“In a notice sent to blood centers and posted on the agency’s website Wednesday evening, the FDA said it is requesting all blood centers in Miami-Dade and Broward counties to ‘cease collecting blood immediately’ until those facilities can test individual units of blood donated in those two counties with a special investigational donor screening test for Zika virus or until the establishments implement the use of an approved or investigational pathogen-inactivation technology.”
Yesterday, Nature published a paper that might help in the fight against MRSA. In a nutshell, German researchers discovered that Staphylococcus lugdunensis–a common bacteria in commensal flora–produces a compound that reduces colonization with MRSA.
From the abstract:
“Notably, human nasal colonization by S. lugdunensis was associated with a significantly reduced S. aureus carriage rate, suggesting that lugdunin or lugdunin-producing commensal bacteria could be valuable for preventing staphylococcal infections.”
The transfusion community has targeted platelets as the primary culprit in transfusion-associated clinical sepsis and fatal microbial infection. Platelets (PLTs) are associated with a higher risk of sepsis and related fatality than any other transfusable blood component. Concerns over bacterial contamination in PLT concentrates prompted the US Food and Drug Administration (FDA) in 1986 to issue a memorandum limiting the storage time of platelet products to 5 days. Only recently did the FDA issue draft guidance describing bacterial testing to improve the safety and availability of PLTs, and outlined the steps necessary for transfusion services to extend apheresis PLTs to 7 days.
Microbial infections were the 4th leading cause of transfusion-related mortality, accounting for 8% of them between 2010 and 2014. PLT storage at ambient room temperature supports high titer bacterial proliferation. Skin flora are the most common source of contamination, occurring at the time of collection. Despite the introduction of improved pre-collection arm preparation and analytically sensitive culture-based bacterial detection methods, the risk of fatal and non-fatal clinical sepsis has persisted.
Most recently, the 2016 AABB standards stated that PLTs may be stored for 7 days only if: 1) storage containers are cleared or approved by FDA for 7-day PLT storage and 2) labeled with the requirement to test every product stored beyond 5 days with a bacteria detection device cleared by FDA and labeled as a “safety measure.” The Verax PGD test is a rapid, single use, lateral flow immunoassay, and the only rapid, day of transfusion test the FDA has cleared as a “safety measure.” The proprietary test detects surface bacterial antigens, namely lipotechoic acid found on gram positive organisms and lipopolysaccharide found on gram negatives. The PGD test as a “safety measure” is to be used in concert with culture, not replace it.
Approximately 2.2 million PLT transfusions are administered yearly in the United States, of which more than 90% consist of apheresis PLTs. If the available data were generalized to the entire US apheresis PLT supply, approximately 650 contaminated apheresis PLTs would be caught with the PGD test, preventing septic transfusion reactions and potential fatalities each year. The FDA approval of this test allows non-culture based testing to extend dating from 5 to 7 days and further closes the safety gap that exists in apheresis PLTs.
-Thomas S. Rogers, DO is a third-year resident at the University of Vermont Medical Center, a clinical instructor at the University of Vermont College of Medicine, and the assistant medical director of the Blood Bank and Transfusion Medicine service.
A 61 year old African American male presents to the emergency department with complaints of a productive cough, dyspnea and altered mental status. His past medical history is significant for HIV and currently he is non-compliant with his anti-retroviral medications. On arrival, he is found to be hypoglycemic (glucose 49 mg/dL) and tachycardic (heart rate between 160-180 beats/min). He lives in a group home and they report decreased oral intake for several days but he denies fever, chills, chest pain or abdominal pain. He is a tobacco smoker and admits to previous illicit drug use. On physical exam, he is lethargic and respiratory auscultation reveals coarse lung sounds, bilaterally. A chest x-ray shows bilateral interstitial and airspace opacities suggestive of an infectious process. His CD4 count is markedly decreased at 3 cells/cmm. Peripheral blood and bronchoalveolar lavage (BAL) fluid are sent to the hematology and cytology laboratories for microscopic examination. Blood and BAL specimens were also transported to the microbiology lab for bacterial, fungal and mycobacterial cultures.
Laboratory Identification
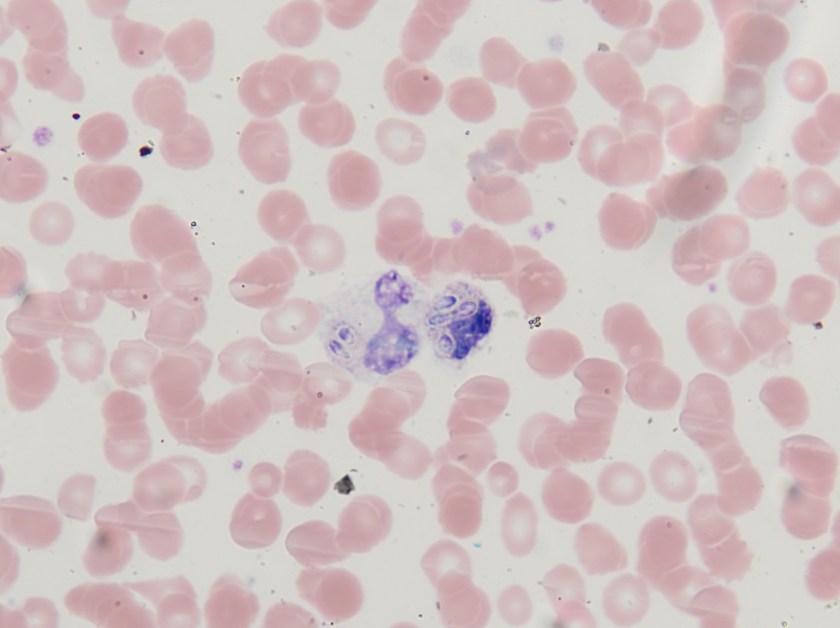
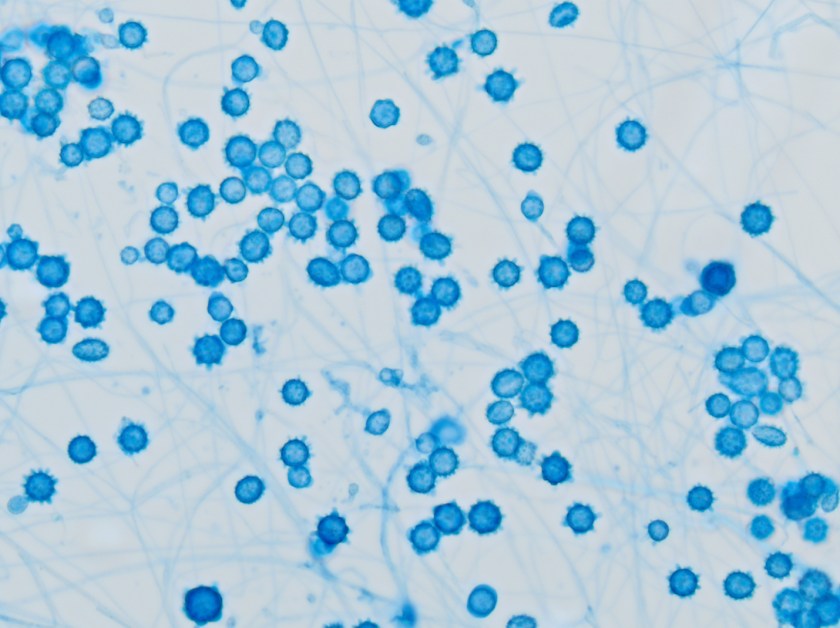
Figure 1. Peripheral blood smear highlighting small, intracellular yeast forms with narrow based budding (Giemsa stain, 1000x oil immersion).Figure 2. Fluid from a bronchoalveolar lavage showing macrophages filled with numerous small yeast forms that have an “acorn-like” appearance (Giesma stain, 1000x oil immersion).Figure 3. White colonies with a fine, cottony texture growing on Mycosel agar after 21 days of incubation at 25°C.Figure 4. Numerous tuberculate, thick-walled macroconidia with septate hyphae in the background (Lactophenol cotton blue stain, 400x).
Both the peripheral blood smear and BAL showed intracellular, small, ovoid yeast cells with narrow based budding (Figures 1 & 2). The yeast forms measured between 2-4 µm in diameter. The characteristic “acorn-like” appearance of the yeast cells surrounded by a thin halo is the result of staining fixation. The blood and the BAL cultures grew white colonies with a fine, cottony texture after incubation for 21 days at 25°C (Figure 3). The mold form grew on Sabouraud dextrose, SAB with chloramphenicol and Mycosel agars. Microscopic morphology of a lactophenol cotton blue prep illustrated septate hyphae bearing round to pear-shaped microconidia as well as tuberculate, thick-walled macroconidia, which measured between 8-15 µm in size (Figure 4). The dimorphic mold was confirmed to be Histoplasma capsulatum by DNA probe testing. The patient also had a positive Histoplasma urinary antigen and fungitell was found to be >500 pg/ml.
Discussion
Histoplasma capsulatum is a thermally dimorphic fungus and the most common endemic mycosis in North America. In the United States, the disease is most prevalent in areas surrounding the Mississippi and Ohio River valleys. Inhalation of conidia occurs as a result of environmental exposure to soil contaminated with bird dropping or exploring caves and other dwelling inhabited by bats. Pulmonary infections are the most frequent manifestation of disease; however, disseminated infection can occur in individuals with underlying cell-mediated immunological defects, including those with HIV, transplant recipients, and individuals receiving tumor necrosis factor alpha inhibitors for rheumatologic conditions. Other extra-pulmonary sites from which H. capsulatum has been isolated include the skin, liver, spleen, central nervous system and bone marrow.
In the environment and when cultured in the laboratory at 25°C, H. capsulatum is a filamentous mold and exhibits both pear shaped microconidia (2-5 µm) and thick walled macroconidia that display characteristic tubercles or projections on their surface (8-15 µm). The yeast phase occurs in tissue and at temperatures above 35°C. The yeast phase is characterized as small oval budding cells, 2-4 µm in diameter and are often found in clusters within macrophages. Historically, mold to yeast culture conversion was used to confirm the diagnosis, but with the advent of more rapid DNA probe technologies, this has been discontinued. Other rapid tests routinely utilized include a urine test to detect the Histoplasma antigen.
H. capsulatum var. duboisii, which is endemic in central and western Africa, is also implicated in causing disease in humans. It can be distinguished from H. capsulatum var. capsulatum due to its larger diameter in tissue where the yeast form of H. capsulatum var. duboisii measures between 8-15 µm in diameter as opposed to 2-4 µm for var. capsulatum. Caution is recommended, however, due to the yeast forms of the two variants being the same size when grown in culture.
Amphotericin B is the antifungal agent used to treat disseminated histoplasmosis infections. In cases of less severe disease, itraconazole is effective and commonly utilized. In the case of our patient, he received 14 days of amphotericin B infusion as an inpatient and was then transitioned to oral itraconazole upon discharge.
-Joy King, MD, is a third year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
Over on her blog, Maryn McKenna discusses the latest emerging microscopic threat: drug-resistant fungal infections. It mentions the organism Candida auris and states: “The Centers for Disease Control and Prevention (CDC) is so concerned that it recently sent an alert to U.S. hospitals, even though only one possible case of the resistant fungus has been identified in the United States so far.”
While equipment rental agency aren’t new–anyone who’s done a home renovation or taken a vacation is familiar when such services–I would guess that not many laboratory professionals would consider using one. A relatively new online equipment rental company called Kwipped is trying to change that.
You can read an article written by the company’s CEO here.
“The U.S. Food and Drug Administration today cleared for marketing the Xpert Carba-R Assay, an infection control aid that tests patient specimens to detect specific genetic markers associated with bacteria that are resistant to Carbapenem antibiotics.”
Have you ever felt like no one knows exactly what you do for a job; friends, family, even your colleagues? As a clinical pathologist, if you are ever asked what your job entails, it might take you a full 10 minutes to just explain the surface of it and by that time your audiences’ s eyes have glazed over and they are wondering when their next coffee break is. It can get pretty lonely when very few people understand your daily life of work.
I currently hold a general clinical pathology position and oversee the microbiology, chemistry, and immunology sections of a community hospital laboratory that services two hospitals totaling a little over 500 beds. I also get consulted on point of care testing and consult at two critical access hospitals that have a general AP/CP pathologist directing their lab.
As a new clinical pathologist, I was asked to blog about my experiences during the first year of working in the real world. I thought it would be a great venue to talk about how I have combatted the “loneliness” I face when I feel like no one knows what I do. Over the next couple of months I will highlight some of the tasks I have undertaken in my current position and I’d also love to hear what other clinical pathologist’s careers look like and/or how they have evolved over the years.
The beauty of a career in clinical pathology was explained to me by an attending during my residency training –you make of it what you want to. He also told me to not venture into the lab because they will ask you to do things, and since I am not very good at following advice, that is exactly the first topic I would like to explore: getting into the lab on a daily basis.
When I was in training, one of the best ideas I took away for my job was microbiology rounds. The first attending I observed holding these was a medical microbiologist that would round through the micro lab every day asking the techs if they had any odd cultures, questions that needed to be answered or anything that required follow up. When I took this job, I knew I wanted to incorporate this type of rounding as part of my work. My office is conveniently located at the back of the microbiology laboratory, so as I walk through the lab, I make it a point to say hi and ask the technologists if they have any issues, or any interesting cultures. It is not a formal rounding, but issues come out of these interactions and give me items to follow up with on a daily basis. Having my office located in the lab also allows the techs to come to me throughout the day with any questions they may have and has established a great rapport between us.
I also round through the chemistry and immunology section of the lab, specifically hitting second shift, as they lack a lot of interaction with clinicians. This has been a harder task for me because my subspecialty training was microbiology. I feel comfortable interacting with the technologists and lab staff, but when I first started I had the fear that I would not know the answer to a question I might be asked. Lucky for me, there are not as many questions that come out of these rounds. But of the questions I have gotten and I did not know the answer, it has never been a problem by me saying “I don’t know off the top of my head, but let me get back to you”. It also helps that I drop off candy in the break room while they wait on me – it is truly amazing how chocolate helps you make friends (thanks for the tip, Mindy Kaling). In addition to troubleshooting, rounding through the lab has given me the opportunity to interact with other people who have a passion for laboratory medicine. The techs will get just as excited about an interesting organism that was isolated or a new instrument we might bring in, and it is great to be able to share that passion you feel for your job with others.
Next month I will discuss a little more about the “formal” interactions I have set in the lab, but for now, let’s hear from you: how do you get involved in the lab and the technologists you work with?
-Lori Racsa, DO, is the director of microbiology, immunology, and chemistry at Unity Point Health Methodist, and a Clinical Assistant Professor at the University Of Illinois College Of Medicine at Peoria. While microbiology is her passion, has a keen interest in getting the laboratory involved as a key component of an interdisciplinary patient care team.
A 42 year old woman presented to her primary care physician after noticing a slightly tender lump in her left breast. After an inconclusive mammogram, the mass was biopsied, revealing no malignancy, but acute and chronic inflammatory changes with granulation tissue. Acid fast bacilli and Gomori’s methenamine silver stains were negative for organisms on this biopsy. The mass continued to enlarge over this time, and the overlying skin became erythematous with no active drainage. She underwent needle aspiration of the mass and the fluid obtained was sent for routine culture.
Laboratory Identification:
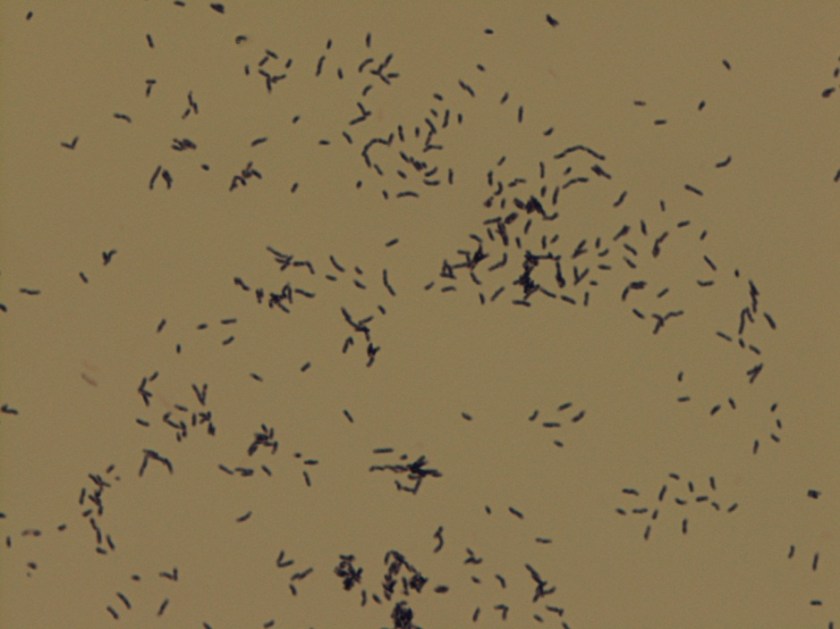
Colonies grown on routine culture were gram stained, and the smear revealed beaded gram-positive bacilli. Acid-fast and modified acid-fast stains were performed, revealing a partially acid fast organism. The culture was sent out for identification and susceptibilities, which came back as Gordonia bronchialis. It was susceptible to all drugs tested (amoxicillin/clavulanate, cefepime, ceftriaxone, imipenem, ciprofloxacin, moxifloxacin, amikacin, tobramycin, doxycycline, minocycline, TMP/SMX, linezolid) with the exception of an intermediate susceptibility result for clarithromycin.
Gordonia bronchialis is an aerobic, gram positive, partially acid fast, branching, filamentous bacteria that can fragment into rods and cocci. On agar, the colonies can be somewhat pigmented, dry, and raised. It is an uncommon pathogen, and is acquired from environmental sources such as soil, farm animals, and water.
Most infections occur in immunocompromised hosts, often in association with intravascular catheters. Gordonia bronchialis has been reported to cause osteomyelitis, bacteremia, pleural infection, intraventricular shunt infection, and sternal wound infection. One case series of seven patients in a single hospital contracting sternal wound infections with G. bronchialis traced these infections back to a nurse anesthetist. One case report was found in the literature of a recurrent breast abscess caused by Gordonia bronchialis, which required months of doxycycline therapy as well as repeated incision and drainage procedures.
It is unclear how the patient in this case acquired the organism; a thorough infectious disease work-up revealed no signs of immunocompromise, and she had no history of trauma or surgery to the area. Of note, she did have acupuncture performed on her shoulder several months prior to presentation, but no acupuncture was performed in the region of the abscess.
Gordonia bronchialis tends to be widely susceptible to antibiotics; however, treatment failures are frequent. It is believed that the tendency of the organism to form sessile colonies explains these failures.
The patient in this case is currently being treated with Bactrim and Augmentin. Her abscess was re-aspirated several weeks after initiation of therapy when it continued to enlarge, and the second culture is once again growing Gordonia bronchialis. The abscess seems to be improving since this second aspiration, so the treatment team currently plans to continue with oral antibiotics and forego a further incision and drainage procedure.
References:
Richet HM, et al. A cluster of Rhodococcus (Gordona) bronchialis sternal-wound infections after coronary-artery bypass surgery. N Engl J Med 1991;324:104–109.
Siqqiqui N et al. Tibial osteomyelitis caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2012;50(9):3119-21.
Werno AM et al. Recurrent breast abscess caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2005;43(6):3009-10.
-Laurie Griesinger is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Over the years, many safety standards and guidelines have been published regarding the Physical Environment of the laboratory (or the Environment of Care). The laboratory environment is not inherently a safe space, so training lab staff about their physical environment is critical so that they may work there without harm. The Physical Environment (PE) includes the overall laboratory space, electrical safety, and compressed gas safety. Physical Environment safety is concerned with ensuring that the facility is constructed, arranged, and maintained to ensure staff and patient safety.
Many labs I have visited are old, and space is often at a premium. Technology has changed over the years in the field of lab medicine, and that has led to the need for different floor plans, counter arrangements, and even work flow patterns. In any lab, the space should be arranged so that the quality of work performed, the safety of the staff, and any patient care given are not compromised. That means there should be enough space to perform the testing required in the department. There should also be room (offices or counter space) for those who perform the administrative work it takes to keep a lab running. Other facilities needs should be available as well such as storage space, rest rooms, staff lockers, a break room, and even meeting space.
One aspect of PE that needs scrutiny is the actual environment (temperature and humidity) of the lab space. The room temperature and humidity need monitoring and controls in order to properly store items in the space, and to ensure that testing is performed in the proper environment determined by the test manufacturer. Working outside of those parameters can have a direct negative impact on patient care. The other important consideration for the environment is staff comfort. Many building systems struggle with maintaining the proper temperature and humidity, especially in the extremes of hot and cold weather months. Will the lab staff remove PPE because it’s too hot? Of course that is an unsafe practice, and finding ways to manage the environment for staff comfort is critical.
Electrical safety should also be considered when evaluating the laboratory Physical Environment. Make sure employees have electrical safety training, and teach them about common errors made from not properly understanding electrical safety. One common error is the use of extension cords. In most locales, extension cords may be used in the lab in an emergency situation (such as accessing emergency power outlets during a power outage), but they should never be permanently placed and used for any lab equipment. The use of “daisy chains” is another common mistake. A daisy chain is made by plugging one multi-plug adapter into another for length. This is a fire hazard and should be avoided.
Compressed gas tanks are often found in the lab environment, and staff needs to adhere to special safety considerations regarding those tanks. Make sure all tanks are secured with a chain or other stabilizing device. A tipping tank, if it breaks open, can blast off like a rocket and cause great damage or even kill. Some tanks have even been propelled through walls or floors. Always transport tanks of compressed gas on a cart, dolly, or hand truck, and ensure all tanks are clearly labeled at all times.
Other considerations in the lab physical environment include the overall neatness and cleanliness of the space. Safety for the staff is improved in a clean and orderly work area. Biohazard work area floors should be wet-mopped at least once a day. Histology and other lab areas that use paraffin in their procedures should make sure the floors are cleaned and scraped so that they are not slippery from the wax. Laboratory counter tops should be neat and orderly, and they should be disinfected after each working shift using a 10% bleach solution or bleach product.
Education and training about PE topics is clearly important, but it is also valuable to regularly monitor the lab space to ensure that safety is maintained. Perform regular (monthly or quarterly) audits on the lab physical environment using a checklist. Use a complete list that covers all of the areas discussed, and be sure review every item on the checklist each time the audit is performed. It is surprising how quickly and easily things change in the lab work space. For example, an analyzer may have been moved for repair and placed back into its original location- but what if that movement caused fraying in the electrical cord? Now there is a fire hazard that didn’t exist just days before, and it needs to be rectified quickly. Sometimes we take for granted the spaces in which we work, but in the laboratory it is important to remember that PE safety needs attention, maintenance, and regular checks. Performing these functions can transform an inherently dangerous space into one in which patient results can be obtained safely.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.