Case History
A 41 year old African male presented to the ED with complaints of abdominal pain, weight loss, and decreased appetite over one month. He immigrated from Zimbabwe 10 years prior, and most recently visited 4 months ago. His past medical history is non-contributory. He was found to have microcytic anemia (Hgb 9.3 g/dL, MCV 77.0 fL), pneumonia, and focal small bowel dilation with thickening and inflammatory changes on abdominal CT.
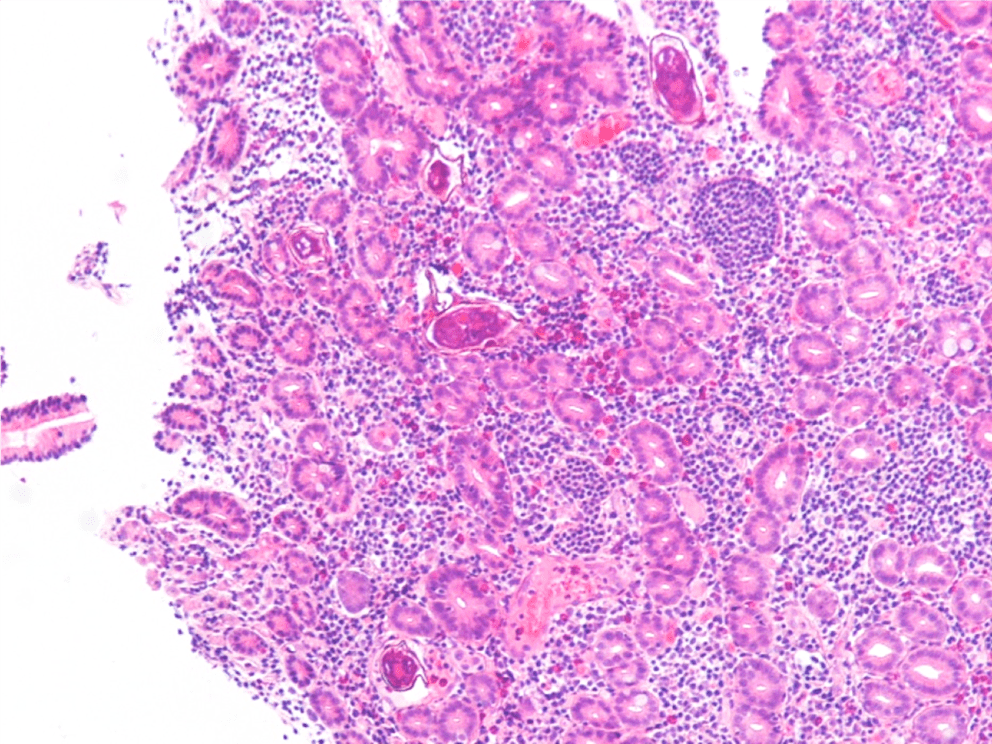
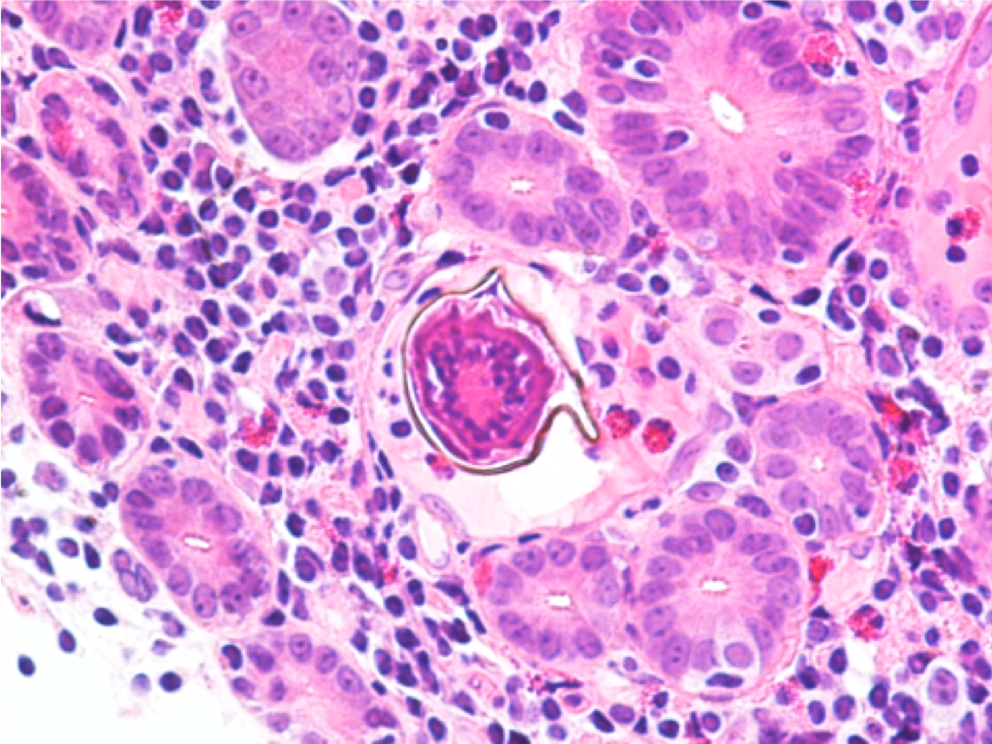
Endoscopy revealed a large, villous, infiltrative mass in the third portion of the duodenum. On histologic examination of the duodenum biopsy, viable Schistosoma eggs were seen within the vessels in the lamina propria and associated with adenocarcinoma (Images 1 and 2). Schistosoma mansoni eggs were identified on stool ova and parasite exam (Image 3), and serology was positive for Schistosoma IgG antibody.

Discussion
Although this is not a common infection to encounter in the US, prevalence in endemic areas ranges from 30-100%. Infection occurs through contact with water contaminated with human feces; common circumstances are irrigation ditches as well as bathing and washing water.1
Schistosomiasis may be an indolent infection in many immunocompetent hosts. Chronic infection requires a shift from inflammatory TH1 response to a modulatory TH2 response.2 There is also evidence that Schistosoma infection may downregulate the immune response by inducing M2 differentiation of macrophages.3 These anti-inflammatory macrophages have been associated with a microenvironment favorable to malignancy. It has also been shown that S. mansoni is a risk factor for hepatocellular carcinoma (HCC) and colonic adenocarcinoma, possibly by altering p53 activation, initiation of chronic granulomatous response that blocks venules, increasing cell turnover, and promotion of ROS and RNOS production.4 Anti-idiotype antibodies produced in chronic infection may also down-regulate both specific and non-specific immune responses.5
This case is an unusual presentation in the US in that viable ova are typically not seen, and S. mansoni is more likely to involve the distal colon and liver rather than the small bowel. There is a known association between S. mansoni infection and HCC, and there are sporadic reports of association with tumors of the prostate, ovary, uterus, and cervix.5,6 To our knowledge however, there are no other reported cases of duodenal adenocarcinoma with concurrent schistosomiasis.
References
- Chai J and Jung B. Epidemiology of Trematode Infections: An Update. 2019. Adv Exp Med Biol. 1154:359-409.
- Barsoum RS, et al. Human Schistosomiasis: Clinical Perspective: Review. 2013. Journal of Advanced Research. 4:433-44.
- Hussaarts L, et al. Chronic helminth infection and helminth-derived antigens promote adipose tissue M2 macrophages and improve insulin sensitivity in obese mice. 2015. FASEB J. 29(7):3027-39.
- El-Tonsy MM, et al. Schistosoma mansoni infection: Is it a risk factor for development of hepatocellular carcinoma? 2013. Acta Trop. 128(3):542-7.
- Palumbo E. Association Between Schistosomiasis and Cancer. 2007. Infectious Diseases in Clinical Practice. 15(3):145-8.
- Peterson MR and Weidner N. Gastrointestinal neoplasia associated with bowel parasitosis: real or imaginary? 2011. J Trop Med. 2011:234254.
-Daniel Welder, MD is a second year Clinical Pathology resident at UT Southwestern Medical Center in Dallas, Texas. He has interests in Hematopathology, Transfusion Medicine and dabbles in Microbiology.
-Dominick Cavuoti, DO is a Professor at UT Southwestern in the Department of Pathology. He is multifaceted and splits his time as the Medical Director of the Parkland Hospital Clinical Microbiology Laboratory and Parkland Cytology attending among other administrative and educational activities.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.












