss of function in tumor suppressors. These findings give credence to the hypothesis that the early T-cell precursor actually displays more of a pluripotent stem cell profile that is similar to myeloid neoplasms, thus confounding findings found during molecular profiling. With this paradigm in mind, molecular diagnostics cannot differentiate between ETP-ALL and in this case, MPAL.
References
Swerdlow, Steven H. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Revised 4th ed., International Agency for Research on Cancer, 2017.
Yan et al. Clinical, immunophenotypic, cytogenetic, and molecular genetic features in 117 patients with mixed-phenotype acute leukemia defined by WHO-2008 classification. 2012 November;97(11):1708-12.
Eckstein OS et al. Mixed Phenotype Acute Leukemia (MPAL) Exhibits Frequent Mutations in DNMT3A and Activated Signaling Genes. Exp Hematol. 2016 August; 44(8):740-744.
Ferrando AA et al. Gene expression signatures define novel oncogenic pathways in T cell acute lymphoblastic leukemia. Cancer Cell. 2002. 1:75–87.
Zhang J et al. The genetic basis of early T-cell precursor acute lymphoblastic leukemia. Nature. 2012 Jan 11;481(7380):157-63.
–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
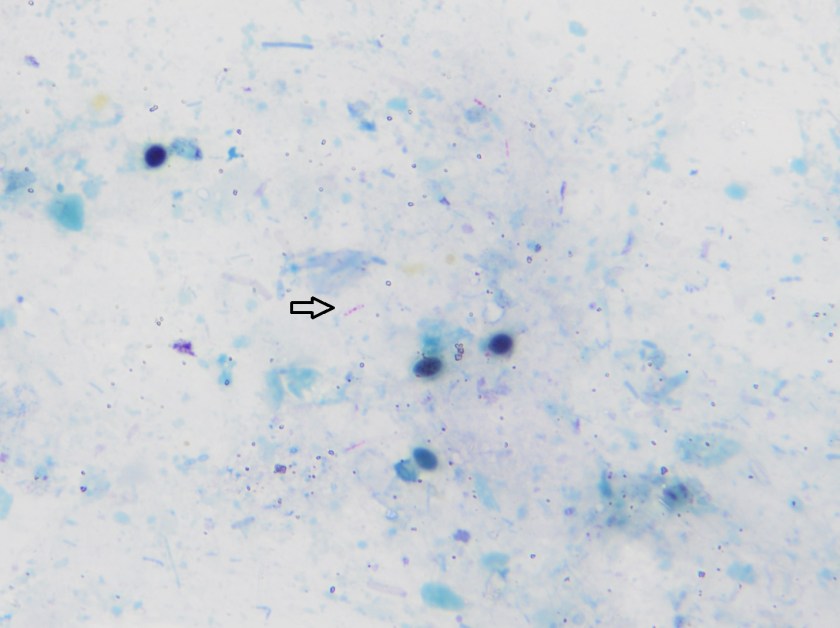
A 27 year old African American male presented to the emergency department with confusion and abdominal pain. His past medical history was significant for a 100 pound unintended weight loss and oral candidiasis which prompted a recent diagnosis of HIV. He was prescribed anti-retroviral therapy and antibiotic prophylaxis with which he reported compliance. Currently, he had no fever or chills. An abdominal CT scan showed an enlarged liver & spleen, generalized lymphadenopathy and a small amount of fluid. Significant lab work included anemia with a platelet count of 18,000 TH/cm2, absolute CD4 100 cells/cm2 (reference range: 506-3142 cells/ cm2) and a HIV viral load of 4,871 vc/mL. Given the concern for an infectious process, the infectious disease service was consulted and the patient underwent a thorough infectious work up including lumbar puncture, was started on board spectrum antibiotics and antifungals and was placed in airborne isolation until Mycobacterium tuberculosis could be ruled out.
Laboratory Identification
Image 1. Direct smear from a stool specimen showed beaded acid fast bacilli (Kinyoun stain, 1000x oil immersion).Image 2. Direct smear from a stool specimen showed beaded acid fast bacilli (Kinyoun stain, 1000x oil immersion).
Initial diagnostic testing for bacterial, fungal and viral pathogens was negative. Three concentrated sputum AFB smears as well as a TB PCR were negative. The quantiferon gold TB test was also negative. The physician additionally ordered AFB blood and stool cultures. The direct smear from the stool specimen showed rare, beaded acid fast bacilli in a background of bacteria and yeast normally present in the stool via Kinyoun stain (Images 1 & 2). The specimen was sent to the department of health for additional work up. There was growth after 21 days incubation and Mycobacterium avium complex was identified by high performance liquid chromatography (HPLC).
Discussion
Mycobacterium avium complex (MAC) is a slow growing nontuberculous mycobacteria (NTM) frequently involved in human disease. Historically, it was classified as Runyon group III which are non-chromogens and do not produce pigment regardless of culture conditions. The group encompasses two taxa, M. avium and M. intracellulare. The species M. avium can further be classified into four subspecies: subsp. avium, subsp. silvaticum, subsp. paratuberculosis and subsp. hominissuis. Of interest, M. avium subsp. paratuberculosis can often be seen in association with Crohn’s disease.
In general, MAC organisms have low pathogenicity, but in the setting of those with lung disease (including cystic fibrosis), heavy smokers, immunocompromised patients and those with HIV, it is a well-known cause of disease. Infections with MAC can range from localized mycobacterial lymphadenitis and isolated pulmonary disease to bacteremia with dissemination to almost any organ. The organisms are located in circulating monocytes and further spread most commonly to the lungs, gastrointestinal tract and lymph nodes. In the case of HIV positive patients, MAC is the most common environmental NTM causing disease, especially in those with CD4 counts less than 100 cells/mm3 who are more likely to have disseminated disease.
In order to diagnosis MAC infections, specimens from blood, sputum, lymph nodes and other tissues are preferred. In addition, stool may also be an acceptable alternative in HIV patients if other specimens are negative or unable to be obtained. However, the sensitivity of a direct stool smear is only 32 to 34% making it not a very effective approach to identifying those at risk for disseminated infections. Once the culture has growth, various methods can be used to identify MAC, including phenotypic methods, DNA probe testing, HPLC, pyrosequencing and other forms of PCR & sequencing.
In the case of our patient, he was started on M. tuberculosis therapy: rifabutin, isoniazid, pyrazinamide & ethambutol (RIPE) until TB was ruled out. At that time, he was removed from isolation and switched to a drug regimen that included azithromycin, rifabutin and ethambutol. He showed clinical improvement and his cell counts, renal function and liver enzymes trended to normal ranges.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
Last month we celebrated Lab Week, to recognize and show appreciation for Medical Laboratory Scientists and Technicians. Lab week is also a time to reminisce, and tell stories of the lab “in the old days.” I have worked with many technologists who have now been in the field for more than 50 years, and some who have worked in the same hospital all that time! Lab techs love to share stories about their experiences over the years, the days without computers, old methodologies, ancient lab equipment and manual testing. Listening to these stories always makes me think about just how far we have come in the field in the last 50- 60 years, and gives me a true appreciation for modern technology. It causes me to reflect on all the changes and developments that enable us to give physicians a wealth of knowledge that was previously unavailable.
During the first half of the 20th century, the complete blood count (CBC) was performed using exclusively manual techniques. Blood cell counts (erythrocytes, leukocytes, thrombocytes) were performed under the microscope using diluted blood samples and a hemocytometer. For each specimen, a technologist spent about 30 minutes at a microscope manually counting the cells and calculating the total count using a mathematical formula. A spectrophotometer was used to perform the hemoglobin by the cyanmethemoglobin method, and a spun hematocrit was performed. Indicies were calculated. A manual smear was made, stained, and cells were counted and differentiated under the microscope. To complete a CBC, all these procedures had to be performed individually, with duplicate testing and applying mathematical calculations, and could take over 2 hours. After all these tests were performed, results were reported on paper and sent to the patient’s doctor or the nursing floor.
In 1953 Wallace Coulter patented the Coulter Principle for counting and sizing microscopic particles. The Coulter Principle can be used for measuring any particles that can be suspended in an electrolyte solution, and has been used in the food and drug industry, in beer making, in the manufacture of construction materials and thousands of other applications. However, probably the most important application has been in the medical field where it has revolutionized the science of hematology. Coulter suspended red blood cells in a solution and, with an electrical current flowing, passed the solution through an aperture. As the cells pass through the current, the impedance between the terminals changes, and this change can be measured as a pulse. The first Coulter Counter measured the number of cells by counting the number of these pulses. The first Model A Coulter Counter was sold in 1956, manufactured in Coulter’s basement in Chicago. The Model A counted red blood cells in a sample in 10 minutes, a marked improvement over manual counting! The Coulter Counter was hailed for its speed, accuracy, and opportunities for reducing human error, tedium and eye strain.
During the 1960’s, an improved Model B Coulter Counter was developed and Model A and Model B were used to count both leukocytes and erythrocytes. Other Coulter Counter models soon followed, and competitors entered the market with their versions of cell counters. Within a decade, nearly every hospital in the United States had a Coulter Counter, and the new, advanced Coulter Model F was widely used. In 1968 the first fully automated hematology analyzer, The Coulter Counter Model S was introduced, and could perform a seven-parameter CBC. The Model S could perform not only WBC and RBC counts, but also reported Hemoglobin, Hematocrit, Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH) and Mean Corpuscular Hemoglobin Concentration (MCHC). In 1955 it took one or several technologists 2 hours to perform a CBC, and in 1969 an automated hematology analyzer could analyze a sample in under 2 minutes.
Image 2. “Woman Using a Model F Coulter Counter Cell Counter,” 1969. Beckman Historical Collection, Box 58, Folder 94. Science History Institute. Philadelphia. https://digital.sciencehistory.org/works/736664585.
Image 2. “Woman Using a Model F Coulter Counter Cell Counter,” 1969. Beckman Historical Collection, Box 58, Folder 94. Science History Institute. Philadelphia. https://digital.sciencehistory.org/works/736664585.
As these improvements and advancements continued, and Coulter patents expired, new manufacturers entered the field. Technicon Instruments Corporation, Ortho Diagnostics, Instrumentation Laboratories and Toa Medical Electronics, (presently Sysmex Corporation) were among the first Coulter competitors. From a simple automated blood cell count, to the first seven-parameter CBC, we saw hematology changing before our eyes. More reliable automated platelet counts were added in the 1970s. In the 1980s we saw the first hematology analyzers that could perform automated differentials and the first automated reticulocyte analyzers. In the late 1990’s, we saw the advent of digital cell images and automated manual differentials.
Today, modern automated cell counters sample blood, and quantify, classify, and describe cell populations. These instruments use optical light scatter, impedance methods based on the Coulter principle or a combination of both optical and impedance methods. Progressive improvement in these instruments has allowed the enumeration and evaluation of blood cells with great accuracy, precision, and speed, at a very low cost per test. The latest descendant of the Model A Coulter Counter, the LH 750, can determine 26 reportable hematological parameters. The Sysmex XN-9100 with four XN analyzers reports 30 parameters and has a throughput of up to 400 CBCs and 75 smears per hour. Today’s analyzers can accomplish more and more routine diagnostics, and the role of the hematology technologist continues to evolve and expand.
This is not your grandmother’s hematology! We’ve truly come a very long way in 60 years. Modern hematology instruments not only perform a CBC, but they give us next generation diagnostics as well. Many give us advanced clinical parameters and other new parameters which provide physicians with additional information about the state of blood cells. We can report out immature granulocytes with every differential, automated nucleated red blood cell counts, immature platelet fractions and fluorescent platelet counts, and report the amount of hemoglobin in reticulocytes and the immature reticulocyte fraction. Future directions of hematology instrumentation include the addition of even more new parameters. In upcoming Hematology blogs I will be presenting case studies that highlight each of these advanced clinical parameters and discuss how physicians can use this new information in making diagnoses.
SLAS TECHNOLOGY: Translating Life Sciences Innovation. The Coulter Principle: Foundation of an Industry. Marshall Don, Ph.D., Beckman Coulter, Inc.. Volume: 8 issue: 6, page(s): 72-81. Issue published: December 1, 2003 https://doi.org/10.1016/s1535-5535(03)00023-6
Medical Electronic Laboratory Equipment 1967-1968. G.W.A Dummer and J. MacKenzie Robertson. 1967 Pergamon Press
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
Ethical decisions are a part of everyday life, but they are even more prominent when leading a team, a company or an entire organization. Ethics are essential for effective leadership, and leaders are responsible for creating ethical organizations. Because people make decisions multiple times a day, ensuring that every decision is ethical is an essential skill, especially for leaders. Ethical decisions are often based on intuition without a logical explanation for why a certain solution was chosen. However, to increase the ethics of a situation, logic needs to be applied to the decision-making process. Logical analysis of a situation creates a deeper understanding of the underlying issues and so improves outcomes. As ethical leaders it is our duty to lead employees and the company towards the best possible outcomes.
There are many logical approaches to ethics and multiple approaches can be used simultaneously to arrive at the best ethical answer. Some analytical approaches to ethics include:
The Utilitarian Approach
This approach relies on the concept that the best ethical decision has the most beneficial consequences for the largest group of people. The four steps of a utilitarian analysis include defining the ethical challenge, identifying those affected by the decision, determine the positive and negative consequences of the decision, and weigh the differences between those consequences.
Kant’s Categorical Imperative
Kant approaches ethical dilemmas based on the belief that people should always be the main focus and never be treated as a means. Kant recommends basing your ethical decision on one simple question: “Would I want everyone else to make the decision I did?” If the answer is no, then it is not the right decision. If the answer is yes, Kant argues that the analysis and decision are correct.
Rawls’ Justice as Fairness
This concept is centered on two principles based in theories of fairness and justice. First, everyone has an equal right to basic liberties, and second, inequalities, both social and economic, have two conditions: 1) everyone has an equal opportunity to qualify for job, and 2) priority should be given to meeting the needs of the less fortunate.
Pragmastism
This approach uses pragmatism as an ethical decision making tool. The process of using the scientific method allows people to come up with ethical solutions, because the hypotheses are tested through dramatic rehearsal. One should come up with a solution to an ethical dilemma and then test it, hypothetically, to see if the solution and its consequences were indeed ethical. What sets this approach apart is the use of emotion and feeling as indicators of unethical decisions.
Altruism
This method to ethical dilemmas focuses on what is best for others and not what is best for oneself. People helping one another and witnessing leaders make sacrifices to the benefit of their employees or customers has a trickle-down effect on the rest of the staff.
Ethical decisions have a profound impact on others, even when they are not directly involved or affected by the decision. Good character is created when making ethical decisions and that character disintegrates when unethical decisions are made. Everyone has an influence on other people, therefore it is our obligation to others and the world to not only keep our ethical character intact, but to increase it so that it can withstand the tests of our time while encouraging others to do the same.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
A 51-year-old man was hospitalized for swelling of his left middle finger. He was in a normal state of health until 6 months prior, when he sustained an injury to his left third finger from a catfish while fishing in Florida in brackish water. The patient claimed he had caught a catfish and was stabbed by one of the spines of the fish in the middle portion of his finger. It became infected and he was prescribed a couple different courses of antibiotics, the details of which are not entirely clear. About one week leading up to his hospitalization, the finger became more swollen, and he had prominent lymphangitic streaking up the left arm as high as the upper bicep, with pain. He did not have any fevers, chills, or night sweats. Initial blood cultures taken were negative. He was admitted for three days on vancomycin/cipro, with resolution of the lymphangitic streaking but ongoing prominence of the swollen left third finger. MRI showed prominent tenosynovitis of the left 3rd finger tendon sheath, though the second, fourth, and fifth digits were also involved. Surgical debridement was recommended at the time but he preferred to pursue medical management. He was started on cipro/doxy/clarithro empirically at the time.
The infection was refractory to medical management. About 3 weeks later, his left third finger “burst open” with a draining sinus tract and purulent discharge (Image 1). He still denied any systemic symptoms such as fever, chills, night sweats. He was seen by infectious disease and orthopedic surgery and subsequently consented to radical tenosynovectomy for suspected mycobacterial chronic tenosynovitis.
Image 1. Infected third finger.
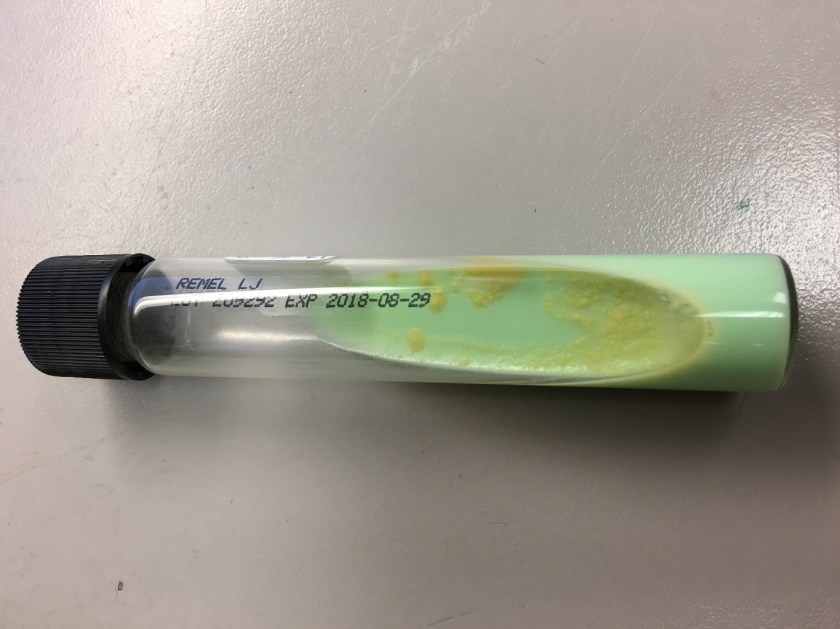
Tissue biopsy was sent for surgical pathology and culture. Histopathologically, the lesion showed chronic lymphohistiocytic and granulomatous inflammation; no microorganisms were identified on special stains. However, AFB culture was positive in the LJ slant and speciation was confirmed (Image 2).
Figure 2. Bright yellow colonies after light exposure on LJ slant media.
Discussion
Mycobacterium marinum was identified at a reference laboratory. Although infection with M. marinum is uncommon, the epidemiology of M. marinum disease is distinctive from other non-tuberculous mycobacterial species. The natural habitat of M. marinum is aquatic, and can be found in both fresh and salt water, including marine organisms, swimming pools, and fish tanks. The annual incidence is estimated at 0.27 cases per 100,000 adult patients.1 The infection is typically limited to the skin, mostly involving limbs, with rare spread to deeper structures reported.
M. marinum causes cutaneous disease as a consequence of exposure to water, usually in the context of a minor abrasion, laceration, puncture wound, or bite wound. Skin infections can occur from putting one’s hand into a contaminated fish tank, resulting in the condition called fish tank granuloma.
Histopathology often demonstrates suppurative granulomatous inflammation. In the microbiology laboratory, M. marinum is a photochromogen, meaning it produces pigment when cultured and exposed to light. Culture growth is optimal at 32°C over 7-14 days. Therefore, cooler extremities, particularly hands, are affected more often than central areas. Providers should be aware that M. marinum may cause a positive tuberculin skin test.2
M. marinum is a slow growing organism that is readily detected by acid fast smear and culture techniques. Confirmation of the presence or absence of mycobacteria in clinical specimens has traditionally required culture. However, traditional methods of identifying mycobacterial isolates to the species level are slow, based upon growth characteristics on solid media and subsequent biochemical tests, requiring additional weeks for subcultures. Newer techniques include MALDI-TOF MS, 16S ribosomal DNA sequencing, PCR-restriction length polymorphism analysis (PRA), and high-performance liquid chromatography (HPLC).
M. marinum infection responds slowly to appropriate antibiotic therapy. Infected patients may require treatment for 2 weeks or up to 18 months. M. marinum infection sequelae include persistent ulceration, draining sinuses, or septic arthritis.
Lewis et al. Fish tank exposure and cutaneous infections due to Mycobacterium marinum: tuberculin skin testing, treatment, and prevention. CID. 2003;37(3):390-7.
-Thomas Rogers, DO is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
Our patient is a 47-year-old female with a history of type II diabetes mellitus, hypertension, pancreatic insufficiency, systemic sarcoidosis with lung and liver involvement. She was admitted into the ED for severe hypercalcemia, hypokalemia and hypomagnesemia. Her total calcium concentration was at 15.1 mg/dL (ref range: 8.3-10.2 mg/dL, critical: >13.0) at admission and albumin was low. Further testing revealed 25-hydroxy vitamin D (25(OH)D) of 23.2 ng/mL, which is considered insufficient, and decreased PTH of < 15 pg/mL (ref range: 15 – 65). From these results, primary hyperparathyroidism was ruled out. PTH related peptide (PTHrp) was tested given her sarcoidosis history.
PTHrp is produced by some cancers, especially kidney, breast and lung cancers, and as well as lymphoma and leukemia. It has the same N-terminal and binds to the same receptor as PTH, therefore sharing some functions of PTH. In patients with hypercalcemia associated with malignancy, PTHrP may be evaluated. There are also case reported sarcoidosis-related hypercalcemia due to production of PTHrp. In the case, PTHrp was normal at 0.4 pmol/L (ref range: < 2.0).
Further tests showed that 1, 25-dihydroxyvitamin D (DHVD) was elevated at a concentration of 93.3 pg/mL (ref: 18.0 – 78.0). In the presence of decreased 25(OH)D, this result suggested that the 1-alpha-hydroxylase could be the cause of hypercalcemia. DHVD is the active form of vitamin D. It promotes intestinal calcium absorption and, in concert with PTH, skeletal calcium deposition. 25(OH)D converts to DHVD via 1-alpha-hydroxylase, which is almost exclusively expressed in the kidney, but can also be found in some extrarenal tissues, including inflammatory cells of the monocyte/macrophage lineage commonly seen in sarcoidosis and other granulomatous diseases. DHVD produced in extrarenal tissues is PTH-independent, and moreover, elevated calcium induced by extrarenal DHVD can inhibit PTH production via calcium-sensing receptor (CaSR) on parathyroid cells.
Sarcoidosis is a multisystem inflammatory disease of unknown etiology manifests as granulomas found predominantly in the lungs and lymph nodes. Hypercalcemia is seen in about 10-13% of patients. Overproduction of 1-alpha-hydroxylase and production of PTHrp can both contribute to the hypercalcemia in some patients with sarcoidosis. In this case, PTHrp was normal and elevated 1-alpha-hydroxylase was found to be the cause of hypercalcemia.
In addition to treatment of the underlying disorder, treatment of hypercalcemia in sarcoidosis is aimed at reducing intestinal calcium absorption and DHVD synthesis. Besides dietary interventions, glucocorticoids and bisphosphonates have also been used successfully to treat hypercalcemia in sarcoidosis:
Glucocorticoids: inhibit DHVD synthesis by the activated mononuclear cells (major contribution), inhibit intestinal calcium absorption and osteoclast activity
Bisphosphonates: inhibit the resorption of bone by osteoclasts
-Rongrong Huang, PhD is a first year clinical chemistry fellow at Houston Methodist Hospital. Her interests include general clinical chemistry, genetic biochemistry and applications of mass spectrometry in clinical laboratories.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.