A 41 year old African male presented to the ED with complaints of abdominal pain, weight loss, and decreased appetite over one month. He immigrated from Zimbabwe 10 years prior, and most recently visited 4 months ago. His past medical history is non-contributory. He was found to have microcytic anemia (Hgb 9.3 g/dL, MCV 77.0 fL), pneumonia, and focal small bowel dilation with thickening and inflammatory changes on abdominal CT.
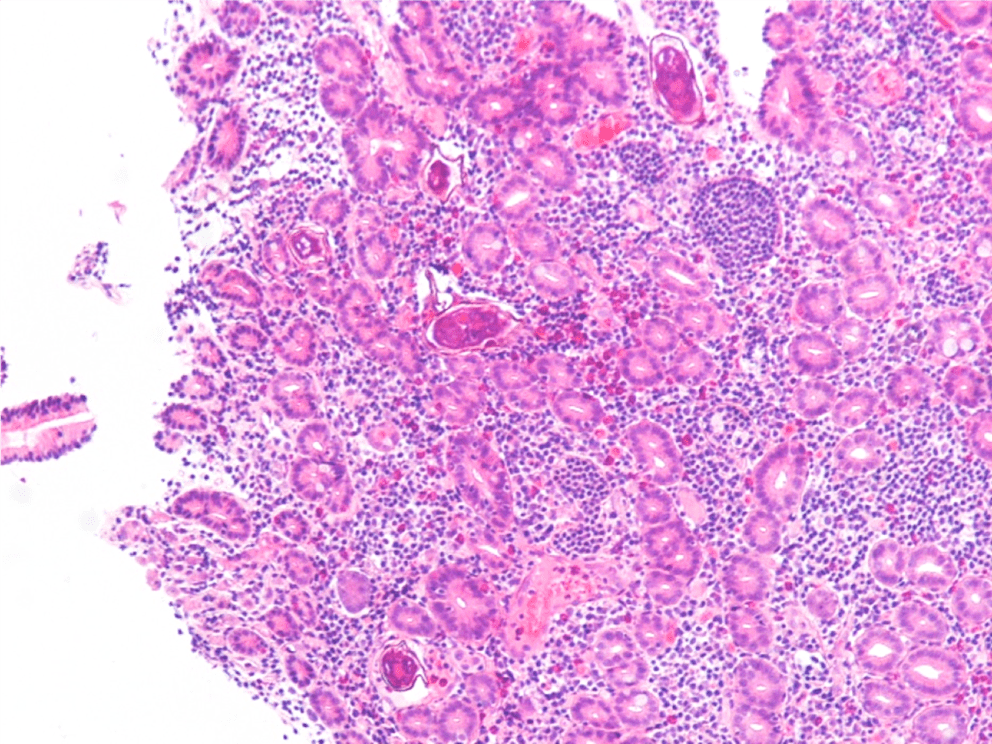
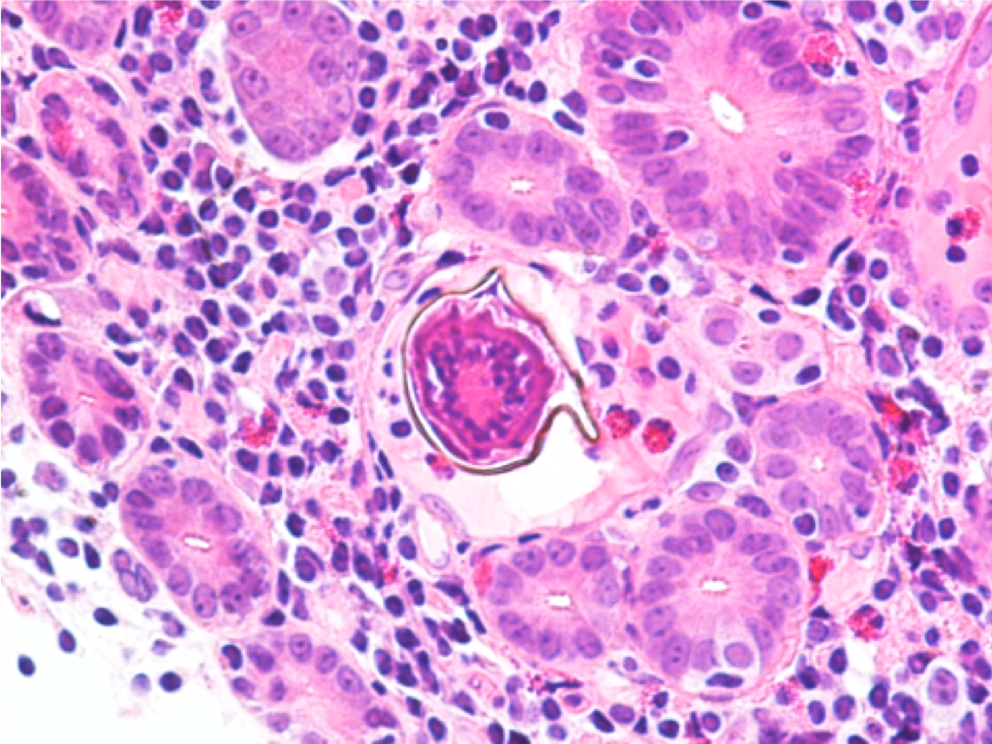
Endoscopy revealed a large, villous, infiltrative mass in the third portion of the duodenum. On histologic examination of the duodenum biopsy, viable Schistosoma eggs were seen within the vessels in the lamina propria and associated with adenocarcinoma (Images 1 and 2). Schistosomamansoni eggs were identified on stool ova and parasite exam (Image 3), and serology was positive for Schistosoma IgG antibody.
Image 1. 10x objective magnification of a hematoxylin and eosin stained histology slide of the duodenal biopsy with associated adenocarcinoma and multiple eggs can be visualized.Image 2. 40x objective magnification of a hematoxylin and eosin stained slide from the duodenal biopsy of a man from Africa who presents with abdominal pain who is found to have a mass on endoscopy. Seen is a viable egg with intact miracidium and no evidence of calcification.Image 3. 100x oil immersion objective magnification of an iodine prep from a concentrated formalin-fixed stool specimen demonstrating a Schistosoma mansoni egg with its characteristic large lateral spine.
Discussion
Although this is not a common infection to encounter in the US, prevalence in endemic areas ranges from 30-100%. Infection occurs through contact with water contaminated with human feces; common circumstances are irrigation ditches as well as bathing and washing water.1
Schistosomiasis may be an indolent infection in many immunocompetent hosts. Chronic infection requires a shift from inflammatory TH1 response to a modulatory TH2 response.2 There is also evidence that Schistosoma infection may downregulate the immune response by inducing M2 differentiation of macrophages.3 These anti-inflammatory macrophages have been associated with a microenvironment favorable to malignancy. It has also been shown that S. mansoni is a risk factor for hepatocellular carcinoma (HCC) and colonic adenocarcinoma, possibly by altering p53 activation, initiation of chronic granulomatous response that blocks venules, increasing cell turnover, and promotion of ROS and RNOS production.4 Anti-idiotype antibodies produced in chronic infection may also down-regulate both specific and non-specific immune responses.5
This case is an unusual presentation in the US in that viable ova are typically not seen, and S. mansoni is more likely to involve the distal colon and liver rather than the small bowel. There is a known association between S. mansoni infection and HCC, and there are sporadic reports of association with tumors of the prostate, ovary, uterus, and cervix.5,6 To our knowledge however, there are no other reported cases of duodenal adenocarcinoma with concurrent schistosomiasis.
References
Chai J and Jung B. Epidemiology of Trematode Infections: An Update. 2019. Adv Exp Med Biol. 1154:359-409.
Barsoum RS, et al. Human Schistosomiasis: Clinical Perspective: Review. 2013. Journal of Advanced Research. 4:433-44.
Hussaarts L, et al. Chronic helminth infection and helminth-derived antigens promote adipose tissue M2 macrophages and improve insulin sensitivity in obese mice. 2015. FASEB J. 29(7):3027-39.
El-Tonsy MM, et al. Schistosoma mansoni infection: Is it a risk factor for development of hepatocellular carcinoma? 2013. Acta Trop. 128(3):542-7.
Palumbo E. Association Between Schistosomiasis and Cancer. 2007. Infectious Diseases in Clinical Practice. 15(3):145-8.
Peterson MR and Weidner N. Gastrointestinal neoplasia associated with bowel parasitosis: real or imaginary? 2011. J Trop Med. 2011:234254.
-Daniel Welder, MD is a second year Clinical Pathology resident at UT Southwestern Medical Center in Dallas, Texas. He has interests in Hematopathology, Transfusion Medicine and dabbles in Microbiology.
-Dominick Cavuoti, DO is a Professor at UT Southwestern in the Department of Pathology. He is multifaceted and splits his time as the Medical Director of the Parkland Hospital Clinical Microbiology Laboratory and Parkland Cytology attending among other administrative and educational activities.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
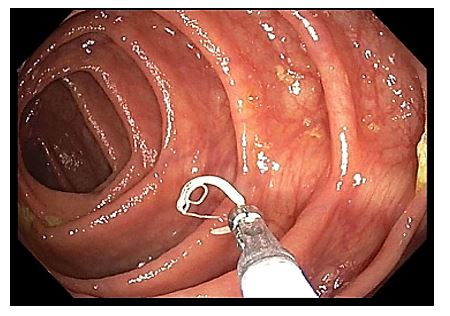
A 52-year-old female with no significant past medical history is seen for a routine annual examination and is scheduled for a colonoscopy due to her age being over 50 years. The colonoscopy was performed and an isolated single worm was found within the cecum (Images 1-2). The worm was removed with cold forceps and subsequently placed in paraffin and sectioned (Images 3-5).
Image 1. The worm is depicted within the cecum attached to the mucosal wall by its anterior end. Image 2. The worm is captured using cold forceps. Image 3. Hematoxylin and eosin stained section of the worm.Image 4. Higher power magnification, showing eggs with distinctive characteristic bilateral polar plugs and barrel shape.Image 5. Higher power magnification, showing eggs with distinctive characteristic bilateral polar plugs and barrel shape.
Discussion
The worm was identified as Trichuris trichiura. The common name for this organism is the whipworm. It belongs to the Nematode classification of parasites, which are commonly referred to as roundworms. Adults measure up to 5 cm in length and have a tapered or whip-like anterior end. The eggs measure 50 x 25 µm, and have brownish thick shells on stool smear. The eggs also have a barrel shape and distinctive protruding polar plugs at each end. These morphologic characteristics of the egg are diagnostic of Trichuris trichiura. The lack of a tissue migration phase and a relative lack of symptoms characterize whipworm infection, with only those with a heavy parasite burden becoming symptomatic. If these symptoms do arise, they are usually mild, ranging from loose stools with minimal blood loss and nocturnal stools, to iron deficiency anemia and vitamin deficiency. As parasite burden increases, however, symptoms can progress to dysentery, colitis, or rectal prolapse. Prolapse is more frequent in the Pediatric population, but has been described in adults as well.
Trichuris trichiura has one of the simplest of the Nematode life cycles. Eggs are unintentionally ingested, hatching in the small intestine by way of exploitation of signaling molecules from the intestinal microbiome. The larvae then burrow through the villi and continue maturing in the wall of the small intestine. They then return to the intestinal lumen, migrating to the cecum and subsequently into the large intestine, where they finish the process of maturation. Finally, the worm uses its anterior end to anchor into the bowel mucosa, where it feeds on tissue secretions and uses its posterior end for reproduction and laying eggs. Female worms can live from 1-5 years and can lay up to 20,000 eggs per day.
Whipworm infection is principally a problem in tropical Asia and, to a lesser degree, in Africa and South America. Children are most commonly infected, and can experience failure to thrive as well as cognitive and developmental defects. Transmission is by the fecal-oral route, explaining the large incidence of infection in children from developing countries, as they are far more likely to be in physical contact with soil and environmental contaminants, with subsequent placement of their fingers in their mouths. The fecal-oral route can also be facilitated by improper washing and cooking of fruits and vegetables, as well as overall poor hygiene, no matter what the geographical location. In the United States, whipworm infection is exceedingly rare. When it does happen, it is most commonly seen in the rural Southeast. Although it is rare, the incidence of infection is reported to be as high as 2.2 million individuals within the United States, with 1-2 billion cases worldwide.
Studies often reveal eosinophilia in nematode infections from ongoing tissue invasion. However, the lack of a tissue migration phase in Trichuris life cycles makes this a rare laboratory finding. Other studies such as anemia can give an indication to the presence of the worm. Characteristic egg morphology on stool smear remains the cheapest and easiest way to diagnose infection, but polymerase chain reaction using new sequencing techniques are now available in some laboratories to detect the presence of Trichuris with great sensitivity and specificity. The parasite burden can be quantified per gram of stool by the Kato-Katz technique. This procedure filters stool through mesh, with the filtered sample being placed within a template on a glass slide. The template is then removed and the remaining fecal material is removed with a piece of cellophane soaked in glycerol, leaving only eggs on the slide.
Discovery of T. trichiura in our patient was an unexpected finding, as our patient had no symptoms. Asymptomatic detection of T. trichiura has been described in the past, so this finding is not unique. The medication of choice is mebendazole, showing a cure rate of 40-75%. The drug works well by inhibiting glucose uptake from the gastrointestinal tract of the helminth. However, this drug is very expensive, and as a result is difficult to obtain. The patient is currently receiving an alternative drug called albendazole as outpatient therapy and will be switched to mebendazole as soon as resources become available should the need remain. The patient is following up with her primary care physician and is expected to make a full recovery.
Sunkara T, Sharma SR, Ofosu A. Trichuris trichiura-An Unwelcome Surprise during Colonoscopy. Am J Trop Med Hyg. 2018 Sep;99(3):555-556. doi: 10.4269/ajtmh.18-0209. PubMed PMID: 30187847; PubMed Central PMCID: PMC6169157.
-Cory Gray, MD is a second year resident in anatomic and clinical pathology at the University of Chicago (NorthShore). His interests include hematopathology and molecular and genetic pathology, as well as medical microbiology.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
According to this recently-published study in the Journal of Histotechnology, ” … experts are confident that 70% ethanol and 0.1% sodium hypochlorite should inactivate the virus. Formalin fixation and heating samples to 56oC, as used in routine tissue processing, were found to inactivate several coronaviruses and it is believed that 2019-nCoV would be similarly affected.”
The FDA is now democratizing the testing of the novel coronavirus: SARS-CoV-2 (the virus which causes the COVID-19 disease syndrome—I will call it COVID-19 from here on as that is the colloquial name most people know) by allowing high complexity testing labs across the United States. This move will permit more labs to test for COVID-19. A previous post by contributor Constantine Kanakis describes the biology of the virus, so I will not repeat that material. Instead, I will focus on some considerations in validating a Lab Developed Test (LDT) COVID-19 molecular assay.
The president of AACC, Carmen Wiley, said there are 11,000 high complexity testing labs in the US, which could qualify for performing this testing. However, not all of these labs have molecular and virology expertise, so others have placed the number of labs with qualified staff and instrumentation at 400.
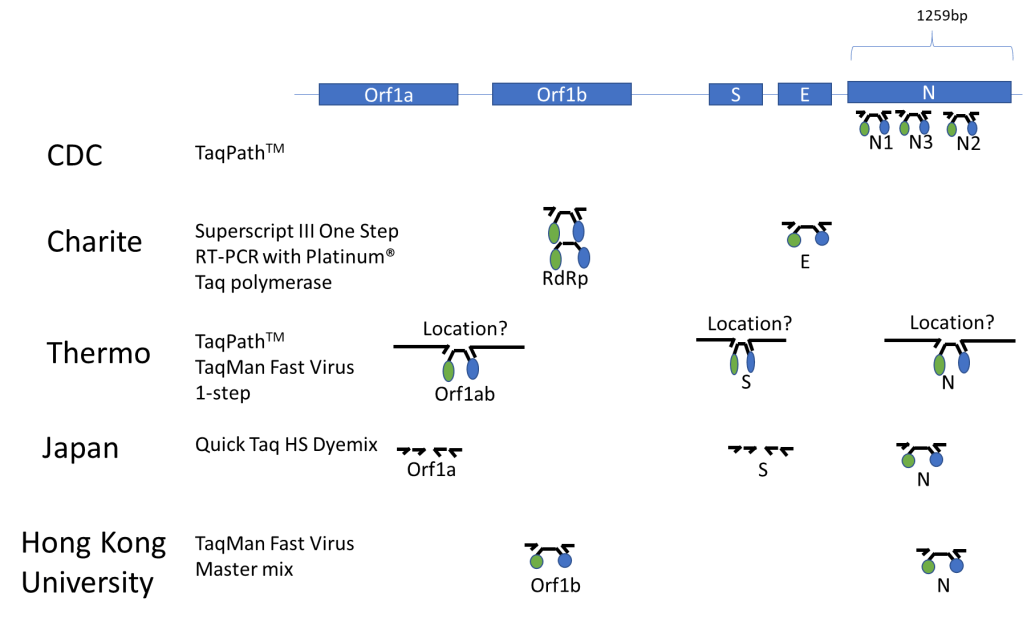
Published Assays and Targets: As an overview, the figure below (Figure 1) summarizes some published COVID-19 assays. As you can see, the major strategy involves using the TaqMan probe strategy where a short probe is degraded by Taq polymerase releasing a fluorescent molecule (green ball) from a quencher molecule (blue ball). The TaqMan approach allows for quick performance of the assay and easy interpretation. One lab from Japan is using nested PCR amplification and sequencing of the Orf1a and S genes as well.
Figure 1. The COVID-19 genetic structure is abbreviated above with the different genes targeted displayed. The names of institutions that have published their assay procedure along with the TaqMan reagents that were reportedly used with each assay are shown above. Primers are represented by small arrows with a TaqMan probe in the middle represented by a black line with green and blue circles indicative of the fluorescent molecule and its quencher. The double set of arrows for the Japanese assay represents a nested PCR strategy.
In silico Cross-reactivity:
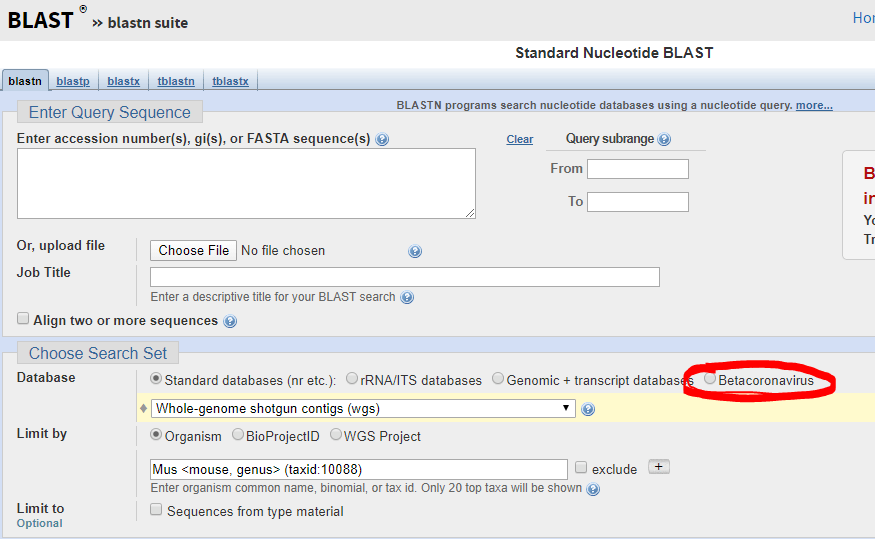
The FDA guidance allows cross-reactivity to be minimally assessed in silico by demonstrating “greater than 80% homology between primer/probes and any sequence present in the targeted microorganism.” The primer locations can be found in the publication of each protocol (except Thermo) and can be confirmed by checking the NCBI Blast site and they actually have a selection for beta-cornavirus (Figure 2) now that allows you to search for your primer’s reactivity across other related viruses- Very helpful!
Figure 2. Select Betacornavirus before entering your primer/probe sequence to confirm cross-reactivity.
Primer/Probe Design:
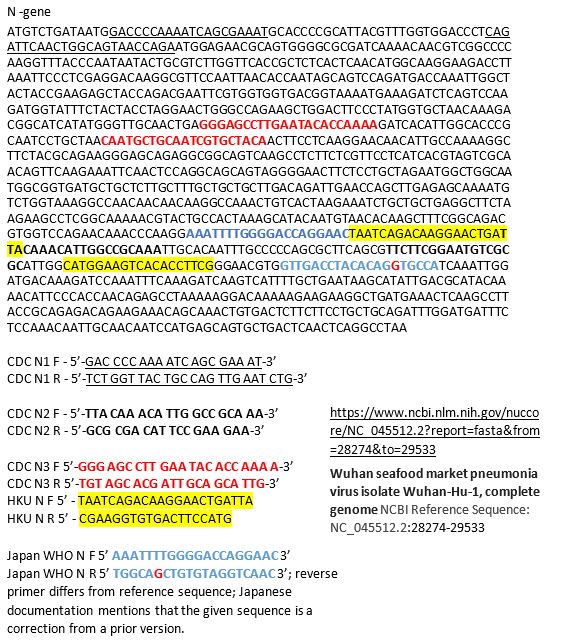
The N region is the most popular site to probe and is included in most kits once and the CDC kit three times. It was the reagent set for N3 in the CDC kit that was having difficulties, so you may decide to not include that component in your LDT. If you want to see how the different available primer sets align on the N gene sequence you can see below for the primers labeled based on their source. Many are overlapping, perhaps because many people thought the same site was a good target (Figure 3).
Figure 3. N-gene of COVID-19 along with labeled primers from some published assays. The information on the source of the sequence is shown on the bottom right with the link.
Commercially Available Assays:
An important part of validating your COVID-19 assay is to do so quickly. Thus commercially available kits would be helpful, however there are only two commercially available sources at this time: IDT and Thermo. IDT is producing a kit with the CDC design. Thermo produced their kit over the last few months and does not have any published validation information that I could find. Also Thermo when I checked just now for the catalog number, it says this product is unavailable… not sure what that means, but maybe you can try contacting them. Both IDT and Thermo list control plasmid reagents for their assays.
Controls for the Assay:
The wording of the FDA announcement was interesting in that it 1) did not require clinical samples, but allows “contrived clinical specimens.” “Contrived reactive specimens can be created by spiking RNA or inactivated virus into leftover clinical specimens.” A major difficulty is the access to actual COVID-19 RNA or inactivated virus. I noticed that the guidance didn’t say that the assay MUST use RNA. Thus most labs would have access to plasmid DNA, which could potentially be used.
Given the limited availability of RNA for validation use, a lab may consider performing much of the assay optimization with COVID-19 Plasmid DNA while waiting for access to RNA. I would like to be sure my assay could extract, amplify and detect RNA as part of the clinical validation.
Asuragen can produce Armored RNA, with synthetic RNA packaged inside of a viral capsid, which would be a useful control for extraction, amplification and detection. However, we heard this will not be available for another month.
Tom Stenzel (director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health (CDRH)) said FDA, BARDA, and the CDC will prioritize and coordinate shipments of viral materials to labs when they are ready to validate tests according to a webinar with labs on Monday. Currently, the FDA is directing inquiries to BEI, which is reportedly prioritizing requests to send out samples in 12-72 hours.
Lastly, one could try to use in vitro synthesized RNA sequences surrounding your primer targets as a control for now and may have better luck in getting the product soon. This is the control that is being shipped with the CDC kits to public labs.
Limit of Detection is an unknown for what is likely to be clinically relevant as we don’t know what the levels look like in people with early vs. late vs. severe vs. mild disease. The FDA just says you should be able to detect 95% of samples (19 of 20) that are x1-x2 the limit of detection.
FDA Notification:
This is the final and important step. Once you go live, you must notify the FDA with an Emergency Use Assay (EUA) form within 15 days. Reviewing the form, there doesn’t appear to have complex explanations or overdue requirements for reporting, which wouldn’t be found in a standard lab validation document.
Final Thoughts/Future commercial solutions:
This information is the best of what I know right now based on current information- this is not a complete guide and the FDA guidance should be read closely for all compliance details.Information is changing quickly and is likely to change more if the number of COVID-19 cases in the United States increases. Cepheid, Luminex, and BioFire are reportedly working on assays that will be out in several months and would be easy to use for many labs that already have one or both of these systems-however it may require a full validation for an LDT, but I’m not sure as it is an EUA-further clarification on this point is needed. Although there are several commercial solutions available, we don’t know how demand could impact supply from each company. Fortunately, some large reference labs like LabCorp and Quest are looking to develop a COVID19 test. Good luck, stay safe, and feel free to contact me with any questions in the comments below so that everyone can benefit from the discussion!
References
In lieu of a list of references, I’ve included web links for the most current and direct sources of information.
-Jeff SoRelle, MD is a Chief Resident of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and improving genetic variant interpretation.
The Food and Drug Administration (FDA) issued new guidance on February 29, 2020, for laboratories to be able to develop novel coronavirus (COVID-19) molecular diagnostics tests and begin use prior to obtaining Emergency Use Authorization (EUA). This permits laboratories that are CLIA certified and meet requirements to perform high complexity testing to start offering severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) molecular diagnostic testing after validation is completed as outlined in the guidance. Laboratories should submit an EUA request to the FDA within fifteen business days after validation. FDA will be hosting a webinar to provide more information on March 2, 2020, at 3 pm ET.
Clinical laboratories should contact their state health departments for guidance if they have a suspected COVID-19 case specimen. Clinical laboratories should NOT attempt viral isolation from specimens collected from COVID-19 persons under investigation (PUIs). For interim guidelines for collecting, handling, and testing clinical specimens from PUIs for COVID-19, please see the CDC Coronavirus Disease 2019 (COVID-19) website.
A 52 year old patient with a history of recent travel to India presented to interventional radiology from an outside hospital for aspiration of a liver abscess, and was subsequently returned to the outside hospital. The patient had spent 2 months in India before returning to the US, and about 1 month later developed right upper quadrant pain. Abdominal CT showed 2 cystic masses measuring 2-4cm. Aspiration of the cysts yielded 0.5mL of bloody fluid, which was sent for bacterial culture and smear. Infectious disease prescribed antimicrobial treatment consisted of ceftriaxone and metronidazole, followed by paromomycin and levofloxacin.
Laboratory findings
A gram smear of the patient’s liver mass aspirate showed few neutrophils and no bacteria. Culture of the aspirate showed no growth at 5 days. Multiple sets of blood cultures collected at the outside hospital all showed no growth at 5 days.
Image 1. Entamoeba coli trophozoite seen in the patient’s stool ova and parasite exam, demonstrating an eccentric karyosome and coarse, irregular peripheral chromatin.
A single ova and parasite exam of the patient’s stool was sent and showed few Entamoeba coli trophozoites. A sample of the patient’s blood was sent to the Mayo reference lab for serum Entamoeba histolytica antibody testing, which came back positive. Stool was sent for Entamoeba histolytica antigen testing which was negative.
Discussion
Entamoeba coli is a non-pathogenic protozoan that can exist as a commensal organism in the human gastrointestinal tract. This organism has not been established to have any disease causing effect per se, but its presence may indicate exposure to water sources that could contain parasitic organisms. (3)
Entamoeba histolytica, by contrast, is a parasitic protozoal pathogen. Most infections are asymptomatic, but they can manifest as amebic dysentery or extraintestinal disease. The most common extraintestinal manifestation is amebic liver abscesses.1
Intestinal amebiasis occurs via ingestion of amebic cysts, typically through contaminated food or water, but also through other forms of fecal-oral contact. Infections are seen most commonly in areas with poor sanitation, but can be found in developed countries in patients who have migrated from or traveled to endemic areas.2
Once the amebic cysts pass into the small intestine, they form trophozoites, which are able to penetrate the mucous barrier of the gut and destroy intestinal epithelial cells. This leads to blood and mucus in the stool. (2) Once the amebae penetrate the gut wall, they are able to reach the blood and ascend through the portal system to the liver and form amebic liver abscesses.3
Clinical presentation of these abscesses typically includes right upper quadrant pain and fever in a patient with a history of travel to an endemic area. Serologic testing is used for confirmation if clinical presentation and imaging are suggestive, but this cannot distinguish between current infection and prior exposure, and up to 35 percent of uninfected inhabitants of endemic areas show positive serology.3 Stool microscopy may be the initial, and indeed only test available in some areas, but cannot differentiate E. histolytica from non-pathogenic E. dispar and E. moshkovskii strains.2
Image 2. E. histolytica trophozoite with ingested red blood cell, visible as a dark inclusion, as well as demonstrating a central karysome and fine, uniformly distributed chromatin. (CDC: https://www.cdc.gov/dpdx/amebiasis/index.html) Erythrophagocytosis is suggestive of E. histolytica.
Empiric treatment in the setting of consistent epidemiology, clinical picture, and radiology consists of metronidazole or tinidazole for tissue clearance followed by paromomycin, diiodohydroxyquin, or diloxanide furoate for intraluminal clearance.
Infectious diseases was taking care of this patient and decided her clinical syndrome is probably extraintestinal Entamoeba histolytica amoebiasis based on the results of the CT findings and the antibody in the right clinical setting. Although her stool ova and parasite only showed Entamoeba coli, she clearly has been exposed to contaminated food or water. In addition, the Entamoeba histolytica stool antigen was negative, but this can be an insensitive test.
-Tom Koster, DO is a 1st year Anatomic and Clinical Pathology Resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
Patient advocates are simply people who care about patients as fellow human beings enough to act on that care. Forensic pathology fascinates many people, but hardly anyone realizes how strongly forensic pathologists advocate for patients.
Forensic pathologists have the responsibility of identifying human remains and determining the cause and manner of death for individuals that die suddenly and unexpectedly. Most often, we accomplish this mission by performing an autopsy. Death makes many people uncomfortable, and we’re accustomed to grim jokes about their work when meeting someone. Typically these comments carry an undertone that because decedents cannot talk, we don’t need interpersonal skills. Not only is this untrue, comments such as these provide an educational opportunity.
It is true that our patients have already died, but the relatives of our patients are very much alive. Those relatives have needs that we work to provide and questions we strive to answer. The most common question relatives have is “Why did my loved one die?” which is precisely what the pathologist is working to determine. We regularly talk with relatives of decedents that we’ve examined. We can tell family members why death occurred, including any implications that the death has for remaining members of the family. We can also help families begin to work through the social and bureaucratic requirements that death brings for those still living, such as the need to make arrangements for the disposition of the body and the need for a death certificate. (For example, after a person dies, that person’s financial accounts are frozen until a death certificate becomes available to unlock the accounts.)
Forensic pathologists work to develop a good relationship with the decedent’s relatives. Because anger and bargaining are part of grieving, conversations with relatives sometimes begin as though the relative and the pathologist are adversaries, but with time and compassion, the relationship usually transforms into a more appropriate professional relationship. A particularly important aspect of family interactions is listening to a grieving relative, because listening with care helps someone who is grieving. Attempting to build a good relationship with the decedent’s relatives does not mean that the pathologist is a blind advocate for the family. We won’t change the cause of death so that the family can reap more financial benefit from the death, for example. Lies will not help someone pass through the process of grieving in a healthy way – truth, time, and patient, loving care are the necessary therapeutic measures.
In the case of homicides, forensic pathologists advocate for the decedent by calling the death what it is and then testifying to the medical facts of that death when a suspect is tried in court. The pathologist testifies to the medical aspects of what caused death without trying to ensure that the suspect is either convicted or acquitted. Trying to sway the jury’s verdict is the work of attorneys; presenting the medical facts of why and how the decedent died is the work of the pathologist.
Forensic pathologists advocate for public health by providing an accurate cause of death. Death certificate data provide an essential component for assessing public health, and those data are an important determinant for allocation of medical research funds and for interventions to improve public health.
Like other pathologists, forensic pathologists typically do their work quietly in the background, advocating for their unique patients in their own special way. People give little thought to professional interactions with a forensic pathologist until forced to do so; in that difficult time we try to serve as best we can.
-Gregory G. Davis, MD, FASCP graduated from Vanderbilt Medical School and trained in pathology at Vanderbilt University Medical Center, Nashville, TN, followed by a fellowship in forensic pathology at the San Diego County Medical Examiner Office in San Diego, CA. Dr. Davis then joined the faculty at the University of Alabama at Birmingham, where he currently serves as a Professor and as Director of the Forensic Division of the Department of Pathology. Dr. Davis also serves as Chief Coroner/Medical Examiner for Jefferson County, Alabama, the county in which Birmingham is located. Dr. Davis has earned a Master of Science in Public Health from the UAB School of Public Health. His research interest is the application of epidemiology to the study and practice of forensic pathology, especially drug abuse. He has published 74 peer-reviewed manuscripts, including serving as lead author on the 2013 opioid position paper of the National Association of Medical Examiners. He is currently working as chair of a panel revising and updating the NAME opioid position paper for expected publication in 2020. He serves on the editorial boards of the Journal of Forensic Sciences and Forensic Science, Medicine, and Pathology. Dr. Davis is a Fellow At-Large Director on the Board of Directors of the American Society for Clinical Pathology.
No, I’m not talking about Netflix or HRH Queen Elizabeth II, nor am I making references to tiaras, bars, beer brands, or imminently deliverable babies…I am, of course, talking about Coronavirus as it would certainly have caught most of our collective attention in the media by now.
I really enjoyed writing last month’s list of what I think are important things on the horizon for pathology and laboratory medicine this new year, but this month let’s take a more topical turn. So put your surgical masks on, wash your hands, quarantine the next 10 minutes of your time and get ready as I take a shot at the novel 2019 coronavirus outbreak!
***Let’s talk about you and me, Let’s talk about COVID-19…***
Less-Than-Common Cold
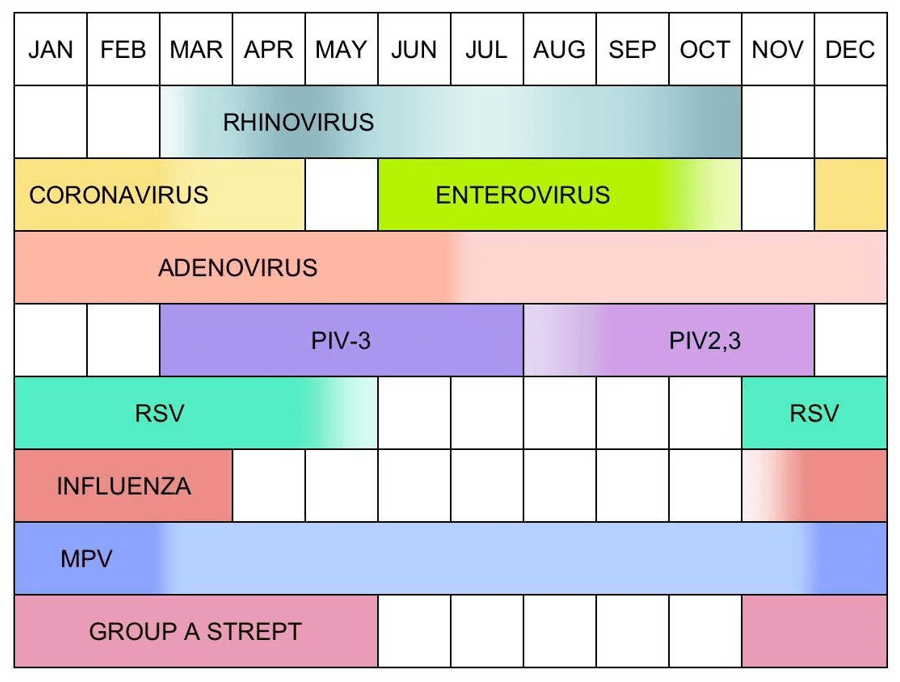
A long time ago, in a galaxy far, far away (aka: last year, about 20 minutes north of my apartment in Manhattan) I was in medical school, on rotations on the floors of a hospital in the Bronx. I experienced the surges of two flu-seasons and had a fantastic little mnemonic to remember the viruses that caused colds in most patients. Depending on age and immune system status, you had to think about the principal three viruses we see all the time—I remembered them as: “c-A-r,” note the capital “A.” Let me explain; the letters correspond to coronavirus, adenovirus, and rhinovirus. The are in a general order of when they appear during the months of the year (as coronavirus and rhinovirus kind of switch off in the spring, while adenovirus is around always thus is capital designation). There are a few hundred viruses which contribute to cold/flu-like symptoms in patients and, unless a patient is compromised in some way, we really worry most about one of them. Hint: it’s the one we give shots for annually, more on that in a minute.
Image 1. Okay this is a little better than my seasonal cold “cAr”…Seasonal variations in frequency of selected upper respiratory tract infection pathogens. Funny that, of all the colors, Influenza gets the good ‘ol fashioned “red alert” from the commanders on the USS Medscape. PIV = parainfluenza virus; RSV = respiratory syncytial virus; MPV = metapneumovirus; Group A Strep = group A streptococcus. (Source: Medscape)
As far as this coronavirus outbreak is concerned, this is a “novel” (i.e. new) variant (read: mutation) of a respiratory viral pathogen that is affecting a disproportionate number of patients in higher severity than expected. Its official entity name has now been filed by the World Health Organization (WHO) as COVID-19—corona virus disease of 2019. The actual virus is a relative of the infamous SARS virus from the early 2000s. That was SARS, this is SARS 2.0—literally. This virus is designated SARS-CoV-2. SARS stands for Severe Acute Respiratory Syndrome and is caused by strains of coronavirus found in the remnants of infected individuals’ coughs and sneezes—please wash your hands—and causes a spectrum of symptoms from mild to severe including pneumonia, respiratory disease, and even renal failure.
Image 2. Heeeerrreee’s COVID, well at least a coronavirus model. Named after the crown-like spikes on its envelope surface which act as receptor anchors in order to attach to cells and infect us. The receptors’ favorite target? ACE2 (angiotensin converting enzyme 2) receptors—am I getting your blood pressure up yet? I said renal failure…full circle, right? (Source: Centers for Disease Control and Prevention)
How Does this Even Happen?
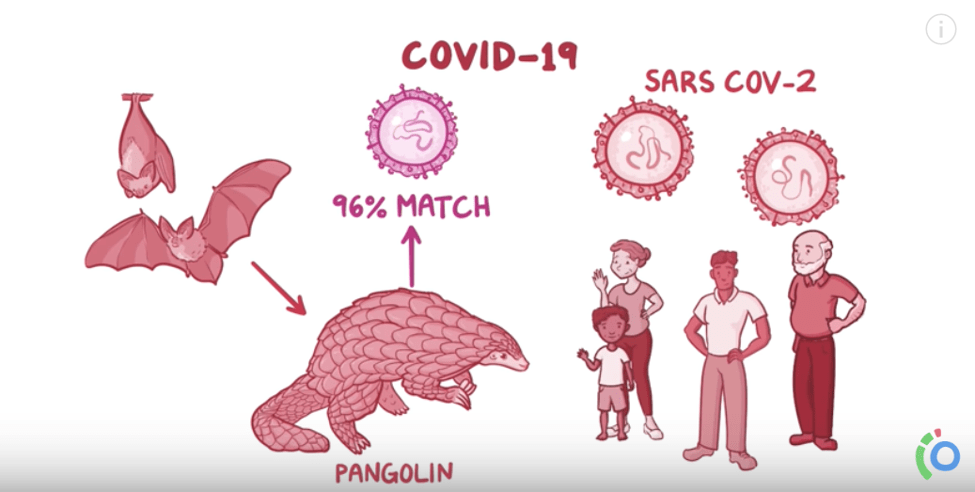
Okay, who took a sabbatical to Wuhan, China, and ate a wild fruit-bat salad? No one, that’s not how this works. But, if you’re looking for quick grocery store recommendations at the present moment I’d probably tell you to check out ALDI or a farmer’s market a few spots higher on the list than the Huanan Seafood Wholesale Market in Wuhan which harbored a majority of outbreak case-cause tracings. The bottom line is that COVID-19 and the SARS-CoV-2 have appeared in the world the same way the previous similar outbreaks have—through zoonotic mutations which then spread to humans. This zoonotic transmission is so effective to presenting humans with super infectious entities because it sends us pathogenic material we would have never seen before and our “naïve” immune systems are caught off guard. Now don’t get all panicky; yes, I’ve seen Contagion, Outbreak, and read The Andromeda Strain—in fact, I absolutely love when epidemiological medicine has the media spotlight. It’s a very exciting way to showcase public health, medicine, and—our favorite—laboratory professional work!
Image 3. Okay, no bat salad but this outbreak does involve bats endemic to the regions in question. It also involves, pangolins, kind of like armadillos, which are bought and sold (and trafficked) all around the world for various reasons. The pangolin DNA matches the SARS-CoV-2 genome highly, so scientists assert that its involvement is inherent. The complications in sanitation and animal/food handling are obviously implicated in this and other outbreaks, but dealing with COVID-19 requires a strong public health response. (Source: Osmosis)
Basically, this process of mutation and transmission is the modus operendi of a viral particle. You can’t quite kill them, they’re not quite alive by biological definitions, they’re just packaged proteins on autopilot. They’re kind of like natural robots that want to propagate their species by adapting over time—they’re The Borg or Cybermen, depending on your sci-fi preferences. But both offending automaton predators have a mutual enemy in public health—a doctor (get it? TARDIS pilot and/or Beverly Crusher both work wonders in a pinch…) Anyway, it’s never just physicians, but a whole hard-working team of health advocates that conduct surveillance, field research, epidemiologic studies, and first-hand treatment.
***Side note: if you’re bored, in a hurry, or just don’t like my articles—don’t fret! Go watch that Osmosis video on COVID-19 and you’ll be up to snuff on the current outbreak in no time. Or in 12ish minutes.***
***Hey, you made it this far. Great! Interested to know more about the COVID-19 virus from our very own American Journal of Clinical Pathology? Visit here to learn more about the story of how this pesky coronavirus mutated its way into headlines. Fresh off the AJCP presses this month!***
You Should Update Your Antivirus Software
Image 4. Fake news is the new normal. It’s hard to sift through a sea of garbage. You can’t just ignore it, because sometimes there’s serious situations like war—or viral pandemics! So, you’ve got to update your personal mental anti-spam filter and know how to sniff out suspicious sources. Let’s call it “information hygiene” to be consistent with the zoonotic exposure narrative, yea? (Image source: NPR)Image 5. Let’s lighten the mood a bit. These situations can drive folks absolutely nuts. People obsess over minutiae and often wrong details when archetypal preventions like hand-washing and isolation are paramount to prevent epidemics. Public health and pandemic situations breed conspiracy thinking—wait, never mind, this is a photo of me explaining the residency match process to my friends and family. Kidding. Kind of. (Source: a popular meme, but originally from It’s Always Sunny in Philadelphia)
No doubt in my mind you’ve probably seen plenty of coverage about SARS-CoV-2 in the media. I’d also be willing to bet a lot of it is either dilute, sensational, or possibly even misleading. Regardless, there are always going to be people that don’t “buy in” to the public health message. If you remember Contagion¸ Jude Law’s character pushes the efficacy of “forsythia,” a homeopathic herb supplement that supposedly mitigates the horrible disease spread from southeastern Asia from improper food handling—if I recall correctly, it was a paramyxovirus that time. In this SARS-CoV-2 epidemic we have no current effective treatments, so prevention is key.
In an effort to address this type of health misinformation the WHO and CDC are actively disseminating as much educational information and graphics as they can write. Trying to dispense advice for the public including proper mask wearing, education videos, and myth-busting (i.e. hand dryers do NOT kill the COVID-19 virus, UV lamps do NOT kill the virus, thermal readers are effective in screening populations for symptoms within limitations, alcohol and chlorine do NOT kill the virus, receiving packages from China is still safe, pets don’t harbor the virus at this time, other vaccines do not affect this virus, saline nose sprays do not affect this virus, garlic/oils/other supplements have no effect on this virus, and all age groups are affected)—good stuff there. The most trusted sources of information regarding epidemics should be the representatives of functional medicine and health outcomes, doing work every day to make people healthier. Often times, politics, misinformation, or complex situations make information delivery harder than you’d think and the risks are increasingly high.
Image 6. BONUS MATERIAL UNLOCKED: Glad you made it this far. I mentioned Netflix’s The Crown above, but if you’re looking for a fantastic series that breaks down public health epidemiology, influenza burden, research and surveillance on emerging pathogens as updated as 2019, check out Pandemic. 5/5 surgical masks would binge again. (Source: Netflix)
A Crown of Thorns: Don’t Forget About the FLU!
Flu vaccine deniers: turn away now or be healed! —or at least exposed to another point of view rooted in evidence-only concepts in medicine and population health. Consider the following: as of this month, COVID-19 has infected 43,000 people and killed 1,000 (approximately 2-3%). Remember SARS? That infected 8,000 and killed 700 (approximately 10%). MERS? 2,500 infected, 860 deaths (approximately 34%). And what about Ebola? 29,000 infectious cases with 11,000 deaths (approximately 40%). That was sourced from the Osmosis video with data from the WHO. Pretty impressive right? Well, not if you look at this: according to the CDC, the 2019-2020 influenza burden statistics include 36,000,000 infectious cases, with 17,000,000 clinical visits, 440,000 hospitalizations, and 36,000 deaths. One might say “hey, Dr. Kanakis, slow down there you’re spitting out all these numbers and the facts won’t lie. Looks like influenza only killed 0.1% of cases.” And you know what, you’re right. 0.1% is lower than the other viral epidemics. But check this out, because of the sheer number of cases, that means more people died of influenza than COVID-19, SARS, MERS, and Ebola COMBINED and those happened in other years. That‘s just this year’s flu season alone. I’ve talked before about recognizing and detecting the common cold vs. influenza before, check it out if you’d like a refresher!
Image 7. What’s a statistical percentage data point if it’s a relative, a loved one, or yourself? Protect yourself, protect others, and let’s find ways to make proper health knowledge available and acceptable to the masses while promoting excellent healthy behaviors, together! (Image source: New York Post)
We have influenza every single year, and it kills so many more people than we realize. If you want to talk about a terrifying, global viral epidemic, we’ve already got one. And it’s closer than you think. So wash your hands, reduce exposures if you’re sick or immunocompromised, get proper rest, eat well, exercise, read my articles every month, but most importantly—and I cannot stress this enough—get your FLU SHOT!
Thank you so much, see you next time!
–Constantine E. Kanakis MD, MSc, MLS (ASCP)CM completed his BS at Loyola University Chicago and his MS at Rush University. He writes about experiences through medical school through the lens of a medical lab scientist with interests in hematopathology, molecular, bioethics, transfusion medicine, and graphic medicine. He is currently a 2020 AP/CP Residency Applicant and actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Follow him on Twitter @CEKanakisMD