For more information, check out CDC’s page for laboratories.
Month: January 2020
Hyping Technology with Opinions rather than Facts
I often have an argument or discussion with my spouse about facts versus opinions. Although both concepts represent information, my brain is mostly concerned with facts as a scientist and a problem solver. My spouse, having spent years in the hospitality, banking, and real estate business, is “all about the customer,” with success rooted largely in recognition of and alignment to their opinions. In my current role as CMO at ASCP where we have “concierge customer service” as one of our principles, I have adapted to listening, understanding, and operationalizing the opinions of a diverse group of individuals. However, when it comes to science, I feel that it is important to remain with facts until the point where science runs out of answers, and we have to guess about something. Where I run into trouble is that I have the opinion that people who do not understand the facts should not necessarily espouse their opinions. Someone once said an expert is someone who knows everything about a topic as well as everything that is wrong about a topic—referring to common misunderstandings that flow through our common knowledge. Opinions are like belly buttons—everyone has one, but some are cleaner than others.
When it comes to journalism, I am unfortunately a purest. I just want the facts. I was, therefore, a bit taken aback by a New York Times article discussing an innovative technology in neurosurgery for intraoperative consultations for brain tumors. My visceral negative response emerged from the surgeon discussed in the article owning part of the company that built the device for the study. My secondary concerns stem from the article discussing intraoperative consultations done by pathologists and, yet, not a single pathologist was interviewed for the article. But the biggest concern I had which made me delve deeper into the topic was the enormous number of inaccurate facts or complete untruths presented in the article. It is hard to say it wasn’t poor journalism but, as a scientist, I had to go to the source.
The scientific article in question was “Near real-time intraoperative brain tumor diagnosis using stimulated Raman histology and deep neural networks” published on Jan 6, 2020. The New York Times article, “A.I. Comes to the Operating Room” was published the same day. I read the article myself, and when it didn’t quite pass my sniff test, asked three of my colleagues who are experts in this area to also read the paper and the news report. Jane Brock, a breast pathologist who is truly an innovative thinker and dreams of the day when pathologists can study tissue immediately with confocal laser imaging and rapid molecular testing—part of her research—said of the technology, “this is a great paper and a great microscope.” She further mentioned how brain is ideal because it is homogenous, easily flattened, and amenable to artificial intelligence (AI) review because of the limited parameters needed to be evaluated for clinical decision making intraoperatively. “This is definitely the future of pathology—getting rid of frozen sections in favor of fresh tissue imaging,” Dr. Brock said. “It also means you can take tissue for research/molecular diagnostics, image it, and not waste it just by imagining it [on frozen section]. The time savings are huge.” It was exciting to hear Dr. Brock’s enthusiasm for the technology conceptually and how it could be a boon for pathologists’ ability to consult during surgery.
Dr. Rebecca Folkerth, a surgical neuropathologist for more than 20 years before she became the neuropathologist for the Office of the Medical Examiner of New York, had some concerns about the science in the paper and the maturity of the technology to replace a consultation with a pathologist today. “The questions asked [in the paper] were of necessity extremely basic, and hardly represent the real world as encountered in the operating room and neuropathology laboratory,” said Dr. Folkerth. She was concerned in the news article with the statement “Final pathologic diagnosis is increasingly driven by molecular rather than morphologic criteria.” “That is actually true for a minority of nervous system lesions, such that the ‘gold standard’ for diagnosis remains ‘macroscopic (gross) pathology’ [essentially imaging] and ‘cytologic and histoarchitectural features’ as well as clinical and laboratory findings. In other words,” concluded Dr. Folkerth, “the training and experience of a physician [pathologist] is what allows the synthesis of all data points to arrive at a comprehensive interpretation.” With regard to the immediate application to real world practice, Dr. Folkerth said, “It is telling that no ‘gliosis/treatment effect’ cases were analyzed [because] distinction of post-treatment changes from a neoplastic process in the brain is one of the most difficult encountered in clinical neuropathology.” Other cellular processes that occur in the brain were also not in the study. “A glaring omission of this paper,” Dr. Folkerth concluded, “were the consequences of the errors in ‘predicting diagnosis’. Were these ‘class A’ [leading to radical changes]?” In the article, the surgeon states that neuropathologists “hate frozen sections” which Dr. Folkerth says is simply not true. Perhaps the author should have interviewed an actual neuropathologist for this piece. Both Dr. Brock and Dr. Folkerth had concerns about the practicality of the technology where Dr. Brock felt it was currently “too expensive” (relative to current practice which provides more information across the spectrum of neuropathology) while Dr Folkerth was not clear who this process could work in smaller or decentralizes or underserved surgical settings (as the new article suggests) without a lower cost. Dr. Folkerth agreed with Dr. Brock, however, that this technology “may well represent a revolution in intraoperative decision-making and outcome.”
Lastly, I spoke with Dr. Jason Hornick, who in addition to be an internationally renowned surgical pathologist, has been in charge of quality of intraoperative consultations at one of the premiere hospitals in the US. The “frozen section [procedure] does not often take longer than 30 minutes, and is not often ‘far less accurate’ than in the study,” Dr. Hornick began. “The rates of significant discordance between intraoperative diagnosis and the final diagnosis in published surveys (for all of surgical pathology) are generally less that 1.5%.” Dr. Hornick (and I) agree that the surgeon quoted in the article is bashing the practice of pathology without any accuracy to his statements. He is not quoting facts and he is not quoting opinions. He is simply saying things that are wrong and not supported by data or years of experience. Dr. Hornick also mentioned that the cost of frozen sections are trivial compared with the cost of this technology and, as pointed out by Dr. Folkerth, the pathologists’ intraoperative consultation is much broader than just reviewing a slide for signs of tumor. Dr. Hornick said it best: “The expert consultation provided intraoperatively by the pathologist to the surgeon is not restricted to making an accurate diagnosis; pathologists are uniquely suited to integrating the patient’s clinical history, imaging, prior pathology, and surgical findings to assist the surgeon in making surgical decisions.” He concluded, “The intraoperative consultation is not a laboratory test; it is a consultative opinion by an expert physician who often understands the patient’s disease better than the surgeon.”
With these three experts’ views including their clarification of the facts and their opinions, it seems pretty clear, in my opinion, that this news article is presenting an inappropriate picture of the practice of pathology and making claims about this technology which are not, in fact, accurate or fair. What struck me, however, was the comment by the surgeon that when he was working with pathologists, he may only ask two questions because of the very long time for the frozen section but with this technology he can ask six or seven questions and get the answers really quickly. If this surgeon needed to know the answers to those question, that is, if they were mission critical to patient care, why didn’t the surgeon work with the pathology team and demand higher quality and faster turnaround time rather than investing time and money in a novel, expensive technology (from which he profits) which can only provide a fraction of the answers that a pathologist can provide? Unless the technology completely replaces a pathologist—which it doesn’t seem to be able to do—the pathologists and frozen section labs still have to be available. Thus, costs are increased, not decreased. The only parameter for increased value for the patient would appear to be time savings; however, most clinicians and pathologists would agree that the value to a patient of a two-minute AI read versus less than 20-minute intraoperative consultation is minimal compared with the cost difference.
But outside of all of this, as the entire field of pathology faces pressure from technologies—largely driven by non-pathologists—we have to realize that pathologists’ consultations, whether intraoperative or on permanents, are a tool of quality directly for the patient. If a surgeon is able to perform a surgery and discard tissue, use a system from which he/she profits, or depends solely on a computer algorithm informed by a couple of hundred cases, where is the quality check for the patient? How do we know that was tumor that was removed? Pathologists are paid to perform intraoperative consultations and ASCP works very hard to ensure that pathologists are not only fairly paid for their work but that their involvement occurs whenever it can improve quality and care for the patient. Dr. Folkerth alone has seen thousands of cases on intraoperative consultation for neuropathology and the collective knowledge of currently living neuropathologists would be millions of cases. If such knowledge were captured by an AI across the full spectrum of neuropathology, the technology would truly be remarkable. But you can’t have such integration of knowledge without involving pathologists.

-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
Prozone Effect in the Fecal Immunochemical Test (FIT)
Case History
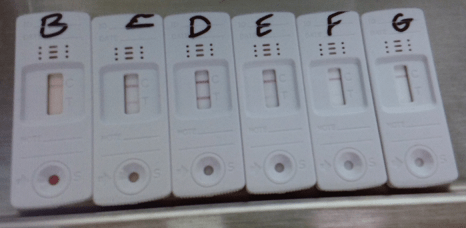
An 80 year old female had a history of chronic iron deficiency anemia with unknown cause and comorbidities included hypothyroidism, congestive heart failure (CHF), severe aortic stenosis and COPD. The patient presented at the ED with initial presentation with increasing shortness of breast, NYHA class 3-4. She was admitted to the hospital for further treatment for CHF, as well hyperventilation, sleep apnea and COPD. Her serum iron and iron saturation were tested and results were 2 umol/L (reference range for iron: 10-29 umol/L) and 7% (reference range: 14-51%), respectively. Part of her investigations included a qualitative fecal test to screen for gastrointestinal bleeding. The immunochemical fecal occult blood test was performed using a CLIA waived Hema Screen SpecificTM POCT test (Immunostics, Inc, USA) in the hospital lab. Hema Screen Specific test is a qualitative, sandwich dye conjugated immunoassay that uses a combination of monoclonal and polyclonal antibodies to detect the globin component of hemoglobin in the fecal samples. The manufacture recommended using Hema Screen Specific test in routine physical examines, hospital monitoring of bleeding in patients and for screening for colorectal cancer or gastrointestinal bleeding for any source (statement from the product package insert).
The specimen submitted to the lab was markedly red (Image 1), yet Hema screen test returned a negative result. Since this device is designed to detect occult blood in fecal samples, a prozone effect was suspected, as the stool appeared to contain overt hemorrhage. The specimen was reanalyzed with serial dilutions by a factor of 5, 10, and at 100 × dilution. The FIT result became clearly positive for blood (Image 2). The patient received a colonoscopy, which revealed internal hemorrhoids, severe diverticulosis in the left colon, as well as multiple angiodysplastic lesions. One such lesion was in the ascending colon and was actively bleeding at the time of colonoscopy. The others, which were not bleeding, were distributed in the proximal ascending colon, hepatic flexure, and proximal transverse colon. All angiodysplastic lesions were treated with argon plasma coagulation.


Moreover, we have tested the device with another bloody fecal sample during the initial evaluation. When an appropriate dilution factor was used, the prozone effect begins to lose its interference as show in Image 3.
Discussion
The prozone effect (or Hook effect) has long been appreciated as a source of interference in immunoassays.1 It typically occurs in sandwich assays, of which the FIT test is an example.2 When the concentration of the analyte is excessively high, it oversaturates the capture and detection antibodies in favor of forming single antibody:analyte complexes, rather than sandwiches. This results in a false negative result where the assay is unable to detect the analyte. The solution to the prozone effect is serial dilution to lower the concentration of the analyte.
The FIT test is designed to detect microscopic amounts of blood, hence its function in screening for fecal occult blood. A number of hospital labs use this test in an acute care setting to screening bleeding in patients. However, its capacity is oversaturated in specimens containing overt hemorrhage, as in our patient. In these cases it is nevertheless important to prove that the red color of the specimen is truly due to blood, as bright red stool can be caused by a wide range of dietary factors. Some examples are red food coloring, beets, cranberries, and tomato juice.3 If these possibilities are not ruled out, the patient may become subject to the risks of unnecessary endoscopy. Serial dilution of the specimen is extremely useful in this type of situation.
References
- Dasgupta A, Wahed A. Clinical Chemistry, Immunology and Laboratory Quality Control: A Comprehensive Review for Board Preparation, Certification and Clinical Practice. Amsterdam: Elsevier; 2014. 2.11.
- Allison JE, Fraser CG, Halloran SP, Young GP. Population Screening for Colorectal Cancer Means Getting FIT: The Past, Present, and Future of Colorectal Cancer Screening Using the Fecal Immunochemical Test for Hemoglobin (FIT). Gut and Liver. 2014 Mar;8(2):117-30. https://doi.org/10.5009/gnl.2014.8.2.117
- Picco MF. Stool color: When to worry [Internet]. Mayo Clinic; 2019 Feb 19 [cited 2019 Feb 23]. Available from: https://www.mayoclinic.org/stool-color/expert-answers/faq-20058080

-Hao Li, MD is a currently a first year anatomical pathological resident at Western University, London ON, Canada. Prior to be a pathology resident, he was a neurosurgery resident at the University of Saskatchewan, Saskatoon SK, Canada. When he was at the University of Saskatchewan, he spent his third year primarily in neuropathology, with also some general anatomical pathology and clinical pathology. Through these experiences, he has come to realize that his passion and calling lay more in pathology than in surgery. He has successfully transferred into pathology, and started a new residency in anatomical pathology in July 2019. Having a background in the clinical neurosciences, he hopes to eventually pursue a fellowship in neuropathology, and possess the skill set to practice both anatomical pathology and neuropathology.
Transfusion Medicine Case Study: Positive Pretransfusion Test
A 72 year old man was admitted to the hospital for an aneurysm repair. The physician ordered a type and crossmatch for 6 units of blood in preparation for surgery. The patient history included surgery in 2016 during which he was transfused with 4 units of RBCs.
patient’s blood type: A positive
antibody screen: negative
history: anti Jkb (2016)
6 Jkb negative units were found and full crossmatches were performed. One of the 6 donor units was incompatible. What is the most probable explanation for these findings?
If the patient has a negative antibody screen, and no history of an antibody, most facilities would do an electronic crossmatch or an immediate spin crossmatch. The immediate spin (abbreviated) crossmatch will simply verify ABO compatibility. However, if the patient has a positive antibody screen, we must identify the antibody, phenotype the patient, and do a full AHG crossmatch with donor units that are antigen negative for the corresponding antibody. In this case, the patient had a history of an antibody, so the antibody must be honored, and antigen negative units must be chosen for transfusion.
Kidd antibodies demonstrate dosage, are often weak, and can be found in combination with other antibodies. Because if this, they can be notoriously difficult to detect. They are usually IgG and are made in response to transfusion or pregnancy. Jkb has an antigen frequency of about 73% in the white population and about 43% in the black population. To find antigen negative blood, we consider that about 27% of units would be antigen negative. The tech working on the sample screened 21 units and found 6 that were Jkb negative.
AHG crossmatch results:
unit 1: compatible
unit 2: compatible
unit 3: compatible
unit 4: 3+ at AHG
unit 5: compatible
unit 6: compatible
There are 2 possible scenarios for the above results. A crossmatch is a test between donor’s red blood cells and patient’s plasma. Antigens, we know, are on red blood cells and antibodies are detected in the plasma. So, with a negative antibody screen, crossmatch incompatibility is due either to a patient antibody to a low incidence antigen on the donor red blood cells, or a donor cells with a positive direct antiglobulin test. We can easily rule in or out a positive donor DAT by performing a DAT on the segment. If the donor unit has a positive DAT, the unit should be quarantined and the positive DAT reported to the collecting facility. If the donor unit has a negative DAT, the patient likely has an antibody to a low incidence antigen.
Low frequency antigens are uncommon, but antibodies that recognize them are less rare. Fortunately, for patients with these antibodies to low frequency antigens, finding antigen negative compatible blood is easy. As we can see, 5 of the 6 chosen units were negative for the unknown low frequency antigen and were antiglobulin crossmatch compatible. The low prevalence of the antigen makes compatible blood readily available. If transfusion is necessary, it should not be delayed while waiting for identification of the antibody.
In this case, the antibody screen was repeated and the negative result was verified. In many cases, it may not be possible for a lab to identify the antibody because the lab may not have the necessary panel cells or typing reagents. Yet, these antibodies to low incidence antigens that react at AHG can be clinically significant and cause severe hemolytic transfusion reactions. To identify the antibody, you may need to send the sample to a reference lab for testing against a panel of reagent red cells that express low incidence antigens. Alternately, the donor red cells that were incompatible can be tested against known antibodies to low prevalence antigens to help identify the antibody.
In this patient, anti-Wra was identified. The incompatible donor unit was verified to be Wra positive. Wra is part of the Diego system, usually IgG, and has ben implicated in hemolytic transfusion reactions.
One of the reasons I have written up this case is questions my Transfusion Medicine students often ask about exam and exam prep questions concerning incompatibility. Below are 2 questions to give examples of the confusion.
“At the indirect antiglobulin phase of testing, there is no agglutination between patient serum and screening cells. One of 3 donor units was incompatible.. The most probable explanation for these findings is that the:
- patient has an antibody directed against a high incidence antigen
- patient has an antibody directed against a low incidence antigen
- donor has an antibody directed against donor cells
- donor has a positive antibody screen”5
answer: b
“Which of the following would most likely be responsible for an incompatible antiglobulin crossmatch?
- recipient’s red cells possess a low incidence antigen
- anti-K antibody in donor serum
- recipient’s red cells are polyagglutinable
- donor red cells have a positive direct antiglobulin test”4
answer: d
I am asked why is one answer “low prevalence antigen” and one answer “positive DAT”? I typically ask questions of my students to let them reason out the answer. Take a careful look at the words antigen and antibody. Remember that a DAT is a test of red cells, the IAT tests for antibodies in plasma. A crossmatch uses donor red cells against patient plasma. Therefore, even though these are both reasons for the incompatibility of one out of multiple units, each question only has one answer of a common reason for such incompatibility. Be sure to read questions and use your theory and knowledge of testing when encountering discrepancies and problems in Blood Bank. To all of my students: Happy Studying for your ASCP exam!
References
- Fung, Mark K., Technical Manual 18th ed, Bethesda: AABB, 2014.
- Harmening, Denise M. Modern Blood Banking and Transfusion Practices, 7th edition, 2019.
- Schonewille, Henk, et al. “The importance of antibodies against low‐incidence RBC antigens in complete and abbreviated cross‐matching”. The Journal of AABB. 20 June 2003.
- BOC Study Guide, 5th edition. Clinical Laboratory Certification Examinations. ASCP, 2016
- BOC Study Guide, 6th edition. Clinical Laboratory Certification Examinations. ASCP, 2018

-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
2020 Vision
Welcome back everybody! Thank you for all the engagement on my last post, Up In Smoke¸ where I discussed the plenary publications surrounding the vaping crisis and EVALI as new pulmonary pathology entity. This month, let’s start 2020 off right. After the holiday break and going on some of my last pathology residency interviews, I’d like to reflect on this new year by taking a look at 20 exciting things on the horizon for those of us in pathology and laboratory medicine!
So, let’s take a look at 2020 with some 20/20 vision… (sorry, not sorry)
20. Big, big, big, big data

Last year, Elsevier’s Clinical Solutions Director in China discussed three topics that would impact our profession in 2019—so let’s start there. These first three go hand-in-hand in prepping the stage for 2020. Up first: the never-ending explosion of biomedical information and the continuing tidal wave of health data we don’t even know what to do with just yet! It’s a very interesting estimate that, by 2020 (aka now!) the whole sum of medical knowledge will double every 73 days. How on earth are we to manage, when compared to 1950 it would have taken 50 years to double? Well, the argument in the linked Elsevier blogpost discusses how evidence-based inquiry databases will store and organize this knowledge for us: think UpToDate, or ExpertPath, or ImmunoQuery…some of you are nodding your heads in relief, great, I’ll move on.
19. Precision Medicine

The second topic last year’s Elsevier’s blogpost discussed was the growth and rapid development of highly specific, targeted, individualized treatment plans. The mainstay example is of course how oncology treatments are moving away from one-size-fits-all chemotherapies to individualized mutation-specific immunomodulating therapy. (We’re moving like melting glaciers but moving nonetheless.) I was definitely well equipped with my ASCP online CE credits as I found myself discussing testing patients during my heme/onc training for PDL-1 and other tailored targets. We’re just starting to ride this wave and it’s definitely growing fast.
18. AI in healthcare (part 1)

Yep. I went there—it’s exciting! But notice I’ll come around after some other topics to really get into the heart of AI in path. Basically, the last point in the blogpost discussed the way smart software has been growing in medicine; particularly with radiology and surgery, using advancements in robotics and detection software to predict and stratify clinical information for patient care. Within this context let me quote them directly for you, “…there remains some uncertainty around the role of AI and its true impact on pathology, it is important to recognize that AI-based technologies or machines will never replace pathologists. Instead, such innovations will play an assistive role, augmenting the decision-making capabilities of pathologists and helping them perform better and faster…” All my pathologist friends may now exhale. It’s going to be okay. We’ll talk more about this at #10.
17. New Tech, New Toys
Pathologists are like the 007’s of the clinical team…at least when it comes to developing tech. There are so many new gadgets and tools we clinicians have available to us today. I delivered a recent TEDx talk where I discussed the “unrecognizable future” of medicine—and obviously now look for new and exciting ways to tell people I gave a TEDx talk. The important thing is that 73 days of doubling medical knowledge is happening so fast we don’t even know what we have available to us! Finger-print drug tests, smartphone facial capillary blood pressures, liquid biopsies, virtual MS-based immunohistochemical stains that never actually stain a single cell, cytology AI, deep data mining of free text pathology reports…it’s not a short list. It’s exciting, and we should all be sharing and collaborating to use these exciting tools together in creative ways for positive outcomes!
16. No More Silos
Last year, I wrote a few pieces here on Lablogatory that mentioned High-Reliability Organizations (HROs) which require absolutely full sharing of responsibility as well as knowledge in order to solve problems and improve patient-care outcomes. There are many ways siloed thinking can harm the progress of any institution. It takes leadership, creative problem-solving, transparency, and teamwork. In the coming months of 2020, keep an eye out for pockets within your organizational environment that act as black holes or veils to keep pieces of critical data from the rest of the team. Encourage discussions between you and your peers, check biases about what you think might be important for one team vs. another, and try to share successes and failures as a group.
15. New Types of Colleagues

What I just mentioned about engaging in new conversations with folks you might not have worked with before—its not groundbreaking, its just good practice! In order to tear down #16’s silos, we’ve got to seek out and explore new ways to collaborate with colleagues outside our everyday scope. There will always be discussions about generational divides and differences that create culture strife in the workplace, or political/opinionated schisms that divide even the most cohesive of medical specialties. (I’m looking at you ACOG, ACP, ASCCP, and others: it’s Cervical Cancer Awareness Month, can we just agree on some guidelines already…) Soapbox over. But seriously, this isn’t a new concept. Feel like a lab half filled with boomers and millennials can’t make the cut? Well, the Harvard Business Review gave us great recommendations for this exact type of interpersonal growth exercise—in the NINETIES! The take home message: having an open culture and proactive leadership allows for fruitful exchange and growth!
14. Digital Pathology!

It’s coming. You can’t stop it. It’s exciting. I don’t care what you think. Well I actually do care, but don’t knock digi-path till it grows into whatever it’s going to become. The desk of the (anatomic) pathologist-of-the-future will look a lot different from today and that’s really cool. Once upon a time, a very long, long time ago—in the eighties maybe—radiologists still had films where we actually used radiation to change the exposure of images to be read over a light box. Classic scene, right? Doctor, the x-ray is ready! *THWIP* *CLICK* *BUZZ* and cue the contemplative stare on the wall light. Then, they went digital and get to hang out in the dark with four computer screens and coffee, and really comfy chairs. I mean what a form of progress, can’t deny.
13. MS Methodologies

In my mailbox this month, is another excellent edition of The Pathologist and in it there’s a great article on Mass Spec imaging transitioning from a research tool to a clinical one. Woah. We’ve all talked about and praised MALDI-Tof methods for microbiologic assays and detection, but the expanse of mass spectrometry has developed rather quickly. Now, it’s looking for a niche in routine laboratory diagnostics outside of the old chemistry analyzer… It’s a new, non-destructive way of examining tissue and gleaning data from the smallest pieces of gross specimens. We’re onto something here, keep an eye on MSI.
12. Molecular—Need I say More?
Same edition of The Pathologist, about 25 pages back: a discussion on the value of molecular Next Generation Sequencing. I’ve already bored half of you, wait! Come back. I agree with you, you can only call it Next-Gen so many times before a whole generation of laboratorians get bored of talking about new tumor markers or mutations. But what’s happening with NGS testing that you should know? Simply put, there are NGS analyzers that are faster, with smaller footprints, combined with smarter software that is making molecular more feasible for laboratories that used to shy away from the notion of including NGS or LDTs in their lab testing menus. This means more labs, running more molecular, for more specific populations, in real time that can collaborate with that many more new colleagues while breaking silos—well just look up at #18, 17, 16, and 15!
11. Global Health

Dr. Dana Razzano recently interviewed me for her global health series, and we got the chance to talk about the important intersection of laboratory medicine and global public health. Getting involved in a community—especially for those of us in healthcare—often includes a survey of what kind of health challenges you face. For some it’s access to clean resources like water, for others it’s a complex system of reimbursement and billing issues that complicate delivery of care, or even more basic assessments reveal high rates of local infections with preventable illness. But you can’t tackle infrastructure change, political reform, or vaccine education single-handedly. Global health is an increasing part of our global world and, if we stay true to our professional values, we should be at the forefront.
10. AI in Healthcare (part 2)

Oh I told you I’d come back to this. Some folks are still apprehensive about AI—that’s ok—I am too, but only because I want to make sure it’s done right. Don’t expect any Skynet stuff, we’re not going that deep. So let me tell you some of the things I got to see on the residency interview trail that piqued my interests. At one hospital system, I saw plans for their anatomic pathology department to go fully digital with augmented AI software to help score mitoses and other morphologic traits by 2025. At another institution, I saw plans for data mining historical free text pathology reports to predict and stratify future specimens before they even got signed out! At a third system, I saw the utilization of smart software to predict clinical lab values for a patient’s personalized reference range…pre-analytically! This stuff is coming in hot so watch for it! What AI-related advancements are you seeing in your neck of the lab?
9. Patient Consultation

Another thing noteworthy of my residency trail are institutions which are championing the face-to-face consultative role of the clinical pathologist in patient care. We, at the end of the day, are consultants to all; physicians and patients alike. And many in our field are celebrating this role by pushing the envelope toward a progressive and effective future for pathology and laboratory medicine at large.
8. Graphic Medicine
Graphic medicine is fantastic! I wish I could have discovered this years ago. Nevertheless, in the last two years I have sought out and read numerous pieces which bridge a significant gap between clinician and patient. And if we in laboratory medicine plan to reach patients more directly, we shouldn’t be afraid to come up with creative solutions to communicate with them. My (current) approach, #PathDoodles which I post occasionally on social media, attempts to explain concepts in pathology to the everyday lay person. What will you do to reach your patients?
7. Wellness Programs

Another interesting thing I encountered on the residency interview trail was the way in which different programs addressed the concept of wellness. Some did, some did not, but everyone discussed it. Because, after all, it is important; not just for residents and physicians, but medical lab scientists, support staff, and …yes… even administrators. Work and work-life stresses and balance take a psychological and emotional toll, and in order to be happy and healthy we need ways to strengthen our mental health along the way. Last year, Dr. Marissa Saint Martin won a 2018 award from the American Association for Physician Leadership for her work in preparing residency resilience and promoting wellness through structured curricula at Loyola Health System and Mount Sinai in Miami. She’s been featured with ASCP numerous times as well as in The Pathologist. It’s promising to see such strong support for residency trainees; keep an eye out for other praise-worthy programs this year!
6. Social Media
You caught me. I can’t make any predictions about the future of health care delivery, education, or collaboration without touting the importance of social media. As a member of the official ASCP Social Media Team (Go #ASCPSoMeTeam!), I’m a proud contributor not only to the content that we publish online, but to the message that unifies and spreads our #StrongerTogether mantra. Social media is fantastic tool to reach new colleagues, spread new ideas, and make new advancements in both our field and in reaching people where they are.
5. Moving Out of the Basement

One of the most memorable interviews I had this season was with a transfusion specialist who recounted to me his memory of training in pathology during his early days of residency. Green and eager, he told me how he remembered being taken on a tour of the facilities to be shown his desk/work space and upon reaching an underground level of the hospital building a sign read ‘BASEMENT’ with an adjacent one ‘PATHOLOGY’ …he paused to say it out loud, “What’s a basement-pathologist?” We bonded over the stifled stereotypes in our work and shared stories of great and terrible lab spaces we’ve seen. Some programs are renovating, some (for better) are moving on up… How are your facilities?
4. The Pipeline Problem

Well I mentioned stereotypes. I’ve talked about it before. You already know about shortages in pathology from physicians to lab scientists. And don’t get me started on pay—especially for lab workers and those in forensic path! But this is a topic I think we’re going to see a boon in media coverage in the coming years, starting now. Some of our awesome colleagues are talking about the “pipeline problem” from a myriad of angles: addressing medical student clerkships, exposure to laboratory workflow in school curriculum, advertising the infinite possibilities of careers within our profession…and more. CAP, ASCP, USCAP, and other professional societies have done amazing work in their due diligence to represent our field and advocate for the advancement of our work and image. A former CAP president once said, “Pathology is what a pathologist does,” and well, it’s a good start. Where do you see solutions to our pipeline problem?
3. PA’s and… CPA’s?

Now this, this is a cool concept and it’s the first time I’ve seen it. We all know and love our pathology assistants (PAs)—especially resident pathologists—as they make the training, education, and workload a better process for learning. They have awesome training and operate essentially as highly specialized clinicians in anatomic pathology. But what about the clinical, laboratory medicine side of things…? I recently saw a program advertised at the University of Alabama at Birmingham that trains clinical PAs for consultative and ancillary support roles to the clinical pathologist! Fantastic! Read more about it here! There are a growing number of DCLS (doctor of clinical laboratory science) professionals, now we’ve got a new pipeline to invite talented folks to work with us in a new way.
2. I’ll Have a Residency!

I have seen so many fantastic programs across the US these past few months, and so many decisions go into the way medical graduates rank programs to match into. To learn how the AAMC/NRMP matching system works, watch this video (maybe with some calming tea). We’ll see where I end up matching to, but I’m excited for the next chapter and to really dive into pathology even more!
1. You!
Obviously, the most important thing to keep an eye out for this year is you! Your goals, your ambition, your plans, your ideas and thoughts, and all the ways you contribute to our fantastic profession! I encourage you all to share, collaborate, and be creative with the ways in which we advance the future of laboratory medicine and continue to keep in mind that we do these things for our patients everywhere.
Thanks for reading, see you next time!

–Constantine E. Kanakis MD, MSc, MLS (ASCP)CM completed his BS at Loyola University Chicago and his MS at Rush University. He writes about experiences through medical school through the lens of a medical lab scientist with interests in hematopathology, molecular, bioethics, transfusion medicine, and graphic medicine. He is currently a 2020 AP/CP Residency Applicant and actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Follow him on Twitter @CEKanakisMD
Biomarker Testing for Cancer Patients: Barriers and Solutions, Part 2
As you may recall last month I shared common barriers to biomarker testing for cancer patients in the community. I also began to dive-in to a few solutions that I have seen implemented to overcome the barriers. Last month I shared solutions that may help with high cost and long turnaround times for biomarker testing. This month I would like to discuss issues with tissue including quantity.
Here are the top 10 barriers that I’ve seen to biomarker testing in the community:
- High cost of testing.
- Long turnaround time for results.
- Limited tissue quantity.
- Preanalytical issues with tissue.
- Low biomarker testing rates.
- Lack of standardization in biomarker testing.
- Siloed disciplines.
- Low reimbursement.
- Lengthy complex reports.
- Lack of education on guidelines.
Sample quantity and quality are both important when considering biomarker testing. If we don’t have enough material we cannot perform the test (quantity not sufficient or QNS). If we have poor quality we cannot trust the results. The old adage of garbage in garbage out holds true for biomarker testing just as it does for all other lab tests.
I’ll start with sample quantity this month and cover quality issues next month. The issue here is that a variety of biopsy types are performed on patients depending on the location and size of a suspicious mass. Historically we only needed enough material for the pathologist to make a diagnosis. Now we often need enough material for diagnosis and biomarker testing. Some tumor types such as breast and ovarian cancers produce enough material in locations that are easily accessible that tissue quantity is rarely an issue, however other tumor types such as lung and pancreatic cancers there is often an issue with tissue quantity. These tumor types must be handled with care to ensure no tissue recovered is lost.
The first step in addressing tissue insufficiency is knowing where you are starting. Do you have an issue with quantity not sufficient (QNS) rate? If you don’t know how many of your cases are insufficient for biomarker testing, then you can’t determine if you have an issue. If your testing is performed at a reference laboratory, you can request your QNS rate from the lab. They may also be able to provide you with the national QNS rate and then you could benchmark yourself against your peers. It is important to have an accurate QNS rate, so if there are blocks that are not sent to the reference lab because the pathologist has determined the block to be exhausted (no tissue is left) then the QNS rate provided by the reference lab may be artificially low.
It is important to agree upon what is QNS. We consider a specimen to be QNS if we cannot perform biomarker testing on the block. Others may consider the block QNS only if there wasn’t sufficient material for diagnosis. We have to ensure there is enough tumor content in the tissue to proceed with biomarker testing, in our case 10% of the nucleated cells (not volume) must be tumor (determined by pathology review of an H&E slide). If we have enough tumor, we can still end up with a QNS block due to low DNA and RNA yield. So we need sufficient tumor and sufficient tissue.
Here is a brief overview of solutions I have seen work to address limited tissue that can lead to high QNS rates:
- Education. The person collecting the biopsy needs to understand how much material is needed. Remember we have moved the goal post. Sufficient material for diagnosis was enough in the past, now we need more material to perform biomarker testing. Educating the team on why we need more material is valuable in ensuring sufficient material is collected.
- ROSE. Rapid onsite evaluation (ROSE) by a pathologist in the procedure room to determine sufficiency has been shown to decrease the repeat biopsy rate [1]. The pathologist can ensure the biopsy is being collected in a tumor rich region and help ensure areas of necrosis are avoided.
- Embedding cores separately. We often get core needle biopsies on lung cancer specimens. We prefer 3-5 cores. It is best practice to independently embed the cores in separate blocks. I have also seen labs that embed no more than 2 cores in one block. This would allow one block to be conserved for diagnosis and the other to be used for biomarker testing.
- Visual cue for limited tissue. Someone far more creative than me developed a process in histology where in cases of limited tissue the tissue was embedded in a red cassette. This cassette color was a visual cue for everyone handling the block that the tissue was limited and care should be taken when facing into the block. This has evolved over time to a red bead being embedded beside the tissue. Any visual cue and an associated procedure to ensure tissue conservation can help ensure we are conserving tissue in cases where it matters.
- Limited IHC Stains. The primary reason a biopsy is performed is for diagnosis. It is recommended that as few IHC stains as possible be used to make the diagnosis. This will conserve tissue for biomarker testing.
- Unstained Slides. Cutting 15-20 unstained slides is considered best practices in tumor types such as lung where biomarker testing will be performed within 30 days. Long term storage of unstained slides is not recommended.
- Reduce the number of times the block goes on the microtome, because every time the block is put back on the microtome it must be refaced. This results in wasted tissue. This can be prevented by thinking ahead and cutting everything you know will be needed while the block is on the microtome.
References
- Collins BT, Murad FM, Wang JF, Bernadt CT. Rapid on-site evaluation for endoscopic ultrasound-guided fine-needle biopsy of the pancreas decreases the incidence of repeat biopsy procedures. Cancer Cytopathol. 2013;121:518-24.

-Tabetha Sundin, PhD, HCLD (ABB), MB (ASCP)CM, has over 10 years of laboratory experience in clinical molecular diagnostics including oncology, genetics, and infectious diseases. She is the Scientific Director of Molecular Diagnostics and Serology at Sentara Healthcare. Dr. Sundin holds appointments as Adjunct Associate Professor at Old Dominion University and Assistant Professor at Eastern Virginia Medical School and is involved with numerous efforts to support the molecular diagnostics field.
Microbiology Case Study: A 60 Year Old Male Status-Post Orthotopic Liver Transplant with Headache and Word-Finding Difficulty
Case History
A 60 year old male with a past medical history of ulcerative colitis requiring total proctocolectomy and immunomodulatory therapy followed by an anti-Tumor Necrosis Factor α blocker for the last two years and primary sclerosing cholangitis with subsequent decompensated cirrhosis that ultimately required an orthotopic liver transplant on tacrolimus and prednisone for immunosuppression presents 17 days post-transplant with worsening headache for two weeks with associated word finding difficulty and expressive aphasia.
Laboratory and Diagnostic Findings
Brain magnetic resonance imaging demonstrated, a “Heterogeneous, partially hemorrhagic and centrally necrotic mass within the posterior left temporal lobe…infectious etiologies such as pyogenic/non-pyogenic abscesses to include fungal organisms, are highest on the differential” (Image 1). At the time of admission, his complete blood count demonstrated a leukocytosis (16.48×109 cells/L), anemia (hemoglobin of 7.8 g/dL, hematocrit of 24.8%) and a normal platelet count (367×109 cells/L). The automated differential showed 82% neutrophils, 10% lymphocytes, 6% monocytes, 1% eosinophils, and 1% basophils. A lumbar puncture was performed to obtain cerebral spinal fluid (CSF) and the analysis showed a glucose of 60 mg/dL, protein of 34 mg/dL, nucleated cell count of <1, and 6 red blood cells (completely normal CSF indices). Broad spectrum antimicrobials (Vancomycin, Piperacillin/Tazobactam, Metronidazole and Micafungin) were initiated. A 1,3-β-D-glucan test had a result of >500 pg/mL in both serum and CSF. Galactomannan, Histoplasma urine antigen, Cryptococcus antigen and other fungal testing were negative. Antifungal therapy was changed to voriconazole. Craniotomy was determined to be the best course of action and the patient was taken to surgery for debridement and pathologic evaluation.
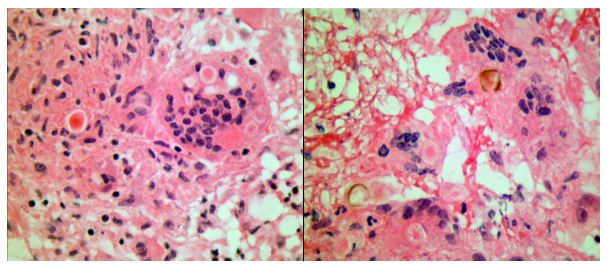
Frozen section evaluation during the time of surgery showed granulomatous inflammation. Septate hyphae were observed on the fungal smear. Following surgery, amphotericin was added. Histologic evaluation of the tissue submitted from surgery showed pyogranulomatous inflammation with pigmented, spore-like structures present in multinucleated giant cells on hematoxylin and eosin (H&E) stain (Image 2). Grocott’s methenamine silver (GMS) stain also highlighted short segments of septate hyphae (Image 3).
Cultures from the surgical debridement grew a mould with central pigmentation (Image 4). Direct microscopic examination of the mould revealed thick-walled, oblong conidia with 3-5 cells, and uniformly pigmented hyphae (Image 5). A germ tube test showed germ tubes originating from both ends of the conidia consistent with Bipolaris species.




The patient’s mental status significantly improved following surgical debridement, 2 weeks of liposomal Amphotericin B, as well as long term treatment with voriconazole. The voriconazole was later switched to posaconazole due to concerns for fluoride toxicity. He completed a year of posaconazole with significant improvement of the abscess observed on imaging and resolution of headaches with no other visual problems. He continued to recover cognitive function with some residual difficulty with reading, comprehension and speech that eventually resolved.
Discussion
Phaeohyphomycosis refers to infections caused by dematiaceous fungi that exist in a variety of forms when seen in tissues and commonly involves skin, soft tissue and nasal sinuses.1 In rare cases, central nervous system (CNS) involvement has been reported. CNS phaeohyphomycosis is predominantly seen in immunosuppressed patients; however, cases involving immunocompetent individuals do exist.2 In one case series from Houston, Texas, five of seven cases of cerebral mycosis were caused by a dematiaceous mould.3 Interestingly, the patient presented in this case came to medical attention around the Dallas-Fort Worth area of Texas.
Cladophialophora bantiana is the most common dematiaceous fungus associated with CNS phaeohyphomycosis, but rare cases of Bipolaris species have been reported previously in literature.4-6
We report a case of CNS phaeohyphomycosis by Bipolaris species following orthotopic liver transplant with an excellent patient outcome. This case is unusual, in part, because the typical hospital course of a patient with phaeohyphomycosis is generally dismal.7 The stories of successful treatment often involve complete debridement of discrete lesions.7-8 In our case, the patient underwent surgical debridement and treatment initially with liposomal Amphotericin B and later transitioned to long term therapy with newer azole antifungals.
References
- Revankar SG, Sutton DA, & Rinaldi MG, (2004). Primary Central Nervous System Phaeohyphomycosis: A Review of 101 cases. CID, 38, 206-2016
- Filizzola MJ, Martinez F, & Rauf SJ, (2003). Phaeohyphomycosis of the central nervous system in immunocompetent hosts: report of a case and review of the literature. Int J Infec Dis, 7, 282-286
- Raparia K, Powell SZ, Cernoch P, Takei H, (2010). Cerebral mycosis: 7-year retrospective series in a tertiary center. Neuropathology, Jun; 30(3): 218-223.
- Frank T, Esquenazi Y, Nigo M, Wanger A, Portnoy B, & Shepard S, (2016). Disseminated Phaeohyphomycosis with Brain Abscess and Biliary Invasion Due to Bipolaris spp. In an Immunocompetent Patient. Annals of Clinical & Laboratory Science, 46(4).
- McGinnis MR, Campbell G, Gourley WK, & Lucia HL, (1992). Phaeohyphomycosis Caused by Bipolaris spicifera, An Informative Case. Eur. J. Epidemiol, 8(3), 383-386
- Rosow L, Jiang JX, Deuel T, Lechpammer M, Zamani AA, Milner DA, Folkerth R, Marty FM, & Kesari S, (2011). Cerebral phaeohyphomycosis caused by Bipolaris spicifera after heart transplantation. Transpl Infect Dis, 13, 419-423.
- Dixon DM, Walsh TJ, Merz WG, McGinnis MR, (1989). Infections due to Xylohypha bantiana (Cladosporium trichoides). Rev Infect Dis, 11: 515-525.
- Gadgil N, Kupfermen M, Smitherman S, Fuller GN, Rao G, (2013). Curvularia brain abscess. J Clin Neurosci, Jan;20(1): 172-175.
-John Markantonis, DO is a second year Clinical Pathology resident at UT Southwestern in Dallas. He has interests in Medical Microbiology and Transfusion Medicine.
-Dominick Cavuoti, DO is a Professor at UT Southwestern in the Department of Pathology. He is multifaceted and splits his time as the Medical Director of the Parkland Hospital Clinical Microbiology Laboratory and Parkland Cytology attending among other administrative and educational activities.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
Friday Poll: IgM Anti-Ku Antibody
To learn more about the first published case of IgM anti-Ku antibody, read the Lab Medicine paper.
A New MLS Graduate’s Experience
I wrote last as a student in the medical technologist program at NorthShore University Healthcare System in Evanston. Now, as my first post as a certified medical technologist, I wanted to share what the journey was like becoming certified, finding a job, and transitioning into the professional arena.
Throughout the program, I felt relatively confident in the material and what we were learning and applying in rotations. We took about 1000 tests over the course of the program – at least that’s what it felt like. When the ASCP BOC exam began peaking its head, I wasn’t too intimidated. To me, it was just another test.
The first step was registering for the exam. My intention was to take the exam the day after I graduated, but I was bad and waited one month prior to graduation to register (it can take up to 45 business days to process). Don’t do as I did! Thankfully, the process was quicker than expected and I was only delayed one week after graduation.
The last four weeks of my program were intimidating to say the least! We had cumulative finals in addition to simulated board exams. Therefore, my BOC exam studying began through preparing for these. One of the most valuable resources that I cannot recommend enough is LabCE by MediaLab. I first discovered LabCE through their manual UA and differential simulators, but then discovered that they have testing simulators which our program director used to create practice exams for subjects and for the BOC exam. Their questions range in difficulty and each one has an explanation, which presents a great way to study (at least for me). It helped me develop study guides on material I consistently got wrong or completely forgot.
Two weeks before my exam, I discovered the BOC CLS study guide. I immediately paid for overnight shipping and received it the next day. This turned into my main study tool – I do best quizzing myself, then reading up on topics I got wrong. I would be lying if I said I felt confident when I received that book and went through the first 50 questions. I felt incompetent. Despite my previous review and studying, I felt as if I discovered an entirely new language. The book is very detailed and covers everything from a to z for laboratory science, with some topics only being covered briefly in school. As time went on, the shock factor wore off and I continued to focus on the things I no longer remembered and believed were important.
Despite the endless hours studying, I felt that there was much left to cover and the night before my exam I remember feeling overwhelmed. There is only so much information the human brain can store without the hands-on experience that ingrains what you learn. Throughout the test I felt as if I were failing, something that seems to be common place among BOC test takers. When it was time to see my score, my hands became clammy. Despite the suspense, I passed! When I received my scores later, I did much better than expected!
So, my concluding advice while preparing for the BOC exam is to focus on summarizations of your notes and to review all your formulas throughout your program. Go through as many practice exams as possible to help you see where you’re lacking and to prepare you for the wording on the BOC exam. Throughout my program, I would type up one to two-page notes for exams for later review. These were helpful when I had to go back and review things I did not remember. Additionally, despite the amount of studying you do, there is bound to be information you will not know and that’s okay. You know more than you think you know and through review you will only increase the recoverable information that is already in your head.
Lastly, I wanted to speak about the process of a new grad finding a job and transitioning from a student to a health professional. As I went through rotations, my passion for each specialty changed. At first, I wanted to be a generalist because I wanted to be more marketable and do everything. Then it was blood bank, then micro, and then came molecular (yay!). I began my job search about 2 months before graduation, and applied for those jobs about a month and a half before graduation. Being a soon-to-be new grad, I knew that I might not end up in the exact field I desired right away (which was molecular). I applied for mostly blood bank, micro, and molecular jobs – as these were of the most interest to me.
I applied for about 6-7 jobs in total and I ended up discovering, and eventually obtaining, my current position as an HLA molecular scientist at Northwestern’s transplant lab in Chicago. Throughout the interview process, being 100% honest of what you do and don’t know is the most important advice. Most employers ask a lot of detailed questions only to gauge where they need to start in your training. A good rule of thumb to remember is that if you’re a new grad being interviewed, then the employer is already okay with the fact that you don’t have much experience or knowledge of the specialty.
Before starting, a lot of people warned me about specializing immediately after graduating. While I hear their concerns, for me I plan on staying in the molecular field for the rest of my career – there are many opportunities and molecular is only becoming more and more advanced/widespread.
Now that I am 2 months into my job, I have fallen in love with it. There is endless opportunity to continue learning and to challenge myself. Walking into this specialty, I had two HLA lectures and nothing more. While my first month and a half mostly consisted of DNA isolation and cell lineage DNA isolation for chimerism tests, I have finally started training on an assay and data analysis for engraftment monitoring (chimerism). As a new grad in such a specific specialty, I have accepted that there will be a large learning curve. My advice is to keep your mind open to learning new things and fuel your motivation to learn more and more. Never stop asking questions and never turn down resources others hand you that have helped them.
As I gain more experience in the HLA world, I plan on writing articles tailored to this field and sharing what I learn. I hope my experience as a new grad helps others approaching this new time in their lives and gives them a sense of direction/confidence.

-Ben Dahlstrom is a recent graduate of the NorthShore University HealthSystem MLS program. He currently works as a molecular technologist for Northwestern University in their transplant lab, performing HLA typing on bone marrow and solid organ transplants. His interests include microbiology, molecular, immunology, and blood bank.
Microbiology Case Study: 18 Year Old Male with Shortness of Breath
Case History
A 18 year old male with no significant past medical history presented with 2-3 month cough, hemoptysis, fevers, night sweats and 15 pound unintentional weight loss. He originally started to feel mild shortness of breath with activity following his return from the Pacific Northwest. He was diagnosed with pneumonia and given antibiotics. He denied vaping, hookah use or any smoking. Of note, his maternal grandmother had pulmonary tuberculosis two years ago, but at that time he had a negative interferon-gamma release assay (IGRA). Since that time he had traveled extensively including Europe and Asia.
Upon admission, physical examination showed decreased breath sounds and coarse crackles in the right lower lung field. His blood test results were unremarkable. Chest X-ray and CT scan showed diffuse reticular pattern and a 4 cm cavitary lesion in his right lower lobe (Image 1). Brochoalveolar lavage fluid, sputum as well as blood were submitted to microbiology lab for bacterial, fungal and mycobacterial culture.

Laboratory results and management
The patient’s Quanti FERON®-TB Gold test (an IGRA) was positive.Laboratory studies including fungal culture to look for endemic fungi and HIV were negative. Auramine-rhodamine (acid fast) staining of sputum smear showed 4+ acid fast bacilli (AFB). Mycobacterium tuberculosis was confirmed by both our laboratory developed TB-PCR assay and a commercial TB-PCR assay (Xpert MTB/RIF). DNA sequencing was performed by the Centers for Disease Control and Prevention (CDC) in order to predict antibiotic susceptibility profiles for first-line anti-tuberculosis drugs including Ethambutol, Isoniazid, Pyrazinamide, and Rifampin. Because the result showed drug-susceptible tuberculosis, the patient started the first-line anti-tuberculosis drugs. Four days after admission, the patient discharged home with follow up with the department of health. After six weeks incubation, the sputum culture grew Mycobacterium tuberculosis with a pan-susceptible antibiotic profile.

Discussion
Mycobacterium tuberculosis (MTB) remains a global health problem. The continuing spread of drug-resistant tuberculosis is one of the most difficult challenges for MTB control. The CDC recommends rapid laboratory confirmation of MTB with using a nucleic acid amplification test (NAAT), followed early drug susceptibility testing. Our case is consistent with the previous reports that NAAT can identify MTB and DNA sequencing can determine the drug susceptibility within a few days. Our case can be summarized into two points.
First, early NAAT provided diagnosis MTB within 2 days after patient admission, enabling the timely initialization of infection control measures. Although culture remains the gold standard for laboratory confirmation of active TB infection, it can take 6-8 weeks to grow in a culture media since MTB is slow growing pathogen. Early laboratory confirmation of MTB with NAAT led rapid initiation of the patient treatment and transmission interruption.
Second, DNA sequencing guided us to start an optimal anti-tuberculosis treatment within 3 days because of the accurate prediction of susceptibility profiles for first-line anti-tuberculosis drugs. In comparison, the conventional susceptibility testing with the drug-containing medium requires 1 month to complete beyond initial growth and identification of the organism. Recent studies demonstrated high accuracy of genotypic predictions (>91.3 % sensitivity; >93.6% specificity). Our case supports a theory that DNA sequencing can help to determine which anti-tuberculosis drugs should be used for treatment.
Despite the notable advantage, NAAT has limitations. There is a relatively low positive predictive value in smear-negative pulmonary MTB. Recent meta-analysis found that overall sensitivity of NAAT to be 90.4% for diagnosis of pulmonary MTB. The sensitivity of the NAAT further defined to be lower in smear negative (75%) compared to smear positive (98%) pulmonary MTB. Additionally, cost effectiveness of NAAT and DNA sequencing is another concern. Further assessments of the benefit of NAAT and DNA sequencing utilization for smear negative MTB are needed.
In conclusion, our case demonstrated that NAAT and DNA sequencing was beneficial to reduce the time to initiation of an optimal MTB management.
References
- Prediction of Susceptibility to First-Line Tuberculosis Drugs by DNA Sequencing. N Engl J Med 2018; 379: 1403-15.
- Use of Nucleic Acid Amplification Tests in Tuberculosis Patients in California, 2010-2013. Open Forum Infect Dis. 2016 Oct; 3(4): ofw230.
- Assessment by Meta-Analysis of PCR for Diagnosis of Smear-Negative Pulmonary Tuberculosis. J Clin Microbiol. 2003 Jul; 41(7): 3233-3240.
-Sachie Ikegami MD, PhD is a 1st year anatomic and clinical pathology resident at University of Chicago (NorthShore). Sachie’s academic interests include neuropathology and molecular pathology. She is passionate about understanding how pathology informatics improving clinical practice. Outside of the lab, she enjoys jogging.

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
