Welcome back everybody! Thank you for all the engagement on my last post, Up In Smoke¸ where I discussed the plenary publications surrounding the vaping crisis and EVALI as new pulmonary pathology entity. This month, let’s start 2020 off right. After the holiday break and going on some of my last pathology residency interviews, I’d like to reflect on this new year by taking a look at 20 exciting things on the horizon for those of us in pathology and laboratory medicine!
So, let’s take a look at 2020 with some 20/20 vision… (sorry, not sorry)
20. Big, big, big, big data

Last year, Elsevier’s Clinical Solutions Director in China discussed three topics that would impact our profession in 2019—so let’s start there. These first three go hand-in-hand in prepping the stage for 2020. Up first: the never-ending explosion of biomedical information and the continuing tidal wave of health data we don’t even know what to do with just yet! It’s a very interesting estimate that, by 2020 (aka now!) the whole sum of medical knowledge will double every 73 days. How on earth are we to manage, when compared to 1950 it would have taken 50 years to double? Well, the argument in the linked Elsevier blogpost discusses how evidence-based inquiry databases will store and organize this knowledge for us: think UpToDate, or ExpertPath, or ImmunoQuery…some of you are nodding your heads in relief, great, I’ll move on.
19. Precision Medicine

The second topic last year’s Elsevier’s blogpost discussed was the growth and rapid development of highly specific, targeted, individualized treatment plans. The mainstay example is of course how oncology treatments are moving away from one-size-fits-all chemotherapies to individualized mutation-specific immunomodulating therapy. (We’re moving like melting glaciers but moving nonetheless.) I was definitely well equipped with my ASCP online CE credits as I found myself discussing testing patients during my heme/onc training for PDL-1 and other tailored targets. We’re just starting to ride this wave and it’s definitely growing fast.
18. AI in healthcare (part 1)

Yep. I went there—it’s exciting! But notice I’ll come around after some other topics to really get into the heart of AI in path. Basically, the last point in the blogpost discussed the way smart software has been growing in medicine; particularly with radiology and surgery, using advancements in robotics and detection software to predict and stratify clinical information for patient care. Within this context let me quote them directly for you, “…there remains some uncertainty around the role of AI and its true impact on pathology, it is important to recognize that AI-based technologies or machines will never replace pathologists. Instead, such innovations will play an assistive role, augmenting the decision-making capabilities of pathologists and helping them perform better and faster…” All my pathologist friends may now exhale. It’s going to be okay. We’ll talk more about this at #10.
17. New Tech, New Toys
Pathologists are like the 007’s of the clinical team…at least when it comes to developing tech. There are so many new gadgets and tools we clinicians have available to us today. I delivered a recent TEDx talk where I discussed the “unrecognizable future” of medicine—and obviously now look for new and exciting ways to tell people I gave a TEDx talk. The important thing is that 73 days of doubling medical knowledge is happening so fast we don’t even know what we have available to us! Finger-print drug tests, smartphone facial capillary blood pressures, liquid biopsies, virtual MS-based immunohistochemical stains that never actually stain a single cell, cytology AI, deep data mining of free text pathology reports…it’s not a short list. It’s exciting, and we should all be sharing and collaborating to use these exciting tools together in creative ways for positive outcomes!
16. No More Silos
Last year, I wrote a few pieces here on Lablogatory that mentioned High-Reliability Organizations (HROs) which require absolutely full sharing of responsibility as well as knowledge in order to solve problems and improve patient-care outcomes. There are many ways siloed thinking can harm the progress of any institution. It takes leadership, creative problem-solving, transparency, and teamwork. In the coming months of 2020, keep an eye out for pockets within your organizational environment that act as black holes or veils to keep pieces of critical data from the rest of the team. Encourage discussions between you and your peers, check biases about what you think might be important for one team vs. another, and try to share successes and failures as a group.
15. New Types of Colleagues

What I just mentioned about engaging in new conversations with folks you might not have worked with before—its not groundbreaking, its just good practice! In order to tear down #16’s silos, we’ve got to seek out and explore new ways to collaborate with colleagues outside our everyday scope. There will always be discussions about generational divides and differences that create culture strife in the workplace, or political/opinionated schisms that divide even the most cohesive of medical specialties. (I’m looking at you ACOG, ACP, ASCCP, and others: it’s Cervical Cancer Awareness Month, can we just agree on some guidelines already…) Soapbox over. But seriously, this isn’t a new concept. Feel like a lab half filled with boomers and millennials can’t make the cut? Well, the Harvard Business Review gave us great recommendations for this exact type of interpersonal growth exercise—in the NINETIES! The take home message: having an open culture and proactive leadership allows for fruitful exchange and growth!
14. Digital Pathology!

It’s coming. You can’t stop it. It’s exciting. I don’t care what you think. Well I actually do care, but don’t knock digi-path till it grows into whatever it’s going to become. The desk of the (anatomic) pathologist-of-the-future will look a lot different from today and that’s really cool. Once upon a time, a very long, long time ago—in the eighties maybe—radiologists still had films where we actually used radiation to change the exposure of images to be read over a light box. Classic scene, right? Doctor, the x-ray is ready! *THWIP* *CLICK* *BUZZ* and cue the contemplative stare on the wall light. Then, they went digital and get to hang out in the dark with four computer screens and coffee, and really comfy chairs. I mean what a form of progress, can’t deny.
13. MS Methodologies

In my mailbox this month, is another excellent edition of The Pathologist and in it there’s a great article on Mass Spec imaging transitioning from a research tool to a clinical one. Woah. We’ve all talked about and praised MALDI-Tof methods for microbiologic assays and detection, but the expanse of mass spectrometry has developed rather quickly. Now, it’s looking for a niche in routine laboratory diagnostics outside of the old chemistry analyzer… It’s a new, non-destructive way of examining tissue and gleaning data from the smallest pieces of gross specimens. We’re onto something here, keep an eye on MSI.
12. Molecular—Need I say More?
Same edition of The Pathologist, about 25 pages back: a discussion on the value of molecular Next Generation Sequencing. I’ve already bored half of you, wait! Come back. I agree with you, you can only call it Next-Gen so many times before a whole generation of laboratorians get bored of talking about new tumor markers or mutations. But what’s happening with NGS testing that you should know? Simply put, there are NGS analyzers that are faster, with smaller footprints, combined with smarter software that is making molecular more feasible for laboratories that used to shy away from the notion of including NGS or LDTs in their lab testing menus. This means more labs, running more molecular, for more specific populations, in real time that can collaborate with that many more new colleagues while breaking silos—well just look up at #18, 17, 16, and 15!
11. Global Health

Dr. Dana Razzano recently interviewed me for her global health series, and we got the chance to talk about the important intersection of laboratory medicine and global public health. Getting involved in a community—especially for those of us in healthcare—often includes a survey of what kind of health challenges you face. For some it’s access to clean resources like water, for others it’s a complex system of reimbursement and billing issues that complicate delivery of care, or even more basic assessments reveal high rates of local infections with preventable illness. But you can’t tackle infrastructure change, political reform, or vaccine education single-handedly. Global health is an increasing part of our global world and, if we stay true to our professional values, we should be at the forefront.
10. AI in Healthcare (part 2)

Oh I told you I’d come back to this. Some folks are still apprehensive about AI—that’s ok—I am too, but only because I want to make sure it’s done right. Don’t expect any Skynet stuff, we’re not going that deep. So let me tell you some of the things I got to see on the residency interview trail that piqued my interests. At one hospital system, I saw plans for their anatomic pathology department to go fully digital with augmented AI software to help score mitoses and other morphologic traits by 2025. At another institution, I saw plans for data mining historical free text pathology reports to predict and stratify future specimens before they even got signed out! At a third system, I saw the utilization of smart software to predict clinical lab values for a patient’s personalized reference range…pre-analytically! This stuff is coming in hot so watch for it! What AI-related advancements are you seeing in your neck of the lab?
9. Patient Consultation

Another thing noteworthy of my residency trail are institutions which are championing the face-to-face consultative role of the clinical pathologist in patient care. We, at the end of the day, are consultants to all; physicians and patients alike. And many in our field are celebrating this role by pushing the envelope toward a progressive and effective future for pathology and laboratory medicine at large.
8. Graphic Medicine
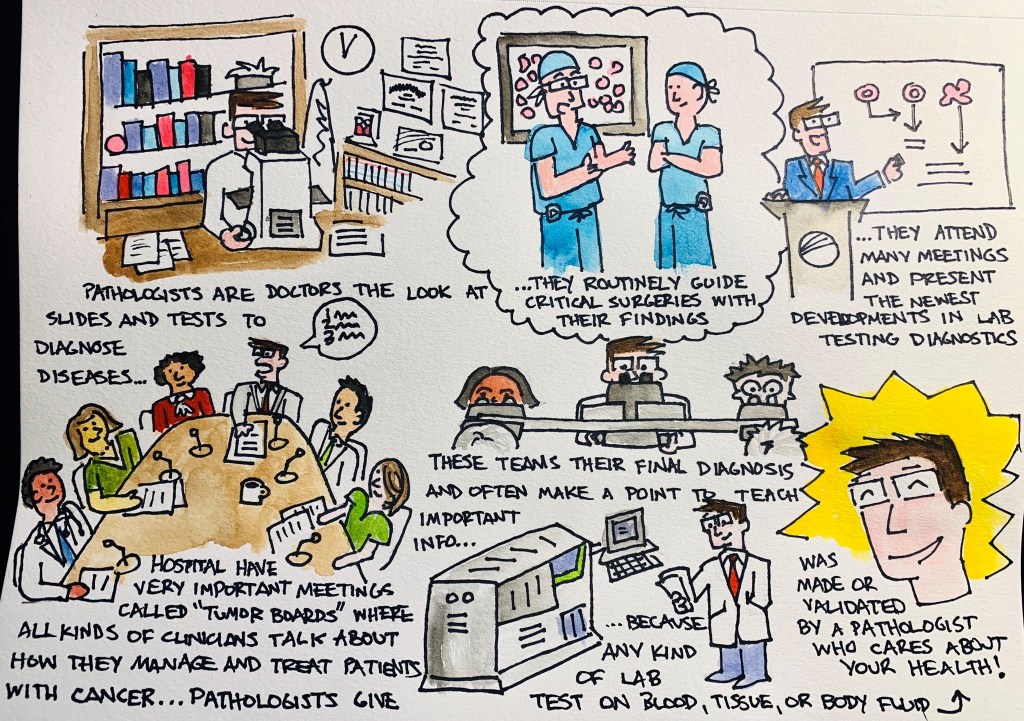
Graphic medicine is fantastic! I wish I could have discovered this years ago. Nevertheless, in the last two years I have sought out and read numerous pieces which bridge a significant gap between clinician and patient. And if we in laboratory medicine plan to reach patients more directly, we shouldn’t be afraid to come up with creative solutions to communicate with them. My (current) approach, #PathDoodles which I post occasionally on social media, attempts to explain concepts in pathology to the everyday lay person. What will you do to reach your patients?
7. Wellness Programs

Another interesting thing I encountered on the residency interview trail was the way in which different programs addressed the concept of wellness. Some did, some did not, but everyone discussed it. Because, after all, it is important; not just for residents and physicians, but medical lab scientists, support staff, and …yes… even administrators. Work and work-life stresses and balance take a psychological and emotional toll, and in order to be happy and healthy we need ways to strengthen our mental health along the way. Last year, Dr. Marissa Saint Martin won a 2018 award from the American Association for Physician Leadership for her work in preparing residency resilience and promoting wellness through structured curricula at Loyola Health System and Mount Sinai in Miami. She’s been featured with ASCP numerous times as well as in The Pathologist. It’s promising to see such strong support for residency trainees; keep an eye out for other praise-worthy programs this year!
6. Social Media
You caught me. I can’t make any predictions about the future of health care delivery, education, or collaboration without touting the importance of social media. As a member of the official ASCP Social Media Team (Go #ASCPSoMeTeam!), I’m a proud contributor not only to the content that we publish online, but to the message that unifies and spreads our #StrongerTogether mantra. Social media is fantastic tool to reach new colleagues, spread new ideas, and make new advancements in both our field and in reaching people where they are.
5. Moving Out of the Basement

One of the most memorable interviews I had this season was with a transfusion specialist who recounted to me his memory of training in pathology during his early days of residency. Green and eager, he told me how he remembered being taken on a tour of the facilities to be shown his desk/work space and upon reaching an underground level of the hospital building a sign read ‘BASEMENT’ with an adjacent one ‘PATHOLOGY’ …he paused to say it out loud, “What’s a basement-pathologist?” We bonded over the stifled stereotypes in our work and shared stories of great and terrible lab spaces we’ve seen. Some programs are renovating, some (for better) are moving on up… How are your facilities?
4. The Pipeline Problem

Well I mentioned stereotypes. I’ve talked about it before. You already know about shortages in pathology from physicians to lab scientists. And don’t get me started on pay—especially for lab workers and those in forensic path! But this is a topic I think we’re going to see a boon in media coverage in the coming years, starting now. Some of our awesome colleagues are talking about the “pipeline problem” from a myriad of angles: addressing medical student clerkships, exposure to laboratory workflow in school curriculum, advertising the infinite possibilities of careers within our profession…and more. CAP, ASCP, USCAP, and other professional societies have done amazing work in their due diligence to represent our field and advocate for the advancement of our work and image. A former CAP president once said, “Pathology is what a pathologist does,” and well, it’s a good start. Where do you see solutions to our pipeline problem?
3. PA’s and… CPA’s?

Now this, this is a cool concept and it’s the first time I’ve seen it. We all know and love our pathology assistants (PAs)—especially resident pathologists—as they make the training, education, and workload a better process for learning. They have awesome training and operate essentially as highly specialized clinicians in anatomic pathology. But what about the clinical, laboratory medicine side of things…? I recently saw a program advertised at the University of Alabama at Birmingham that trains clinical PAs for consultative and ancillary support roles to the clinical pathologist! Fantastic! Read more about it here! There are a growing number of DCLS (doctor of clinical laboratory science) professionals, now we’ve got a new pipeline to invite talented folks to work with us in a new way.
2. I’ll Have a Residency!

I have seen so many fantastic programs across the US these past few months, and so many decisions go into the way medical graduates rank programs to match into. To learn how the AAMC/NRMP matching system works, watch this video (maybe with some calming tea). We’ll see where I end up matching to, but I’m excited for the next chapter and to really dive into pathology even more!
1. You!
Obviously, the most important thing to keep an eye out for this year is you! Your goals, your ambition, your plans, your ideas and thoughts, and all the ways you contribute to our fantastic profession! I encourage you all to share, collaborate, and be creative with the ways in which we advance the future of laboratory medicine and continue to keep in mind that we do these things for our patients everywhere.
Thanks for reading, see you next time!

–Constantine E. Kanakis MD, MSc, MLS (ASCP)CM completed his BS at Loyola University Chicago and his MS at Rush University. He writes about experiences through medical school through the lens of a medical lab scientist with interests in hematopathology, molecular, bioethics, transfusion medicine, and graphic medicine. He is currently a 2020 AP/CP Residency Applicant and actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Follow him on Twitter @CEKanakisMD
