Case History
An 80 year old female had a history of chronic iron deficiency anemia with unknown cause and comorbidities included hypothyroidism, congestive heart failure (CHF), severe aortic stenosis and COPD. The patient presented at the ED with initial presentation with increasing shortness of breast, NYHA class 3-4. She was admitted to the hospital for further treatment for CHF, as well hyperventilation, sleep apnea and COPD. Her serum iron and iron saturation were tested and results were 2 umol/L (reference range for iron: 10-29 umol/L) and 7% (reference range: 14-51%), respectively. Part of her investigations included a qualitative fecal test to screen for gastrointestinal bleeding. The immunochemical fecal occult blood test was performed using a CLIA waived Hema Screen SpecificTM POCT test (Immunostics, Inc, USA) in the hospital lab. Hema Screen Specific test is a qualitative, sandwich dye conjugated immunoassay that uses a combination of monoclonal and polyclonal antibodies to detect the globin component of hemoglobin in the fecal samples. The manufacture recommended using Hema Screen Specific test in routine physical examines, hospital monitoring of bleeding in patients and for screening for colorectal cancer or gastrointestinal bleeding for any source (statement from the product package insert).
The specimen submitted to the lab was markedly red (Image 1), yet Hema screen test returned a negative result. Since this device is designed to detect occult blood in fecal samples, a prozone effect was suspected, as the stool appeared to contain overt hemorrhage. The specimen was reanalyzed with serial dilutions by a factor of 5, 10, and at 100 × dilution. The FIT result became clearly positive for blood (Image 2). The patient received a colonoscopy, which revealed internal hemorrhoids, severe diverticulosis in the left colon, as well as multiple angiodysplastic lesions. One such lesion was in the ascending colon and was actively bleeding at the time of colonoscopy. The others, which were not bleeding, were distributed in the proximal ascending colon, hepatic flexure, and proximal transverse colon. All angiodysplastic lesions were treated with argon plasma coagulation.


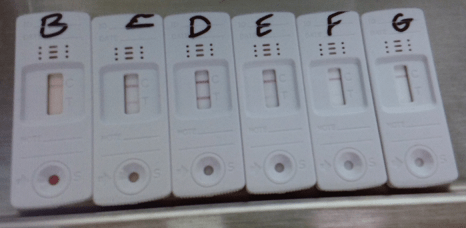
Moreover, we have tested the device with another bloody fecal sample during the initial evaluation. When an appropriate dilution factor was used, the prozone effect begins to lose its interference as show in Image 3.
Discussion
The prozone effect (or Hook effect) has long been appreciated as a source of interference in immunoassays.1 It typically occurs in sandwich assays, of which the FIT test is an example.2 When the concentration of the analyte is excessively high, it oversaturates the capture and detection antibodies in favor of forming single antibody:analyte complexes, rather than sandwiches. This results in a false negative result where the assay is unable to detect the analyte. The solution to the prozone effect is serial dilution to lower the concentration of the analyte.
The FIT test is designed to detect microscopic amounts of blood, hence its function in screening for fecal occult blood. A number of hospital labs use this test in an acute care setting to screening bleeding in patients. However, its capacity is oversaturated in specimens containing overt hemorrhage, as in our patient. In these cases it is nevertheless important to prove that the red color of the specimen is truly due to blood, as bright red stool can be caused by a wide range of dietary factors. Some examples are red food coloring, beets, cranberries, and tomato juice.3 If these possibilities are not ruled out, the patient may become subject to the risks of unnecessary endoscopy. Serial dilution of the specimen is extremely useful in this type of situation.
References
- Dasgupta A, Wahed A. Clinical Chemistry, Immunology and Laboratory Quality Control: A Comprehensive Review for Board Preparation, Certification and Clinical Practice. Amsterdam: Elsevier; 2014. 2.11.
- Allison JE, Fraser CG, Halloran SP, Young GP. Population Screening for Colorectal Cancer Means Getting FIT: The Past, Present, and Future of Colorectal Cancer Screening Using the Fecal Immunochemical Test for Hemoglobin (FIT). Gut and Liver. 2014 Mar;8(2):117-30. https://doi.org/10.5009/gnl.2014.8.2.117
- Picco MF. Stool color: When to worry [Internet]. Mayo Clinic; 2019 Feb 19 [cited 2019 Feb 23]. Available from: https://www.mayoclinic.org/stool-color/expert-answers/faq-20058080

-Hao Li, MD is a currently a first year anatomical pathological resident at Western University, London ON, Canada. Prior to be a pathology resident, he was a neurosurgery resident at the University of Saskatchewan, Saskatoon SK, Canada. When he was at the University of Saskatchewan, he spent his third year primarily in neuropathology, with also some general anatomical pathology and clinical pathology. Through these experiences, he has come to realize that his passion and calling lay more in pathology than in surgery. He has successfully transferred into pathology, and started a new residency in anatomical pathology in July 2019. Having a background in the clinical neurosciences, he hopes to eventually pursue a fellowship in neuropathology, and possess the skill set to practice both anatomical pathology and neuropathology.
