Case History:
A 42 year old woman presented to her primary care physician after noticing a slightly tender lump in her left breast. After an inconclusive mammogram, the mass was biopsied, revealing no malignancy, but acute and chronic inflammatory changes with granulation tissue. Acid fast bacilli and Gomori’s methenamine silver stains were negative for organisms on this biopsy. The mass continued to enlarge over this time, and the overlying skin became erythematous with no active drainage. She underwent needle aspiration of the mass and the fluid obtained was sent for routine culture.
Laboratory Identification:
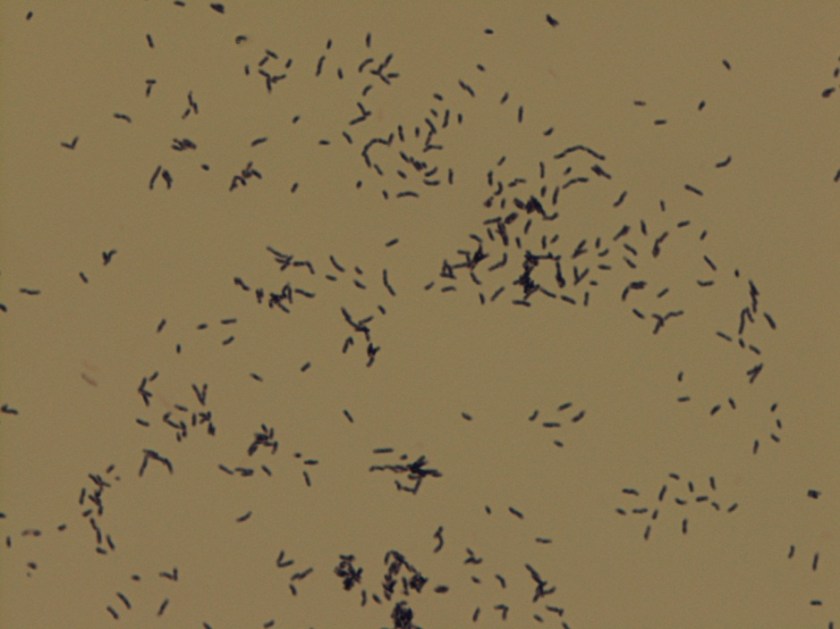
Colonies grown on routine culture were gram stained, and the smear revealed beaded gram-positive bacilli. Acid-fast and modified acid-fast stains were performed, revealing a partially acid fast organism. The culture was sent out for identification and susceptibilities, which came back as Gordonia bronchialis. It was susceptible to all drugs tested (amoxicillin/clavulanate, cefepime, ceftriaxone, imipenem, ciprofloxacin, moxifloxacin, amikacin, tobramycin, doxycycline, minocycline, TMP/SMX, linezolid) with the exception of an intermediate susceptibility result for clarithromycin.


Discussion:
Gordonia bronchialis is an aerobic, gram positive, partially acid fast, branching, filamentous bacteria that can fragment into rods and cocci. On agar, the colonies can be somewhat pigmented, dry, and raised. It is an uncommon pathogen, and is acquired from environmental sources such as soil, farm animals, and water.
Most infections occur in immunocompromised hosts, often in association with intravascular catheters. Gordonia bronchialis has been reported to cause osteomyelitis, bacteremia, pleural infection, intraventricular shunt infection, and sternal wound infection. One case series of seven patients in a single hospital contracting sternal wound infections with G. bronchialis traced these infections back to a nurse anesthetist. One case report was found in the literature of a recurrent breast abscess caused by Gordonia bronchialis, which required months of doxycycline therapy as well as repeated incision and drainage procedures.
It is unclear how the patient in this case acquired the organism; a thorough infectious disease work-up revealed no signs of immunocompromise, and she had no history of trauma or surgery to the area. Of note, she did have acupuncture performed on her shoulder several months prior to presentation, but no acupuncture was performed in the region of the abscess.
Gordonia bronchialis tends to be widely susceptible to antibiotics; however, treatment failures are frequent. It is believed that the tendency of the organism to form sessile colonies explains these failures.
The patient in this case is currently being treated with Bactrim and Augmentin. Her abscess was re-aspirated several weeks after initiation of therapy when it continued to enlarge, and the second culture is once again growing Gordonia bronchialis. The abscess seems to be improving since this second aspiration, so the treatment team currently plans to continue with oral antibiotics and forego a further incision and drainage procedure.
References:
Richet HM, et al. A cluster of Rhodococcus (Gordona) bronchialis sternal-wound infections after coronary-artery bypass surgery. N Engl J Med 1991;324:104–109.
Siqqiqui N et al. Tibial osteomyelitis caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2012;50(9):3119-21.
Werno AM et al. Recurrent breast abscess caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2005;43(6):3009-10.
-Laurie Griesinger is a Pathology Student Fellow at University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.

Very interesting. Thank you.
Nice work! But it’s Gomori’s methenamine silver, not gamori
Thanks for spotting that! We’ll fix it. –The editor
The Intermediate result for clarithromycin makes me wonder whether it possesses an inducible erm gene.
Interesting and valuable case