Case History
A 51-year-old man was hospitalized for swelling of his left middle finger. He was in a normal state of health until 6 months prior, when he sustained an injury to his left third finger from a catfish while fishing in Florida in brackish water. The patient claimed he had caught a catfish and was stabbed by one of the spines of the fish in the middle portion of his finger. It became infected and he was prescribed a couple different courses of antibiotics, the details of which are not entirely clear. About one week leading up to his hospitalization, the finger became more swollen, and he had prominent lymphangitic streaking up the left arm as high as the upper bicep, with pain. He did not have any fevers, chills, or night sweats. Initial blood cultures taken were negative. He was admitted for three days on vancomycin/cipro, with resolution of the lymphangitic streaking but ongoing prominence of the swollen left third finger. MRI showed prominent tenosynovitis of the left 3rd finger tendon sheath, though the second, fourth, and fifth digits were also involved. Surgical debridement was recommended at the time but he preferred to pursue medical management. He was started on cipro/doxy/clarithro empirically at the time.
The infection was refractory to medical management. About 3 weeks later, his left third finger “burst open” with a draining sinus tract and purulent discharge (Image 1). He still denied any systemic symptoms such as fever, chills, night sweats. He was seen by infectious disease and orthopedic surgery and subsequently consented to radical tenosynovectomy for suspected mycobacterial chronic tenosynovitis.

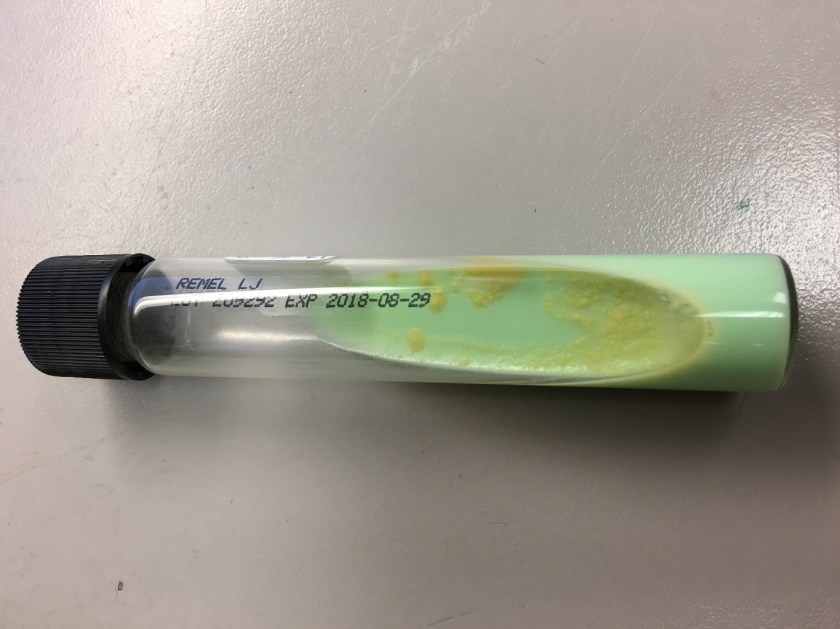
Tissue biopsy was sent for surgical pathology and culture. Histopathologically, the lesion showed chronic lymphohistiocytic and granulomatous inflammation; no microorganisms were identified on special stains. However, AFB culture was positive in the LJ slant and speciation was confirmed (Image 2).
Discussion
Mycobacterium marinum was identified at a reference laboratory. Although infection with M. marinum is uncommon, the epidemiology of M. marinum disease is distinctive from other non-tuberculous mycobacterial species. The natural habitat of M. marinum is aquatic, and can be found in both fresh and salt water, including marine organisms, swimming pools, and fish tanks. The annual incidence is estimated at 0.27 cases per 100,000 adult patients.1 The infection is typically limited to the skin, mostly involving limbs, with rare spread to deeper structures reported.
M. marinum causes cutaneous disease as a consequence of exposure to water, usually in the context of a minor abrasion, laceration, puncture wound, or bite wound. Skin infections can occur from putting one’s hand into a contaminated fish tank, resulting in the condition called fish tank granuloma.
Histopathology often demonstrates suppurative granulomatous inflammation. In the microbiology laboratory, M. marinum is a photochromogen, meaning it produces pigment when cultured and exposed to light. Culture growth is optimal at 32°C over 7-14 days. Therefore, cooler extremities, particularly hands, are affected more often than central areas. Providers should be aware that M. marinum may cause a positive tuberculin skin test.2
M. marinum is a slow growing organism that is readily detected by acid fast smear and culture techniques. Confirmation of the presence or absence of mycobacteria in clinical specimens has traditionally required culture. However, traditional methods of identifying mycobacterial isolates to the species level are slow, based upon growth characteristics on solid media and subsequent biochemical tests, requiring additional weeks for subcultures. Newer techniques include MALDI-TOF MS, 16S ribosomal DNA sequencing, PCR-restriction length polymorphism analysis (PRA), and high-performance liquid chromatography (HPLC).
M. marinum infection responds slowly to appropriate antibiotic therapy. Infected patients may require treatment for 2 weeks or up to 18 months. M. marinum infection sequelae include persistent ulceration, draining sinuses, or septic arthritis.
References
-
-
- Akram SM, Bhimji SS. Mycobacterium Marinum. 2017. StatPearls.
- Lewis et al. Fish tank exposure and cutaneous infections due to Mycobacterium marinum: tuberculin skin testing, treatment, and prevention. CID. 2003;37(3):390-7.
-
-Thomas Rogers, DO is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
