Case History
A 60 year old male with a past medical history of ulcerative colitis requiring total proctocolectomy and immunomodulatory therapy followed by an anti-Tumor Necrosis Factor α blocker for the last two years and primary sclerosing cholangitis with subsequent decompensated cirrhosis that ultimately required an orthotopic liver transplant on tacrolimus and prednisone for immunosuppression presents 17 days post-transplant with worsening headache for two weeks with associated word finding difficulty and expressive aphasia.
Laboratory and Diagnostic Findings
Brain magnetic resonance imaging demonstrated, a “Heterogeneous, partially hemorrhagic and centrally necrotic mass within the posterior left temporal lobe…infectious etiologies such as pyogenic/non-pyogenic abscesses to include fungal organisms, are highest on the differential” (Image 1). At the time of admission, his complete blood count demonstrated a leukocytosis (16.48×109 cells/L), anemia (hemoglobin of 7.8 g/dL, hematocrit of 24.8%) and a normal platelet count (367×109 cells/L). The automated differential showed 82% neutrophils, 10% lymphocytes, 6% monocytes, 1% eosinophils, and 1% basophils. A lumbar puncture was performed to obtain cerebral spinal fluid (CSF) and the analysis showed a glucose of 60 mg/dL, protein of 34 mg/dL, nucleated cell count of <1, and 6 red blood cells (completely normal CSF indices). Broad spectrum antimicrobials (Vancomycin, Piperacillin/Tazobactam, Metronidazole and Micafungin) were initiated. A 1,3-β-D-glucan test had a result of >500 pg/mL in both serum and CSF. Galactomannan, Histoplasma urine antigen, Cryptococcus antigen and other fungal testing were negative. Antifungal therapy was changed to voriconazole. Craniotomy was determined to be the best course of action and the patient was taken to surgery for debridement and pathologic evaluation.
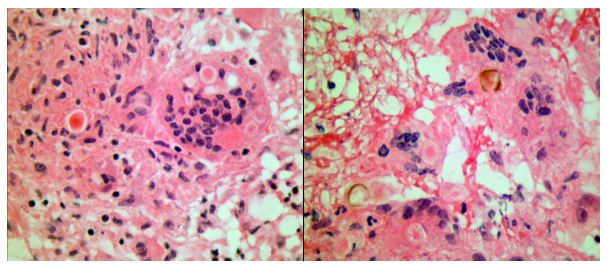
Frozen section evaluation during the time of surgery showed granulomatous inflammation. Septate hyphae were observed on the fungal smear. Following surgery, amphotericin was added. Histologic evaluation of the tissue submitted from surgery showed pyogranulomatous inflammation with pigmented, spore-like structures present in multinucleated giant cells on hematoxylin and eosin (H&E) stain (Image 2). Grocott’s methenamine silver (GMS) stain also highlighted short segments of septate hyphae (Image 3).
Cultures from the surgical debridement grew a mould with central pigmentation (Image 4). Direct microscopic examination of the mould revealed thick-walled, oblong conidia with 3-5 cells, and uniformly pigmented hyphae (Image 5). A germ tube test showed germ tubes originating from both ends of the conidia consistent with Bipolaris species.




The patient’s mental status significantly improved following surgical debridement, 2 weeks of liposomal Amphotericin B, as well as long term treatment with voriconazole. The voriconazole was later switched to posaconazole due to concerns for fluoride toxicity. He completed a year of posaconazole with significant improvement of the abscess observed on imaging and resolution of headaches with no other visual problems. He continued to recover cognitive function with some residual difficulty with reading, comprehension and speech that eventually resolved.
Discussion
Phaeohyphomycosis refers to infections caused by dematiaceous fungi that exist in a variety of forms when seen in tissues and commonly involves skin, soft tissue and nasal sinuses.1 In rare cases, central nervous system (CNS) involvement has been reported. CNS phaeohyphomycosis is predominantly seen in immunosuppressed patients; however, cases involving immunocompetent individuals do exist.2 In one case series from Houston, Texas, five of seven cases of cerebral mycosis were caused by a dematiaceous mould.3 Interestingly, the patient presented in this case came to medical attention around the Dallas-Fort Worth area of Texas.
Cladophialophora bantiana is the most common dematiaceous fungus associated with CNS phaeohyphomycosis, but rare cases of Bipolaris species have been reported previously in literature.4-6
We report a case of CNS phaeohyphomycosis by Bipolaris species following orthotopic liver transplant with an excellent patient outcome. This case is unusual, in part, because the typical hospital course of a patient with phaeohyphomycosis is generally dismal.7 The stories of successful treatment often involve complete debridement of discrete lesions.7-8 In our case, the patient underwent surgical debridement and treatment initially with liposomal Amphotericin B and later transitioned to long term therapy with newer azole antifungals.
References
- Revankar SG, Sutton DA, & Rinaldi MG, (2004). Primary Central Nervous System Phaeohyphomycosis: A Review of 101 cases. CID, 38, 206-2016
- Filizzola MJ, Martinez F, & Rauf SJ, (2003). Phaeohyphomycosis of the central nervous system in immunocompetent hosts: report of a case and review of the literature. Int J Infec Dis, 7, 282-286
- Raparia K, Powell SZ, Cernoch P, Takei H, (2010). Cerebral mycosis: 7-year retrospective series in a tertiary center. Neuropathology, Jun; 30(3): 218-223.
- Frank T, Esquenazi Y, Nigo M, Wanger A, Portnoy B, & Shepard S, (2016). Disseminated Phaeohyphomycosis with Brain Abscess and Biliary Invasion Due to Bipolaris spp. In an Immunocompetent Patient. Annals of Clinical & Laboratory Science, 46(4).
- McGinnis MR, Campbell G, Gourley WK, & Lucia HL, (1992). Phaeohyphomycosis Caused by Bipolaris spicifera, An Informative Case. Eur. J. Epidemiol, 8(3), 383-386
- Rosow L, Jiang JX, Deuel T, Lechpammer M, Zamani AA, Milner DA, Folkerth R, Marty FM, & Kesari S, (2011). Cerebral phaeohyphomycosis caused by Bipolaris spicifera after heart transplantation. Transpl Infect Dis, 13, 419-423.
- Dixon DM, Walsh TJ, Merz WG, McGinnis MR, (1989). Infections due to Xylohypha bantiana (Cladosporium trichoides). Rev Infect Dis, 11: 515-525.
- Gadgil N, Kupfermen M, Smitherman S, Fuller GN, Rao G, (2013). Curvularia brain abscess. J Clin Neurosci, Jan;20(1): 172-175.
-John Markantonis, DO is a second year Clinical Pathology resident at UT Southwestern in Dallas. He has interests in Medical Microbiology and Transfusion Medicine.
-Dominick Cavuoti, DO is a Professor at UT Southwestern in the Department of Pathology. He is multifaceted and splits his time as the Medical Director of the Parkland Hospital Clinical Microbiology Laboratory and Parkland Cytology attending among other administrative and educational activities.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
