Most laboratories (and clinicians) utilize and rely on microscopic observation as the first step in the detection and identification of microorganisms. In some cases, direct microscopic analysis is used to determine the immediate clinical course of action. For example, if during a surgical procedure infection is suspected, then it is possible for the surgeon to submit a specimen to the laboratory for rapid (STAT) analysis. If polymorphonuclear leukocytes (PMN) and organisms are observed, then the differential diagnosis of infection is confirmed. Assuming proper specimen collection; if no PMN and no organisms are seen, then infection is less likely (true in most cases; there are always exceptions). These direct microscopic observation results thus drive the surgeon’s decision to either remove the infected area or perhaps advises on the use of intraoperative antimicrobials.
In part 1 of this series we discussed the pre-analytical problems associated with tissue culture; specifically, how specimen processing can affect whether or not organism is detected and recovered (1). In part 2 we will consider methods used for the direct observation of microorganisms in tissue specimens.
The Issue
Let’s take a step back to review our previous “culture-negative” endocarditis case (1). Recall that the blood cultures were negative at first, no organisms were observed on the Gram stain and the culture was also negative of the valve tissue. However, when we evaluated the frozen tissue that was “split” and saved for sequencing, the organism was observed via acridine orange (AO).
The Solution
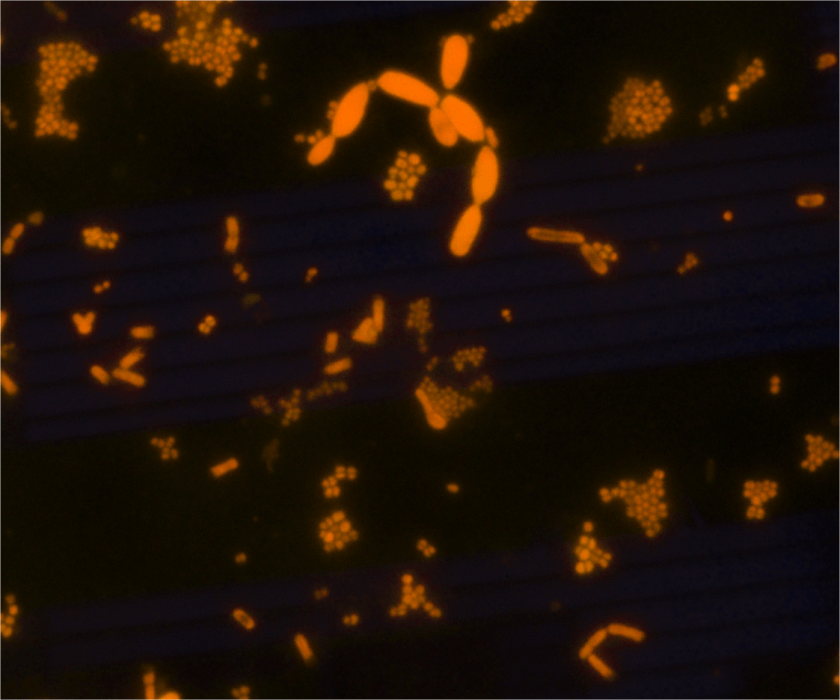
AO is a fluorescent dye that intercalates nucleic acids. It is a rapid, inexpensive, and most importantly- it is a sensitive alternate dye that can aid in microorganism detection in a variety of specimen types (2, 3 ,4, 5). AO is more specific than Gram stain (2, 3). Because bacterial DNA is not contained in a nucleus, but freely contained within the cell, the AO-stained cell takes the shape of the organism’s cellular morphology (Image 1). For example, if the organism is Staphylococcus aureus, then the AO would exhibit Gram positive cocci in clusters. Similarly, if the organism in question is Escherichia coli, then Gram negative bacilli would be observed, etc.
Some organisms (Campylobacter, Mycoplasma, etc.) do not stain well with Gram stain and as such they can be difficult to detect in direct specimen observations. The presence of many PMN and no organisms may be a clue that the organism is present in low numbers or that the organism does not stain well with the Gram stain. In cases such as these, the use of AO has proven to be very useful. Additionally, if the morphology of an organism in a Gram stain is difficult to interpret, then AO can also provide a more clear-cut answer. Lastly, the presence of artifact(s) can be problematic when reading Gram stains. “Is that Gram positive cocci or junk?”. Junk usually does not contain DNA and therefore does not fluoresce. Therefore, the information provided by the AO stain can aid in your decision to report cocci or not.
One disadvantage is that a fluorescent microscope is required to visualize the stain. Implementing AO may require the purchase of new equipment as not all laboratories have access to a fluorescent microscope. Because AO stains nucleic acid, anything with DNA or RNA will stain positive. This is another disadvantage because too much material that is positively stained can make interpreting the stain difficult at times. Another disadvantage is that a Gram stain is still required because the AO only allows the visualization of DNA-containing cells, it does not determine the Gram stain reaction.
Thinking back to our original case, the organism was present in the frozen tissue piece. It was not detected in the direct Gram stain, but rare organisms were noted in the AO. Because the AO was positive, we then reviewed the Gram stain and found rare Gram negative bacilli. This suggests that the organism was initially missed in the Gram stain because of the low abundance present. Bottom line, the AO was positive and we were thus able to provide the clinical team with relevant information.
The Conclusion
There are many stains used to aid in the observation of microorganisms. The AO stain is easy to perform, inexpensive, rapid, sensitive, and versatile. AO can be used on direct specimen smears, isolated colonies, and formalin-fixed paraffin embedded sections. Although there are limitations to using AO, the benefits considerably outweigh the shortcomings. AO is a great tool that laboratories should consider implementing as an alternate method for the direct observation of microorganisms.
References
- https://labmedicineblog.com/2018/04/20/tissue-is-the-issue-splitting-specimens-part-1/
- Mirrett, S., Lauer, B.A., Miller, G.A., and Reller, B. 1982. Comparison of Acridine Orange, Methylene Blue, and Gram stains for Blood Cultures. J. Clin Microbiol. 15; 4: 562-566.
- Lauer, B.A., Reller, B., and Mirrett, S. 1981. Comparison of Acridine Orange and Gram Stains for Detection of Microorganisms in Cerebrospinal Fluid and Other Clinical Specimens. J. Clin Microbiol. 14; 2:201-205.
- Martinez, R.M., Bowen, T.R., and Foltzer, M.A. Prosthetic Devise Infections. Diagnostic Microbiology of the Immunocompromised Host. 2016 (Book chapter, chapter 27. Pages 711- 733. ASM Press.
- Cooper, J.D., Dometita, D., Hasan, A., Dorion, P., Wolk, D.M. and Martinez, R.M. Orange you glad you checked the buffy coat? Clin. Microbiol. Newslett. 37: 9-13.

-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
