Inspections are a great learning opportunity. Our recent American Association of Blood and Biotherapies (AABB) introduced us to the risk analysis requirement in its 2024 checklist. Though the requirement is specifically stated in 3.7 Information Systems #13, the requirement can be applied to instruments as well as software. The update is significant as it emphasizes the need to proactively identify, assess, and mitigate risks associated with introducing or modifying software and instruments within the laboratory setting.
AABB-accredited laboratories will need to review their validation procedures to ensure they include a risk analysis with mitigation for identified risks. There are a few steps to conducting a risk analysis.
First, clearly define the changes being made. This could include new software installations, updates to existing software, introduction of new instruments, or modifications to current equipment. Understanding the full scope of changes is essential for a comprehensive risk analysis.
Secondly, if possible, form a multidisciplinary team that includes IT specialists, laboratory managers, quality assurance personnel, and end-users. In reality, for many small to medium laboratories, frequently one person fills more than one role. It’s conceivable for the laboratory manager to be the quality person and an end user since they often may have to fill in during staff shortages.
Next, identify the risks. Structured techniques like Failure Modes and Effects Analysis (FMEA) can be used to identify potential risks. Consider software-based risks such as data loss or corruption, system incompatibility, user interface issues, and cybersecurity vulnerabilities. Calibration errors, operational failures, compatibility with existing systems, and maintenance requirements are some instrument-based risks that should be considered. And, of course, human-based risks involving user errors, poor or insufficient training, and workflow disruptions.
The fourth step would be to assess each identified risk, assessing its potential impact on laboratory operations and patient safety and evaluating the likelihood of occurrence and the severity of consequences if the risk materializes. Use a risk matrix to categorize risks as low, medium, or high.
For each high or medium risk identified, develop mitigation strategies to reduce the likelihood of occurrence or minimize the impact. Some examples are increasing training programs, additional testing, or developing contingency plans for failures.
Ensure the entire risk analysis process is documented, including the identified risks, evaluation results, and mitigation strategies. Documentation is crucial for compliance with the AABB checklist and is a reference for future audits or inspections.
The risk analysis requirement in the AABB’s 2024 checklist underscores the importance of proactive risk management in clinical laboratories. Through the implementation of the outlined steps, laboratories can not only meet this requirement but also enhance their operational resilience and commitment to patient safety. Conducting a thorough risk analysis for software and instrument changes is an investment in the quality and reliability of laboratory services, ultimately contributing to better patient outcomes.
-Darryl Elzie is the Regulatory Affairs Manager Inova Blood Donor Services. He has been an ASCP Medical Laboratory Scientist for over 25 years, performing CAP inspections for two decades. He has held the roles of laboratory generalist, chemistry senior technologist, and quality consultant. He has a Master’s in Healthcare Administration from Ashford University, a Doctorate of Psychology from The University of the Rockies, and is a Certified Quality Auditor (ASQ). Inova Blood Donor Services is the largest hospital-based blood center in the nation. Dr. Elzie is also a Counselor and Life Coach at issueslifecoaching.com.
On May 11, 2023, the FDA’s Center for Biologics Evaluation and Research (CBER) issued guidance updating the blood donor history questionnaire (DHQ). Also known as the DHQ v4.0. The hope was that creating a gender-neutral questionnaire would increase the number of people eligible to donate, improving the nation’s blood supply.
After 3 months, has it made a difference?
The DHQ v4.0 is a series of questions asking potential donors about their lifestyle activities and travel to assess whether they are eligible to donate blood. The questionnaire is a risk-based model and is a critical step in ensuring the safety and potency of the nation’s blood supply.
As knowledge and understanding about disease increases along with the ongoing need to maintain an adequate blood supply, the FDA, in conjunction with the Association for the Advancement of Blood and Biotherapies (AABB), reviewed the restrictions or limitations on groups or individuals who may be allowed to donate with the goal of increasing the pool of eligible donors.
The DHQ v3.0 contains gender-specific questions impacting the eligibility of LGBTQ members. The new DHQ v4.0 was developed to be gender-neutral. There was concern that the new questions (especially the follow-up if any were answered yes) would be uncomfortable, but they were necessary to assess every potential donor the same.
“Some of the follow-up questions can seem to be a bit personal,” states Marvin Opulencia, Donor Operation Trainer at Inova Blood Donor Services (IBDS).
But Marvin thinks the change was a good thing because the questionnaire is no longer gender-specific and makes the process easier. “Some of my friends are members of the LGBTQ community, and now they are able to donate. I’m happy about that.”
Recognizing the difficulty and sensitivity inherent in the impacted topics, the FDA did not issue a deadline for implementation but has allowed blood donation centers to integrate the new guidance at their own pace. However, there were some blood donor centers that were ready to move forward with the recommendations. Their experience tells us that it is still too early to evaluate the effect of the change.
Nicholas Lilly, Interim Director of IBDS in Northern Virginia, believes we still don’t know the overall impact of the DHQ v4.0. “Inova Health System welcomes and supports initiatives improving the diversity, inclusiveness, and equity of our services. That’s why we were one of the first to implement the DHQ v4.0 in June. We serve the DMV area (D.C., Maryland, and Virginia), which is a highly diverse community, and so we saw the new guidance as a continuation of our vision and goals.”
With three months of data to evaluate, Director Lilly still doesn’t know what impact the change has on the blood supply. “Though we have received no negative feedback from our clients, we still haven’t seen a net increase in the number of donors. We have seen more non-binary people donate, but overall, there has not been a noticeable increase in donations. But it’s still early.”
It was expected that changing the Individual Donor Assessment to a more gender-neutral questionnaire would generate a bit of consternation and questions regarding whether it was in the nation’s best interest. However, so far, it was just one more step toward allowing everyone to make a difference.
Stated simply, Blood Saves Lives and is desperately needed. Now everyone has the opportunity to donate. Limitations or restrictions should be determined by science-backed non-judgmental research. That’s what the DHQ v4.0 is… that’s the difference it makes.
–Darryl Elzie is a Quality Consultant for Inova Blood Donor Services. He has been an ASCP Medical Technologist for over 25 years, performing CAP inspections for 15+ years. He has held the roles of laboratory generalist and chemistry senior technologist. He has a Master’s in Healthcare Administration from Ashford University, a Doctorate of Psychology from The University of the Rockies, and is a Certified Quality Auditor (ASQ). Inova Blood Donor Services is the largest hospital-based blood center in the nation. Dr. Elzie is also a Counselor and Life Coach at issueslifecoaching.com.
One of my favorite things about working in Hematology is handling those “difficult” samples. You know the ones. The one that some techs put aside to work on “later,” or they might decide it’s time to take a break when they see them coming. I love investigating and working on these interesting but perhaps uncooperative samples. At times this involves running samples in different modes, making new slides or albumin smears, and diluting samples. At other times, we investigate a delta or unusual results by checking patient diagnosis and previous results or by calling the care provider for more information and clues to help us resolve the problem.
I’m sure you’ve all seen the sayings “Without the Lab, you’re only guessing” and “Laboratory Professionals get results.” Physicians rely on the lab every day for information used to help diagnose and treat patients. Therefore, our goal is to deliver to the care provider the best possible results in a timely manner. Which means that we don’t just report results because that’s the answer the instrument gave us. With today’s instruments and middleware, we get very accurate and precise results, and about 85% or more of hematology specimens autovalidate. This is important because it leaves us time to work on those specimens with flags, and discrepancies; the ones that need a little more time and attention.
When faced with unusual or conflicting results, we first need to ask ourselves if we are dealing with a spurious sample, interfering substances or true abnormal results. Many labs today use middleware that will give the operator alerts when a sample needs to be investigated. These alerts give us suggestions as to how to handle the specimen but are usually short phrases triggered by certain values or flags and cannot be all encompassing. Operator alerts cannot tell us all the steps we may need to follow to resolve, for example, deltas, platelet clumps, abnormal scattergrams or a possible cold agglutinin. The alerts are great guidelines but it is often necessary to do more. We may need to refer to procedure manuals for SOPS or check instrument manuals or technical bulletins to decide how to handle these specimens. Sometimes we need to be detectives to report the most accurate results. We must review results with a critical eye, use all that “stuff” we learned in school, and be able to make educated decisions based on this investigation.
In my experience, one of the most common troublesome and perhaps misunderstood specimens I see is the one with a “hemoglobin (Hgb) interference” flag. An instrument flag “suspect, turbidity /Hgb interference?” is generally initiated when the MCHC is above a certain value. In our hematology lab, we see this flag when the MCHC is above 37.5 g/dL. What this is telling us is that turbidity may be present in the diluted and lysed sample. This turbidity can interfere with the Hgb detection light path and falsely increase the Hgb. Because the MCH and MCHC are calculated using the Hgb, these parameters are also affected. BUT, an MCHC >37.5 g/dL is not always something that can be or that needs to be corrected. With any parameter 95% of normal values will fall within 2SD of the mean. This means that 5% of normal healthy individuals have MCHC results <32 g/dL or >36 g/dL, and a few may have an MCHC over 37.5 g/dL. An MCHC >37.5 g/dL therefore can indicate a normal specimen, such as in a healthy young male with a Hgb at the high end of the reference range. High MCHCs can also be seen routinely in specimens from patients with spherocytosis or hemoglobinopathies such as Hgb SS, Hgb SC or Hgb C disease. In these conditions the RBCs are hyperdense due to altered surface volume and this leads to a high MCHC.
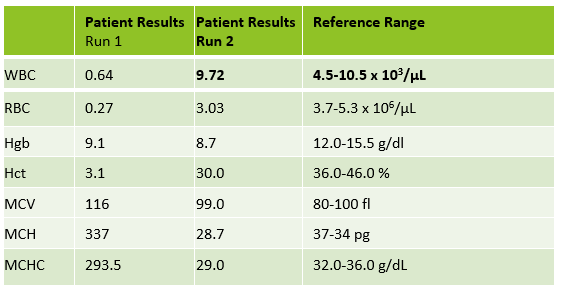
On our instrument, an MCHC >37.5 g/dL will cause a Hgb/Turbidity flag. An asterisk (*) will appear next to the Hgb, MCH and MCHC. The middleware triggers an operator alert that says “MCHC >37.5. Incubate at 37C for 30 mins. Evaluate for lipemia, icterus, hemolysis, Plasma replacement if indicated, rerun”. So, what’s the first thing to do?? Incubate? Hold on…not so fast. This is one of those instances where hematology is not just black and white. This operator alert is giving us suggestions of how to handle a specimen, but techs need to evaluate the specimen before jumping on the ‘cold’ wagon. Incubating will usually help resolve a cold agglutinin, but won’t help with a sickle cell specimen, or resolve one that’s icteric or lipemic. A grossly hemolyzed sample can give a spurious high MCHC result and, if so, needs to be recollected, not warmed. Putting a specimen that’s hemolyzed or lipemic or icteric in the heating block for 30 or more minutes would only delay reporting of results. My first case example involves a 45 year old female. The MCHC on initial run was 38.1 and the specimen gave a Hgb turbidity flag. The sample was incubated and rerun several times. After 1 hour of incubation, the MCHC was reported as 37.1 with a comment “repeated after warming for 1 hour at 37C”. In this case the patient was a known sickle cell patient. Previous results show that this patient’s MCHC is typically high and previously reported results ranged from 36.1- 37.8 g/dL. When evaluating a specimen with a high MCHC it is important to check the pattern of results. In this case the MCHC was high but the MCV was low. This does not fit the pattern for a cold agglutinin. As noted above, super dense RBCs in sickle cell patients may cause a high MCHC. This specimen was warmed, and even though the MCHC was a bit lower after warming, it would have been acceptable to report the original run MCHC. Checking patient history and previous results, and reviewing the smear for morphology would have allowed these results to be reported in a timely fashion. The operator alert does say “incubate the specimen” but it also says to evaluate. Be sure to check the MCV and MCHC along with patient history before warming specimens that don’t fit the pattern of a cold agglutinin.
Table 1. Case 1 CBC. The patient is a 45 year old known sickle cell patient.
The second example is from a 75 year old male. The CBC flagged Hgb turbidity with an MCHC of 45.8 g/dL. The MCHC >37.5 operator alert triggered Checking the pattern of results for the indicies, the MCHC was very high and the MCV was low. In a specimen with a low or normal MCV and a high MCHC, lipemia, icterus, abnormal proteins or severe leukocytosis can be affecting the Hgb. On evaluation, this sample’s Hgb and Hct did not meet the ‘rule of 3’. The rules of 3 are now generally recognized to be valid only for samples when the RBCs are normal, but the * here is telling us that there is an interference affecting the Hgb. In these cases it is valuable to know what the interference is so we know how to handle the specimen. By spinning down a small aliquot, (or asking chemistry!) we can investigate for lipemia or icterus. The specimen was found to be grossly lipemic. Flagging guidelines for lipemic specimens suggest diluting the specimen 1:5 and rerunning. Alternately, with severely lipemic or icteric samples, plasma replacement procedure may be necessary to correct the results. In this case, a plasma replacement was performed. After a plasma replacement, the WBC, RBC, Hct, MCV and platelet count are reported from the original run. The Hgb interference is what was causing the problem. Thus, when you correct the Hgb you must always correct any indicies that are calculated with the Hgb. The Hgb from the plasma replacement sample is used and the MCH and MCHC are recalculated. Notice that the new lower Hgb value now matches the Hct.
Table 2. Case 2, a 75 year old male with lipemic specimen. Plasma replacement performed. WBC, RBC, Hct, MCV, and Plt were reported from original run. Hgb was reported from plasma replacement sample. MCH and MCHC were recalculated.
Case 3 is a sample from an 80 year old woman. This was an interesting sample because there were multiple things going on here. This patient had an initial result with a high MCHC and MCH, with decreased RBC and Hct. In this patient the initial WBC was 0.64 and the RBC was 0.31. The Hgb of 9.1 /dL was less than the Hct of 3.1 %. MCV was 116 fl and the MCHC was 293.5 g/dL! In specimens with a high MCV and high MCHC we can suspect a cold agglutinin. When the MCV is very high it is because the RBCs are going through the aperture as one big bunch and this is measured as the size of one RBC. Often the Hct is less than the Hgb. Sometimes the RBC and Hct are so low that it causes the MCV to be appear within normal range. On our instrument, a RBC count of <0.5 x106/μL will give a flag “abnormal RBC scattergram” but no other indicies related flags are generated, so we didn’t even get an operator alert to evaluate the MCHC. But, it’s clear there is something very wrong with these results. Warming the sample is used to loosen clumping of RBCs, which lowers the MCV and allows the RBCs to be counted. Make a smear to examine for RBC clumping and look at the sample tube. Many cold agglutinin samples will appear to be ‘grainy’ or have agglutination along the side of the tube. This is the time when we want to incubate the sample. To resolve a cold agglutinin, warming the sample is necessary. Sometime 30 minutes is enough, sometime they need to be incubated longer. Some cold agglutinins are so strong that after incubation a dilution or plasma replacement still needs to be done. Warming this sample did not lower the MCHC. After incubating, I diluted this sample, and also did a plasma replacement to see how results would compare. The new results matched. This sample took a bit more time than others but the cold agglutinin was resolved and we were able to report valid results.
Table 3. CBC results from 80 year old woman with cold agglutinin. Image 1. Tube from cold agglutinin specimen. Note agglutination in sample along sides of tube.
There are other factors that can affect the Hct or Hgb and cause a high MCHC. Icteric specimens act much like lipemic ones and the Hgb can be corrected with dilution or a plasma replacement. An electrolyte balance can affect the Hct. Abnormal proteins and severe leukocytosis can affect the Hgb. Grossly hemolyzed samples can have a high MCHC. It is important to evaluate the indicies in these samples and correlate the values with previous results and patient history. What concerns me is that I have seen samples being warmed that do not match the indicies patterns for cold agglutinins. I have seen samples from sickle cell patients signed out with a comment “warmed at 37C. Possible cold agglutinin.” I have seen lipemic or icteric samples that are reported out with high MCHCs, erroneously high Hgb or parameters that are not reported at all. While warming these samples may actually lower the MCHC a bit, it still usually remains on the high side and does not give us the clean results that dilution or plasma replacement will. A little extra time looking at the indicies can give us important clues as to how to handle these samples. Doctors use our results every day to make patient care decisions. We need to make sure that we are making decisions every day to give them the best possible results so that patients can get the best care possible.
Table 4. Evaluating high MCHC specimens.
References
Costa, B. M. B., Vellés, M. C., Viana, M. M. F. B., & Rebelo, C. I. M. (2018). Interference of cold agglutinin autoantibodies in erythrogram interpretation: a case report and literature review. Jornal Brasileiro De Patologia e MedicinaLaboratorial, 54(4). doi: 10.5935/1676-2444.20180043
Sysmex USA. XN-Series Flagging Interpretation Guide. Document Number: 1166-LSS, Rev. 6, March 2021
It’s not Black and White: Unraveling the puzzles of Hematology. Becky Socha MS, BB, MLS(ASCP) Mercy Medical Center, Baltimore, MD
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A 31 year old woman, gravida 1 para 0, 35 weeks pregnant, arrived in the emergency room via ambulance following a fall down the stairs. The ER ordered a CBC, Type and Screen and a Kleihauer-Betke (KB) test and sent blood to the lab. The KB result was positive with 1.1 % fetal cells. Hypothetically, if this was an exam question, you might be asked, “How many doses of Rhogam should be administered?” But, before you grab your calculators, let’s explore that a bit.
Hemolytic Disease of the Fetus and Newborn (HDFN) has been described since the early 1600s, before blood groups were recognized. In the early 1900s, pioneers in blood banking, Landsteiner and Weiner, discovered the ABO and Rh blood groups, and, later, the Rh system became associated with HDFN. However, the antibody related etiology and pathogenesis of HDFN was not recognized until the late 1930s. Thus, the disease was written about in memoirs of midwives and physicians as early as 1609, but the mechanism involved was not described for another 300 years. The KB test was developed in 1957 by Enno Kleihauer and Klaus Betke to quantitate fetal maternal hemorrhage (FMH). The KB test allows physicians to diagnose and monitor and to initiate therapy to prevent the effects of HDFN. Finally, considered one of the most significant successes in medicine, prophylaxis for Rh HDFN, Rh immune globulin (RhIg), became available in 1968. The KB test is used to quantitate FMH in RhD negative mothers and the results can be used to calculate dosage for RhIg to prevent immunization. The KB test became one of the earliest examples of using a laboratory test to determine the appropriate dosage of a drug.1
KB testing has traditionally been used for RhD negative women to detect FMH and to determine the appropriate dose of RhIg to prevent immunization. In an RhD negative woman, we are concerned with immunization if the baby and mother are not antigenically similar. An RhD negative mother is given a prophylactic dose of RhIg at 28 weeks gestation. After delivery, when a newborn has a positive DAT and the fetal screen is positive, a quantitative test is needed to determine the appropriate dose of RhIg. In prenatal maternal trauma, there can also be a fetal bleed. Much as in childbirth, in a trauma, the baby’s blood can enter the mother’s circulation. This indicates placental hemorrhage and can be a prediction of preterm labor. In prenatal maternal trauma, the KB test has been used as aid in diagnosis and prognosis of HDFN, preterm labor and fetal demise. It can be used to determine if there has been a fetal bleed, and if so, to determine how much RhIg should be administered.
But, did you know that the KB test can also be used to determine FMH in RhD positive mothers? This is considered an alternative usage of the test. In the labs where I did KB tests, most fetal screens in Blood Bank were held until the following morning and performed on day shift. So, any KB tests on postpartum patients were also mostly done on day shift. I worked 2nd shift, and it was not uncommon to see KB tests ordered on RhD positive women. In fact, most of the KB tests ordered on 2nd and 3rd shift were from the ER and on RhD positive mothers. With RhD positive mothers, providers are not concerned with the mother producing anti-D, so RhIg is not a concern. Therefore, the answer to the hypothetical question posed above, is that this mother did not need any RhIg because, by checking the lab results it would be noted that this woman was Rh positive with a negative antibody screen.
A study performed in 2004 at the Shock Trauma Center, University of Maryland in Baltimore, reported that pregnant trauma patients with positive KB tests often had pre term contractions All patients in their study who experienced preterm contractions had positive KB tests. None of the patients with negative KB tests had uterine contractions. The conclusion was that “Kleihauer-Betke testing accurately predicts the risk of preterm labor after maternal trauma. Clinical assessment does not.” 2 They additionally concluded that, with a negative KB test, electronic fetal monitoring could safely be reduced. The major statement of the study, which has been incorporated into practice guidelines was that KB testing is important for all pregnant trauma patients, regardless of Rh status.2,3
In 2019 the College of American Pathologists Transfusion, Apheresis and Cellular Therapy Committee sent a survey with their proficiency testing program to determine how many participating laboratories perform KB tests on Rh positive pregnant females. 52% of the labs who responded noted that they performed quantitative fetal hemoglobin testing for RhD positive women, and about 39% reported performing more than 20 tests a year. The CAP group also reviewed literature detailing 16 observational studies and concluded that the literature supporting relying on the KB as a predictor of fetal distress was lacking evidence and nonconclusive. Despite the fact that doctors are ordering these and many laboratories are still performing this test STAT on RhD positive mothers, different guidelines for practice are mixed regarding if and how the KB should be used in these RhD positive trauma patients. Furthermore, many labs responded on the survey that doctors considered these results very important but that the labs were not sure how the results helped guide management of the mother or fetus.4
One of the problems some of these guidelines cite is that the KB test may not be rapid enough to use in trauma situations. Now, I have to start by saying that KB tests are probably no tech’s favorite test. The last hospital I worked at did KB tests in Hematology. Before that I worked at a hospital where we did KB tests in Blood Bank. There seems to be no way to avoid them! I would have to agree that a KB is not at all rapid. The test is both time sensitive, always ordered STAT, and very time consuming. Hands on time is considerable. I’ve gotten 2 in one night, on 2nd shift with only 4 or 5 techs manning the whole lab, and that makes for a busy night! Add a trauma or 2 to the mix, or a few units to wash for the NICU and you know why “Kleihaur-Betke” are not our favorite words.
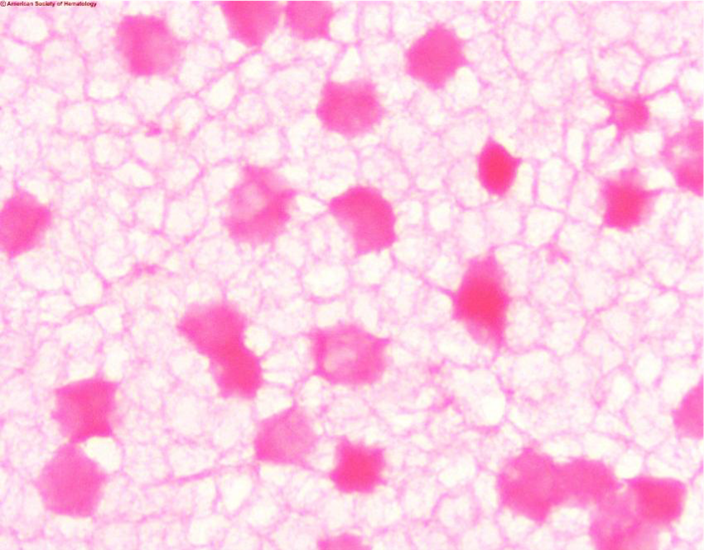
Another concern is that the KB test is marketed as a quantitative test. The problem with this is that it is not very precise due to technical difficulty. In the KB acid elution test the mother’s blood is treated with acid and then stained and counterstained. Fetal cells contain HbF which is resistant to acid and these cells will remain bright pink. The mother’s cells, which are primarily HbA, will appear as faint ‘ghost’ cells. 2000 cells are counted and the percent of fetal cells is determined. The test is complicated and needs precision in staining, counting and calculations. A slide that’s too thick, poor timing of steps, slides that are not adequately dried, or fetal cells that fail to stain can all affect results and cause false negative results. In pregnant women HbF may be increased, and in women with hemoglobinopathies such as sickle cell anemia and thalassemia Hb-F can be increased, leading to false positive results. As well, late in pregnancy it would be considered normal to have some fetal cells in the mother’s circulation. Thus, both false negative and false positive KB results are not uncommon, and a positive report on a KB test may not accurately predict fetal distress.
Image 1. Kleihauer-Betke stain showing dark ink fetal cells and ‘ghost’ like pale maternal cells
In the CAP survey article, it was noted that, of participating labs, about 96% did KB tests and 4% use flow cytometry.4 Flow cytometry is accurate, sensitive and reliable for HbF determination. Flow cytometry uses antibodies directed against fetal hemoglobin and antibodies directed against adult RBCs. A clear separation of populations can be identified and quantitated. Despite the fact that it is well known that flow cytometry is a much more precise test for FMH, many laboratories continue to do KB testing. This is likely due to the fact that only a small percentage of labs have flow cytometers. If, in trauma situations, physicians want HbF determination with a “fast” turnaround time, KB testing can be done in house with no equipment necessary. This is not fast, but would, in most circumstances, be faster than sending a test to a reference lab.
The KB test has historically been validated and used to estimate the total amount of FMH, and the results used to calculate if additional doses of RhIg are indicated. The test has high specificity for HbF but can be subjective. Precision between techs and even with the same tech repeating the test can be relatively low. Because of this, the formula used to calculate RhIg dosage has a factor built in to make up for any imprecision. An alternate usage of the test, and the one used in this case example, is to predict outcomes and guide treatment in maternal trauma victims, regardless of Rh status.
While there is some controversy on using the KB test in these cases, it is none the less still recommended by many authors and included in medical guidelines.5 Providers are using the KB test more and more for assessing placental hemorrhage in cases of trauma and premature labor. Though immunophenotyping by flow cytometry has a greater accuracy, the KB test can give reliable results at a lower cost and with a faster turnaround time.
As always, this blog led me off on several tangents while writing. When I have an idea for a blog, I start with a case study or an interesting sample I have seen in the lab. The case study itself is the easy part, then I start researching and reading articles about the disorder, test or phenomenon that I am writing about. Often, when I read one article, I ask myself another question and say, “what if…?” and that leads to another article and another and another. Days later I can still find myself reading articles and chasing after more information. I love my job, I love being a Medical Laboratory Scientist and educator, and in true form of the curious MLS, I always want to investigate and never want to stop learning. Thus, this simple case about an alternative usage of Kleihauer-Betke (KB) test kept developing as I wrote. As a side note, it was interesting to see that the studies have had different conclusions and the guidelines for this use of the KB test have swayed over the years. It will be interesting to see what the future will bring. I have seen some articles about adding the HbF determination to hematology analyzers—wouldn’t that be nice!
References
Reali G. Forty years of anti-D immunoprophylaxis. Blood Transfus. 2007;5(1):3-6. doi:10.2450/2007.0b18-06
Muench MV, Baschat AA, Reddy UM, Mighty HE, Weiner CP, Scalea TM, et al. Kleinhauer-betke testing is important in all cases of maternal trauma. J Trauma 2004;57(5):1094-8.
Michael V. Muench, Joseph C. Canterino, Trauma in Pregnancy, Obstetrics and Gynecology Clinics of North America, Volume 34, Issue 3, 2007, Pages 555-583.
Matthew S. Karafin, Chad Glisch, et al, for the College of American Pathologists, Transfusion, Apheresis, and Cellular Therapy Committee; Use of Fetal Hemoglobin Quantitation for Rh-Positive Pregnant Females: A National Survey and Review of the Literature. Arch Pathol Lab Med 1 December 2019; 143 (12): 1539–1544.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
When I first thought of writing a blog on blood supplies amid the COVID-19 pandemic, it was early March. Fast forward a couple months and a lot of things have changed. So, where were we, and where are we now?
January 6, 2020
At this time, most people in the US were not even aware of the novel coronavirus. (unless you were taking my Introduction to Human Disease course and were searching online for media articles about infectious disease!)
I first became aware of this ‘mystery’ virus in early January, when I was teaching an online Winter session course called Introduction to Human Disease. I developed this course a number of years ago as a STEM course for non-science majors. The intent of the course is to familiarize students with diseases and disease terminology that they will use in their everyday lives. The course gives students a chance to learn basic medical concepts that will enable them to become their own (or their family’s) medical advocate. In addition, the course covers many diseases that are ‘in the news’ and allows students to gain some knowledge and insight into the myths and facts surrounding these diseases. Topics covered include general mechanisms of disease, including inflammation, infectious disease, immunity, heredity, and cancer. Emphasis is placed on emerging and pandemic …. so, when this disease emerged, we were right there to take note!
I asked the students to find an article in the media on an infectious disease, and to summarize and answer questions about the article and the mechanism of the disease. Three students chose different articles about this yet unnamed mystery illness affecting people in Wuhan, China. We had active discussion board conversations about this emerging severe respiratory disease and pneumonia, that at the time had infected around 40 people, with no reported deaths, and no human to human transmission. In my comments, I compared this novel virus to seasonal influenza, H1N1, SARS and MERS and tried to reassure students that this would hopefully follow the same path as H1N1 or SARS and MERS.
Feb 21, 2020
The first confirmed case in the United States was on Jan 21 in Washington state. (CDC)1 On Jan 31, the Health and Human Services Secretary declared Coronavirus a Public Health Emergency in the US. (HHS.gov)2 We began hearing news of restrictions on flights from China, passengers affected on Princess Cruise ships and outbreaks at a long term care facility in Washington State.
As a Medical laboratory Scientist, I became concerned with this virus early on, and started watching statistics. I was concerned not only for the health of my family, friends and coworkers, but also for the health or our laboratories and our blood supply.
The first journal articles I read about COVID-19 and blood safety were published in Transfusion Medicine Reviews on Feb 21, 2020. In the very early days of this novel coronavirus, researchers in China reviewed publications about SARS and MERS to help give us a better understanding of SARS-CoV-2, the virus that causes our current pandemic of COVID-19. When discussing blood safety, one of the first things to consider is if the virus is transmittable via blood transfusions. If the virus is transmittable, we also must consider if there is an asymptomatic time when there is virus in the blood. One review stated that SARS, MERS and SARS-CoV-2 can all be found in the serum or plasma, but, at the time of this review, it was still uncertain if SARS-CoV-2 could be transmitted from those with pre-symptomatic or asymptomatic infections.3
March 18, 2020
On March 18, Blood Transfusion published an article written by a group at several Blood Centers in a few provinces in China. This article discussed efforts to minimize the impact of blood shortages due to COVID-19. It was noted that the rising pandemic had had a profound impact on the number of blood donations, and on blood safety. Because it was now recognized that there is a long incubation period and a significant number of asymptomatic cases, this posed a huge challenge in recruiting blood donors. In China, strictly restricted mobility led to a decrease in donations across the country. Donors were recruited through various methods, including the use of social media. Social distancing during blood donations and thorough cleaning and disinfecting of donor areas were enforced. Screening procedures were enhanced to include temporary isolation of blood products for 14 days after collection and delaying release for clinical use. At the same time, donors were followed up until the expiration of the products. If a donor was found to test positive for COVID-19 after donation, the blood products were recalled. These new protocols in place were helping to insure adequate donations and the safety of blood products. ne interesting note is that this article referred to the epidemic as “effectively controlled” and that “normal medical services had been resumed”.4
Meanwhile, in the US, American Red Cross was pleading for blood donors. On March 17 it was reported that 2,700 mobile blood drives had been cancelled at a loss of 86,000 units of blood potentially collected. On March 21, 4 days later, that number had risen to more than 5,000 blood drives canceled at a loss of 170,000 units. As more schools, workplaces, churches and college campuses closed down in response to the pandemic, those institutions had to cancel their blood drives. Social distancing guidelines and shelter in place orders resulted in fewer people donating blood. In addition, an FDA mandate from February, that people who had traveled to areas with COVID-19 outbreaks should wait at least 28 days before donating blood, most likely contributed to the shortage. Dr. Justin Kreuter, from the Mayo Clinic Blood Donor Center, stated that the blood shortage was not due to more COVID-19 patients needing blood products. Rather, “it’s a lack of donations coming in.”5
April 1, 2020
procedures that the Chinese had instated. Mobile blood drives were shut down, but collection centers remained open. TV commercials, radio ads, You Tube videos and social media called for blood donors, assuring them that this was essential and that donating blood was safe. Donations were arranged through appointments only, and potential donors contacted and verbally screened for symptoms and risk factors before appearing to donate. On arrival at the centers, temperatures were taken and travel and symptoms questions were asked before a donor was allowed to enter the center. The use of masks and social distancing, along with extra cleaning and donor chair decontamination between donors were all implemented.
In an effort to open up the pool of potential donors, the FDA reviewed current studies and epidemiological data and concluded that certain donor eligibility criteria could be modified without compromising the safety of the blood supply. On April 2, 2020 the FDA approved several important changes in donor qualifications. These revisions included the following:
For male donors deferred for having sex with another male: the recommended deferral period changed from 12 months to 3 months.
For female donors deferred for having sex with a man who had sex with another man: the recommended deferral period changed from 12 months to 3 months
The deferral period for recent tattoos and piercing was changed from 12 months to 3 months
For people who have traveled to malaria-endemic areas, the recommended deferral period was changed from 12 months to 3 months. In addition, the guidance notes that deferral can be waived for these donors, provided the blood components are pathogen-reduced using an FDA-approved pathogen reduction device.
For donors who spent time in European countries or on military bases in Europe who were previously deferred due to potential risk of transmission of Creutzfeldt-Jakob Disease or Variant Creutzfeldt-Jakob Disease, the FDA has eliminated the deferrals and these individuals may now qualify to donate.6
Despite loosening requirements, advertising, and calls from the blood centers for additional donors, the shortages remained. To address the decline in blood product availability, it became essential to review the principles of patient blood management (PBM). PBM is defined as “the timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin concentration, optimize hemostasis and minimize blood loss in an effort to improve patient outcome.”7 Firstly, elective procedures were put on hold, thus freeing up units for the most needy patients. Despite this, many blood banks still had their standing orders decreased. In many cases, Blood bank Medical Directors approved changes in transfusion triggers. At the hospital where I work, the transfusion trigger was changed from a hemoglobin of 8g/dL to 7 g/dL. New changes of SOP were approved to issue to all patients, except females of child bearing age, Rh positive units instead of more scarce Rh negative units. We also have a large NICU unit and baby units were not available from ARC, so we were using the newest units available, when necessary for these patients.
By April 8, 15,000 blood drives had been cancelled across the US, at a potential loss of almost 500,000 donated units. One technologist reported in an online Blood bank professionals group, that “Our supplier downgraded us in terms of standard inventory (about 40%), but our transfusion numbers have dropped at least as much.”8 With the decrease in usage and the careful patient blood management, blood needs were met.
May 12, 2020
AABB began sending out a weekly COVID impact survey for hospital transfusion services survey in late March. Many questions on the survey, and the resulting charts and graphs, are related to COVID convalescent plasma practices and procedures (details in my next blog!), but one important graph produced by this survey shows the increase in inventory wastage due to changes related to COVID-19. These changes due to COVID-19 can be a decrease in patients and elective surgeries or changes in transfusion protocols. In early April, in the first few weeks of the survey, 25%-28% of hospitals responding reported an increase in inventory wastage. This corresponds to when donors started coming back to donate, and usage dropped. This percent of hospitals reporting wastage increased each week until the week of May 4-7 when 54% of hospitals reported inventory wastage. This may be due to several factors. The units collected at the end of March and early April, have reached their 42 day expirations. Donors came out initially in response to the call for blood, but now, these units have expired, and it has not yet been 56 days when these donors can donate again. Usage also decreased during this time. COVID patients have not generally had heavy use of red cells, in particular, and doctors have been very conservative in usage with all patients. For the week of May 11-14, as more hospitals are planning to resume elective surgeries, and for the first time in the 8 weeks, fewer hospitals (52.0%) reported an increase in wastage due to changes related to the pandemic. Of the 100 respondents, 59% reported they are resuming “some” elective surgeries before mid-May and 28.0% are doing so after mid-May.9
What does this mean for the future of our blood supply during this pandemic? On May 12, a group of Blood bank professionals, when asked in an informal online survey, had had varying answers. These were likely dependent on location, both geographic and city vs. rural, and size of the hospital. One comment was that “We have gone from huge shortages to throwing away massive units not being used. Hospital is empty.” Another tech said “We were way overstocked a week ago, now we’re dipping way below average.” Technologists in Florida, Oregon and Pennsylvania reported low inventory. Techs in Ohio and Maryland reported their inventory to be very healthy. But these reports could easily vary between areas of the individual state, and even different hospitals in the same city. Another technologist commented “We had a mass of donors when this all started and now all those units are expiring!” The shortage of donors will likely continue, but may relax a bit with some states beginning to lift restrictions. We likely won’t see a huge drove of donors, all at once, which is actually good because it will spread out expiration dates. But, though things may be opening up, it is unlikely that we will see blood drives at schools, workplaces and churches for some time, and this is a huge source of our countries blood supply.
We have seen a big swing in both inventories and usage. After elective and with surgeries have been put on hold for months, we may see an increase over the typical number of elective surgeries, which will mean we will see an increase in blood usage, and with a lack of donors, inventories may drop again.
As far as blood safety, we know now that SARS-CoV-2 did not follow the path of SARS and MERS. We know that it can definitely be transmitted from person to person, and can be transmitted by people who are asymptomatic. But, we also know that, in general, respiratory viruses are not known to be transmitted by blood transfusion. So, from what we know at this time, it is likely not necessary to routinely screen blood products for SARS-CoV-2, and not necessary to isolate blood products after collection and delay release of the products. It is recommended that blood centers encourage self-deferral for donors who have traveled to a COVID-19 affected area or been in contact with an infected person in the past 14 days and to screen donors carefully for fever and respiratory symptoms. With these practices in place, we can ensure an adequate and safe blood supply. We will continue to see swings in volumes, but with careful patient blood management, we will ride these waves and come out on top. Thanks to all our wonderful Blood Bank Technologists who are helping manage our country’s blood supplies!
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
In my July post, “Blood Bank Case Study:
What’s Your Type?” I discussed some of the dilemmas when dealing with a weak D
phenotype and the fact that there is no standard or general consensus as to the testing
performed or terminology to be used in resulting a weak D patient. Results
obtained on patient testing also vary depending on the method used, and the
anti-D reagent and enhancement used in testing. This can be confusing to medical
technologists, physicians and to patients.
For anyone who has not been in the Blood bank for a while, the Du variant was first
recognized in 1946 and renamed weak D in 1992. To
review last month’s blog, serologic studies have distinguished three broad
categories of D variants, weak D, partial D, and DEL, from conventional D. A
serologic weak D phenotype is one that has no or weak reactivity (≤2+) of RBCs
with an anti‐D reagent at immediate spin, but does agglutinate with antihuman
globulin. Since there is no general consensus on how labs perform
and report patient testing for weak D, it is left up to individual
interpretation as to what type blood these patients should receive, and, if
pregnant, if they should receive Rh D immune globulin (Rhogam). Last month I
focused on testing, resulting, donors and blood administration. In this blog I
will focus on issues concerning weak D in the obstetric population and how labs
can move forward now and in the future towards the best patient care and blood
management.
About 15% of
Caucasians are RhD negative. About 3% are weak D phenotypes.In the genral
population, this means that about 0.2% to
1.0% inherit RHD genes that code for serologic weak
D phenotypes.2 In Europe
and the US, weak D phenotypes are the most common D variants found, but we also know that the
prevalence of weak D phenotypes varies by race and ethnicity. Today we have
much more information about D antigen expression than we had in the past, because
we have the availability to genotype these weak D RBCs. We know that more than
84 weak D types have been identified, but types 1, 2, and 3 account for more
than 90% of these in people of European ethnicity.1 Currently,
with the mixed ethnicity population in the US, about 80% of people who inherit RHD genes for serologic weak D
phenotypes are found to be weak D
type 1, 2, or 3.3 We also know that
types 1, 2 and 3 are unlikely
to become alloimmunized to anti-D, so they can safely be treated as RhD
positive and receive RhD positive units.
The introduction of RhD immune globulin in 1968is one of the great success
stories in obstetrics. Rhogam has been used very successfully in developed
countries in the prevention and treatment of hemolytic disease of the fetus and
newborn due to RhD alloimmunization. The routine recommendation is that women
who are candidates for Rhogam receive one dose at approximately 28 weeks’
gestation and a second dose after the delivery of an Rh pos baby. Additional recommendations are for administration
of Rhogam after threatened miscarriage, abdominal trauma during pregnancy and
before invasive diagnostic procedures.
But,
who is a candidate? Any unsensitized woman who is RhD negative and who may be
carrying or who delivers an RhD positive baby is a candidate for Rhogam. And,
that brings us back to the problem that we have no standardization for the
reporting of serological weak D phenotypes.
As
an example, let’s look at a patient who has 3 children. Many labs do not do
weak D testing on patients and report anyone who is RhD negative at immediate
spin as RhD negative. This patient was typed at such a lab (Lab #1) as RhD
negative, and received Rhogam for her first pregnancy. During her 2nd
pregnancy, she had moved to a different state, and went to another lab (Lab #2)
for prenatal testing. This lab performed serologic weak D testing and found
this patient to be weak D positive and reported her type as RhD positive.
Rhogam was not further discussed during this pregnancy and the patient did not
receive Rhogam. The patient had blood drawn during her 3rd pregnancy
at yet a third hospital (Lab #3). Some labs distinguish women who are pregnant
or of childbearing age from the general population, and have different procedures
on the reporting of RhD type on these women. This hospital’s procedure was to
do weak D testing on all patients, but, in women of childbearing age, if weak D
positive, they report these women as RhD negative. The patient was told she was
RhD negative and would be a candidate for Rhogam. At this time the woman
thought she remembered that she didn’t get Rhogam with her second pregnancy and
was a little confused, but with 2 young children and pregnant with her 3rd,
she simply followed the doctor’s recommendation and didn’t question further.
When her 3rd child was 4 months old, she attended a Red Cross blood
drive at work and donated a unit of blood. Soon she received a blood donor card
in the mail that said she was RhD positive. At this point she was thoroughly
confused and questioned all the lab results she had had done over the past 6
years. On her next visit to the doctor she questioned her obstetrician. The
obstetrician recommended RhD genotyping. The woman was found to be weak D type
2. The doctor explained to her that all blood donors who are weak D are treated
as RhD positive, but, that as a patient, policies and procedures vary. However,
he also informed her that now that they had her genotype, she would be
considered RhD positive. He explained that the genotype was DNA testing, would
not need to be repeated, she would not need Rhogam for any future pregnancies
and she could safely receive RhD positive blood products.
The
American College of Obstetricians and Gynecologists (ACOG) guidance practice
bulletin of 1981 recommended that recommended that RhD‐negative women “whether Du positive or
Du negative” were candidates for Rhogam. Shortly
afterwards, that recommendation was
reversed and revised to read “[a]
woman who is genetically Du‐positive is Rh‐positive and
administration of Rh immune globulin is unnecessary.1 This remained the recommendation of the
group until the latest version of this publication in 2017. The 2017 ACOG
guidelines recommend giving Rhogam to weak D positive patients, “in appropriate
clinical situations, until further studies are available.”3 Another comparative
study published in 2018 reported inconsistency between national groups over how
to treat weak D phenotypes and recommended the creation of international
guidelines.4
Thus,
the controversy over whether a pregnant woman who is weak D positive is RHD
positive or RHD negative continues. The latest recommendations, and those of
ACOG, are for a move to genotyping patients with a serological weak D
phenotype. There are several benefits to this. As we can see from my case study
example, genotyping put this woman at ease and gave her definitive answers
about her blood type. It also can do the same thing for medical technologists
and physicians. RHD genotyping only needs to be performed once on a
patient. If performed at the first prenatal appointment, this would alleviate
much confusion as to procedures and how to report the results. I have in blood
bank, that whenever we have a weak D on a prenatal patient, there are questions
about how to result them, and we refer to the SOPs. We also occasionally get a
patient who had previously been typed elsewhere where the reporting procedures
were different and there is therefore an apparent discrepancy between the
current and historical typing. This causes frequent phone calls from physicians
and nurses asking for clarifications on weak D types, and questions about
Rhogam. Lastly, RHD genotyping could avoid confusion which could lead to
transcription and computer entry errors when entering types on these patients. RHD
genotyping would solve all of these problems and eliminate confusion.
Additional
benefits of RHD genotyping are, if RHD genotyping was performed
on all weak D transfusion recipients, we could save as many as 47,700 units of
RHD negative RBCs annually.3 With the availabilityof
molecular testing, there is no reason to administer RhD negative units to
patients who can use RhD positive units. This could help alleviate the constant
shortage of RHD negative units. With RHD molecular testing, these
critical units could be reserved for patients who are truly RhD negative.
It may not be feasible for all laboratories to perform molecular testing for RHD genotypes, but reference laboratories should offer affordable testing for the most prevalent and clinically relevant RHD genotypes. From a study done of over 3100 laboratories, it was found that, at this time in the US, most labs are managing weak D phenotypes as RhD negative. Laboratories not performing weak D testing are essentially avoiding their detection. Clinical laboratories should instead increase the detection of serological weak D and interpret these with the use of RHD genotyping. Rhogam shortages exists, and RHD genotyping could save thousands of injections of Rhogam annually in the US alone, and at the same time, avoid the unnecessary administration of products to patients. The work group study calculated that annually, approximately 24,700 doses of unnecessary Rhogam could be avoided.1 It is time to move forwards to molecular testing for the best patient care and blood management.
References
Sandler SG, Flegel, WA, Westhoff CM, et al. It’s time to phase in RHD genotyping for patients with a serologic weak D phenotype. Transfusion 2015;55:680‐9
Garratty G. Do we need to be more concerned about weak D antigens? Transfusion 2005;45:1547‐1551.
Practice Bulletin No. 181: Prevention of Rh D AlloimmunizationObstetrics & Gynecology: August 2017 – Volume 130 – Issue 2 – p e57-e70 doi: 10.1097/AOG.0000000000002232
Sperling, JD et al. Prevention of RhD Alloimmunization: A Comparison of Four National Guidelines. Am J Perinatol. 35(2):110-119. doi: 10.1055/s-0037-1606609. Epub 2017 Sep 14.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
The general public doesn’t always know a lot about laboratory
testing in general, but most people know a little about blood types, even if
it’s what they have learned from TV! Blood types do seem to come up in casual
conversation. We might hear a conversation about blood type after someone has
donated blood, or between family members comparing notes, who ask “What’s your
type?” Yet, even with medical technologists, there can still be some confusion
about blood types and blood typing, particularly if one has not worked in Blood
Bank in many years. I recently received an email from a colleague who had a few
questions about blood types, as she has not worked in Blood Bank for over 40
years. I always tell my students that no question is a bad question, and indeed,
she asked some very good questions, which I will address with this case study.
What blood type is listed on a patient’s chart if they type “O
Du”?
What blood type is recorded on a donated unit of blood typed “O
Du”?
What type of blood does an “O Du” patient receive?
Can an “O Du” patient have a transfusion reaction if they are
transfused with O positive blood? Would she need to receive O negative blood in
a transfusion?
Does an “O Du” patient need to receive RhoGAM if she pregnant and
her husband is Rh positive?
If you have ever wondered or can’t remember details about any of
these questions, you’re in the right place. So, what’s new, if anything, with
blood types?
Landsteiner discovered the ABO blood group system in 1901, and
identified A, B and O blood types, using experiments performed on blood from
coworkers in his laboratory. The discovery of the codominant AB blood type soon
followed, but it was not until around 1940 that the Rh blood group was first described.
In 1946, Coombs and coworkers described the use of the antihuman globulin (AHG)
to identify weak forms of Rh antibodies in serum. For us old blood bankers, the
original name for this test was the Coombs’ test. (You will still find
physicians ordering a Coombs’ test!) The current and proper name for this is
the direct antibody test (DAT), which is used to detect in vivo sensitization
of RBCs. AHG can also be used to detect in- vitro sensitization of RBCs using
the 2 stage indirect antibody test (IAT).
Since Landsteiner’s work, we have not discovered any new blood groups
that are part of the routine blood type. The ABO and Rh blood groups are still
the most significant in transfusion medicine, and are the only groups consistently
reported. However, we currently recognize 346 RBC antigens in 36 systems.1 Serological tests determine RBC
phenotypes. Yet, today we can also determine genotype with family studies or
molecular testing. This case study and 2 part blog reviews some terminology in
phenotyping, some difficulties and differences encountered, and explores the
possibility of RHD genotyping to assess a patient’s true D status.
Our case study involves a 31 year old woman who is newly married.
She is not currently pregnant, has never been pregnant, is not scheduled for
surgery but has had a prior surgery 15 years ago, and has never received any
blood products. She and her husband recently donated blood and, as first time
blood donors, just got their American Red Cross (ARC) blood donor cards in the
mail. The husband noted that his card says that he is type O pos. The woman
opens her card, and, with a puzzled look on her face, says “My card says I’m an
O Pos, too. There must be a mistake.” She knows she has been typed before and
checks her MyChart online. Sure enough, her blood type performed at a local
hospital is listed in her online MyChart as O negative. She further checks
older printed records and discovers that 15 years ago, before surgery, she was
typed at a different hospital as “O Du”. She is very upset, wondering how she
can have 3 different blood types. She is additionally concerned because they
are planning to have children and recalls being told that because she is Rh
negative, that she would need Rhogam. Is she Rh negative or positive, and what
does Du mean? Will she need Rhogam when pregnant? She has many questions and calls
the ARC donor center for an explanation.
What blood type is listed on a patient’s chart
if they type “O Du”?
What is happening here, what is this woman’s actual blood type, and what testing can be done to ensure accuracy in Rh typing? From the patient reports, it appears that this woman has what today we call a “weak D.” Du is an older terminology that should no longer be used, and that has been replaced by the term “weak D.” But, why does she have records that show her to be an O neg, a type O, Du (today, this would be written O weak D), and now, a card from ARC stating she is O pos?
RhD negative phenotypes are ones that
lack detectable D antigen. The most common Rh negative phenotype results from
the complete deletion of the RHD gene. Serologic testing with anti-D is usually
expected to produce a strong 3+ to 4+ reaction. A patient with a negative
anti-D at IS and at IAT would be Rh negative. If the patient has less than 2+ strong
reaction at immediate spin (IS), but reacts at IAT, they would be said to have
a serologically weak D.1 Historically, weak D red blood cells (RBCs)
are defined as having decreased D antigen levels which require the IAT for
detection. Today’s reagents can detect many weak D
types that may have been missed in the past, without the need for IAT. However,
sometimes IAT is still necessary to detect a weak D. When this is necessary is
dependent on lab SOPs and whether this is donor testing or patient testing. The
reported blood type of this patient also depends on the SOPs of the laboratory
that does the testing. And, the terminology used for reporting is also lab
dependent. It is not required by AABB to test patient samples for weak D
(except for babies of a mother who is D negative). There is also no general
consensus as to the terminology to be used in reporting a weak D. Some labs would
result this patient as O negative, weak D pos. Some labs may result O pos, weak
D pos. Others may show the individual reactions but the resulted type would be
O pos. Labs who do not perform weak D testing would report this patient as O, Rh
negative. The following chart explains why this patient appears to have 3 types
on record.
Figure 1. Tube typing results of same patient from different labs with different SOPs.
What blood type is recorded on a donated unit
of blood typed “O Du?”
AABB Standards for Blood Banks and
Transfusion Services requires all donor blood to be tested using a method that
is designed to detect weak D. This can be met through IAT testing or another
method that detects weak D. If the test is positive, the unit must be labeled
Rh positive. This is an important step to prevent alloimmunization in a
recipient because weak D RBCs can cause the production of anti-D in the
recipient. This also explains why the ARC donor card this patient received
lists her type as O pos.
What type
of blood does an “O Du” patient receive?
Historically, weak D red blood cells
(RBCs) were defined as having decreased D antigen levels which require the IAT
for detection. A patient who is serologic weak D has the D antigen, just in
fewer numbers. This type of weak D expression primarily results from
single-point mutation in the RHD gene that encodes for a single amino acid
change. The amino acid change causes a reduced number of D antigen sites on the
RBCs. Today we know more about D antigen expression because we have the
availability to genotype these weak D RBCs. More than 84 weak D types have been
identified, but types 1, 2, and 3 represent more than 90% of all weak D types
in people of European ethnicity.2 An Rh negative patient has no D
antigen and should, under normal circumstances, only receive Rh negative blood.
Yet, there has been a long history of transfusing weak D patients with Rh
positive RBCs. 90% of weak D patients genotype as Type 1, 2 or 3 and may
receive Rh positive transfusions because they rarely make anti-D. 2
It is now known that weak D can actually
arise from several mechanisms including quantitative, as described above, position
effect, and partial D antigen. Molecular testing would be needed to
differentiate the types, but, with the position effect, the D antigen is
complete and therefore the patient may receive Rh positive blood with no
adverse effects. On the other hand, a partial D patient may type serologically
as Rh negative or Rh positive and can be classified with molecular testing. It
is important to note that these partial D patients are usually only discovered
because they are producing anti-D. If anti-D is found, the patient should
receive Rh negative blood for any future transfusions.
Thus, 3 scenarios can come from typing
the same patient. With a negative antibody screen, and because 90% of weak D
patients have been found to be Type 1, 2 or 3 when genotyped, many labs do not routinely
genotype patients and will report the blood type as Rh pos and transfuse Rh pos
products. However, depending on the lab medical director and the lab’s SOPs,
these same patients may be labeled Rh neg, weak D and receive Rh negative
products. There is no general consensus on the handling and testing of weak D
samples. The 3rd scenario is that many labs do not test for weak D
in patients at all, and a negative D typing at IS would result in reporting the
patient as Rh neg, with no further testing. In this case, the patient would be
transfused with Rh negative products.
Can an “O
Du” patient have a transfusion reaction if they are transfused with O positive
blood? Would she need to receive O negative blood in a transfusion?
This question was covered
somewhat in the above discussion. Policies regarding the selection of blood for
transfusion are lab dependent, dictated by the lab medical director, and are
based on the patient population, risk of developing anti-D, and the
availability or lack of availability of Rh negative blood products. Anti-D is
very immunogenic. Less than 1 ml of Rh pos blood transfused to an Rh negative
person can stimulate the production of anti-D. However, not all patients
transfused with Rh positive blood will make and anti-D. As discussed above, 90%
of weak D patients are types 1, 2 or 3, would be unlikely to become
alloimmunized to anti-D. If a weak D patient with a negative antibody screen
receives a unit of D pos RBCs, there is a very small possibility that they are
a genotype who could become alloimmunized to the D antigen and produce anti-D. However,
as stated above, the majority of weak D patients can be
transfused with D positive RBCs. Thus, with few exceptions, from a historical
perspective, one can safely classify the weak D as D positive.
This question gets a little trickier
when dealing with females of childbearing age. We particularly want to avoid
giving Rh positive blood to females to avoid anti-D and the complications of
Hemolytic Disease of the Fetus and Newborn. Therefore, when dealing with these
patients, lab policies and physicians tend to be more conservative in their
approach to transfusion. The consequences, however, in males and older females
are less serious and these patients could be given Rh positive blood if there
exists a shortage of Rh negative units. Any patient who becomes alloimmunized
to the D antigen, would thereafter be transfused with Rh negative products.
Does an “O
Du” patient need to receive RhoGAM if she pregnant and her husband is Rh
positive?
This, again, would be up to the medical
director, the lab’s SOPs or the patient’s physician. Depending on lab practice,
the lab may or may not perform weak D testing. If the lab does not perform weak
D and results this patient as Rh neg, the patient would get Rhogam. If the lab
does do weak D testing and finds a weak D phenotype, the decision whether or
not to give Rhogam would be up to lab practices and the practitioners involved.
The lab’s policy on terminology used in resulting the type may also reflect the
decision whether or not to give Rhogam. This brings up a lot of questions in
the lab because we know that a patient who would not make anti-D would not need
Rhogam. So, what is the best course of action? Read my next blog to learn more
about troubleshooting and resolving D typing discrepancies!
From the discrepancies in reported type in this individual, and putting all the pieces of the puzzle together, we can conclude that this patient is a weak D phenotype. However, the type reported and the terminology used varies from lab to lab. Molecular testing is available, yet most labs are still using serological testing for blood types for both donors and patients. This is based on several factors within the lab setting. Stay tuned for my next Blood Bank blog exploring D typing discrepancies and the financial aspects of performing genotype on pregnant patients to clarify Rh type.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
A 28 year old
woman, gravida 1 para 0 presented to her OB/GYN for her first prenatal visit. A
type and screen was ordered and the patient typed as A pos, with a positive
antibody screen. Maternal history indicated that she had received several transfusions,
for a total of 5 units of blood, following an automobile accident 15 months
previously. An antibody identification was performed and Anti-K was identified
in her plasma. The patient sample was phenotyped and was confirmed to be K
negative.
Is the fetus at
risk for Hemolytic Disease of the Fetus and Newborn (HDFN)? How can we know? And,
if so, how should this pregnancy be monitored?
The answer to
these questions is not a simple answer, and depends on several factors. Let’s
look first at HDFN and its causes. HDFN is destruction of the RBC’s of the
fetus and newborn by antibodies produced by the mother. This happens in 2
steps. The first step is that blood containing
a foreign antigen enters the maternal blood stream and stimulates the mother to
produce unexpected IgG antibody. But, how is a mother exposed to these foreign
antigens? The mother is exposed either via a blood transfusion or a previous
pregnancy. In this case, this was the mother’s first pregnancy, however her
history revealed that she had been previously transfused. In order for the
mother to produce anti-K , she must be K antigen negative, which was confirmed
in the Blood Bank testing. She was exposed to the K antigen through transfusion
and produced the anti-K antibody to the foreign antigen. The second step in the
development of HDFN occurs when the
mother’s antibody crosses the placenta and binds
to this foreign antigen
present on the red blood cells of the fetus. This can lead to RBC
suppression, destruction, and fetal anemia.
Again, certain
criteria must be met. First of all, the antibody must be IgG. Only IgG
antibodies can cross the placenta. Active transport of IgG from mother to fetus
begins in the second trimester and continues until birth. Secondly, the mother’s
antibody is only of concern if the baby possesses the antigen that the mother
lacks. Where does the baby get an antigen
that is foreign to the Mom??
It’s the Dad’s Fault!! In HDFN, the mother lacks the antigen in question and the
fetus possesses the antigen, which is of paternal origin.
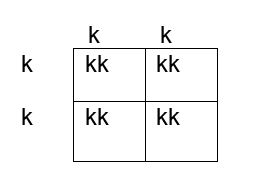
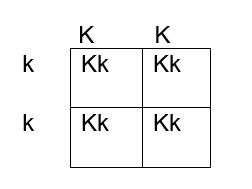
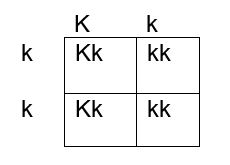
How do we determine if the fetus has the K antigen and is at risk? If you remember your genetics and Punnett squares, if the mother does not have the antigen and the baby does, the father must possess the antigen, because the baby gets an allele from each parent. This means that the fetus affected by HDFN is always heterozygous for the antigen in question. Figures 1, 2 and 3 below illustrate the possible inheritance patterns. In the first scenario, shown in Figure 1, the baby would not inherit a K antigen and would not be at risk for HDFN. In the Figure 2 scenario, the father is homozygous for K, and 100% of offspring from these parents would be K positive. Figure 3 illustrates a heterozygous father who would have a 50% chance of passing this gene to their offspring.
Figure 1. Punnett square showing inheritance of K antigen. Mother (on side) is negative for K (kk), father (at top) is also negative, homozygous kk
Figure 2. Punnett square showing inheritance of K antigen. Mother is negative for K (kk), father is homozygous KK
Figure 3. Punnett square showing inheritance of K antigen. Mother is negative for K, father is heterozygous Kk
The father was phenotyped as K positive. The father’s blood sample was sent out for further zygosity testing, and he was found to be heterozygous for the K antigen. Thus, the fetus had a 50% chance of being affected by HDFN, and further testing was performed. The mother’s antibody titer was 1:4. To avoid an invasive procedure such as amniocentesis or chorionic villus sampling (CVS) which may worsen maternal alloimmunization, fetal DNA was isolated from the mother’s plasma at 12 weeks’ gestation and the fetal genotype was determined. The fetus was determined to be K positive and at risk for HDFN.
The mother’s
titer and the fetus continued to be monitored. Diagnostic ultrasounds were performed to monitor fetal size,
age, and structural changes. At
16-18 weeks’ gestation, ultrasounds of the middle cerebral artery (MCA-PSV) were
performed to assess fetal anemia. MCV-PCA of 1.29 -1.5 multiples of mean (MoM)
for the gestational age is indicative of mild anemia. Higher values predict
moderate to severe anemia which require further intervention. At 18 weeks the
MCV-PCA was 1.27 MoM and the fetus was determined to be developing normally.
A type and screen and antibody titer at 28 weeks
showed the mother’s titer had increased, to 1:32, indicating that fetal RBCs
with K antigen had entered the mother’s circulation and were stimulating further
antibody production. Repeat MCV-PCA was 1.33, indicating mild anemia. Weekly
measurements of MCA-PCV were recommended. At 32 weeks, a sudden increase was
recorded, with MCV-PCA of 1.65 MoM. Cordocentesis was performed and fetal
hemoglobin was 6.2g/dl. Fetal DAT was positive and anti K was identified in the
eluate. An intrauterine transfusion (IUT) was performed. IUT was repeated at 34
and 36 weeks. The infant was delivered at 37weeks. The newborn required several
neonatal transfusions while in the hospital and was discharged to home 3 weeks
later.
Kell isoimmunization is the third most common cause of HDN
after Rh and ABO and the most clinically significant of the non-Rh system
antibodies in the ability to cause HDFN.
It tends
to occur in mothers who have had several blood transfusions in the past, but it
may also occur in mothers who have been sensitized to the K antigen during
previous pregnancies. Anti-K HDFN may cause rapidly developing severe fetal
anemia. Anemia and hypoproteinemia are dangerous to the unborn child because
they can lead to cardiac failure and edema, a condition known as hydrops
fetalis. The MCA-PSV is a non-invasive doppler measurement of peak systolic
velocity which is used to monitor fetal anemia. As mentioned previously,
MCV-PCA of 1.29 -1.5 multiples of mean (MoM) is indicative of mild anemia. Values
greater than 1.5 MoM are very sensitive and can be used to predict moderate to
severe anemia that would need intervention.
HDFN due to anti-K differs from ABO and Rh HDFN in that, in
HDFN due to K alloimmunization, Anti-K targets the RBC precursors. Remember
that the K antigen can be detected on fetal RBCs as early as 10 weeks. The primary mechanism of K HDFN is due to maternal
anti-K antibody actually
suppressing the fetal production of RBCs, rather
than hemolysis of mature fetal RBCS as seen in ABO and Rh HDFN. With reduced
hemolysis, amniotic fluid bilirubin levels also do not correlate well with the degree
of anemia. In addition, alloimmunization due to Anti-K differs in that even a
relatively low maternal anti-K titer can cause erythropoietic suppression and
severe anemia. In Rh HDFN, a critical titer is considered to be 16. In anti-K
HDFN, a critical titer is considered to be 8, and newer research suggests a titer of 4 should be used to target clinical monitoring.4 Since fetal anemia
can occur even with low titers, and the titer does not necessarily correlate to
the degree of anemia, fetal MCA-PSV measured by Doppler ultrasound is the
investigation of choice in the evaluation of anemia related to maternal K alloimmunization.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
The patient is a 54 year old woman, presenting to the
Emergency Room with complaints of abdominal cramps and feeling lethargic for
the past few days. She also reports her stools have been black and sticky. Her chart reveals a history of ulcers and GI
bleeding. She was transfused with 2
units packed RBCs 2 months ago for the same symptoms. CBC results are shown
below.
The patient was admitted to the hospital and four units of
blood were ordered. The patient is type A pos with a negative antibody screen.
One unit of packed red blood cells would be expected to raise the Hgb by 1g/dl.
Because the patient was actively bleeding, 4 units were crossmatched and
transfused.
Two days later, the patient was discharged, with orders to
follow up with her GI doctor for further testing and treatment. Three days
after discharge she still felt weak and returned to the ER. On examination, it
was noted that the patient’s eyes and skin appeared jaundiced. The patient had
a fever of 100F. Repeat lab results are shown below.
The Physician ordered a type and crossmatch for 2 units of
packed red blood cells. The patient’s antibody screen was now positive. A
transfusion reaction workup was initiated
Transfusion workup
Clerical Check- No clerical errors found.
Segments from all 4 transfused units were phenotyped for Jka
antigen. Three of the four units transfused typed as Jka positive.
A transfusion reaction is defined as any transfusion-related adverse event that occurs during or after transfusion of whole blood, or blood components. Transfusion reactions can be classified by time interval between the transfusion and reaction, as immune or non-immune, by presentation with fever or without fever, or as infectious or non-infectious.
A delayed
transfusion reaction is defined as one whose signs or symptoms typically present
days to several weeks after a transfusion. In Transfusion Medicine, we do not
want to give the patient an antigen that is not present on their red blood
cells. However, we do not routinely phenotype patients, so, in the patient with
a negative antibody screen and history, it is always possible that the patient
receives units with foreign antigens. The more immunogenic the antigen, and the
greater number units received that expose the patient to this antigen, the
greater likelihood that the patient will develop an antibody to the foreign
antigen. Therefore, this type of reaction would also be categorized as immune.
In a delayed hemolytic transfusion reaction (DHTR)
investigation, the units transfused would have appeared compatible at initial
testing. This type of adverse event is fairly common in patients who have been
immunized to a foreign antigen from previous transfusion or pregnancy. The antibody formed may fall to a very low level
and therefore not be detected during pretransfusion screening. If the patient
is subsequently transfused with another red cell unit that expresses the same
antigen, an anamnestic response may occur.
The antibody level rises quickly and leads to the DHTR. In the transfusion reaction workup,
this antibody can often be detected when testing is repeated. However,
in some cases, particularly with Kidd antibodies, the levels again drop off so
quickly they may not be detected! The diagnosis of DHTR is often difficult because
antibodies against the transfused RBCs are often undetectable and symptoms are
inconclusive.
This case is a classical example of a DHTR. Kidd antigens are notorious for causing DHT
because their levels can drop off quickly and disappear, making them difficult
to detect in screening. In this case, the transfusion two months earlier
exposed the patient to the Jka antigen and the patient produced the
corresponding antibody. The levels then dropped quickly, as elusive Kidds are
known to do! When the patient returned to the ER in crisis, the antibody levels
had dropped below detectable levels and the antibody screen was negative. The
patient was given 4 units and returned to the ER five days after transfusion. This
patient did exhibit mild jaundice and a low-grade fever. However, often, the
only symptom of a DHTR is the unexpected drop in Hgb and Hct, making them even
more difficult to diagnose.
The new antibody screen, sent to the Blood Bank on day 5, detected
anti-Jka. The DAT was positive mixed field due to the transfused cells. Elution
was performed and anti-Jka was recovered in the eluate. In the DHTR, only the
transfused cells are destroyed. Phenotyping segments from the transfused units
can estimate amount of transfused RBCs that may have shortened survival. Management
of this case patient would be to provide antigen negative units for all future
transfusions.
Kidd (Anti-Jka
and Anti-Jkb), Rh, Fy, and K have all been associated with DHTR and
occur in patients previously immunized to foreign antigens through pregnancy
and transfusion. These types of reactions are generally self-limiting but can
be life threatening, especially in multiply transfused patients, such as those
with sickle cell anemia. Antigen negative blood must always be given, even if
the current sample is not demonstrating the antibody in question. For that
reason, it is vitally important to always do a thorough Blood Bank history
check on all samples!
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
In the Iliad, Homer described the chimera as “a thing of immortal make, not human, lion-fronted and snake behind, a goat in the middle, and snorting out the breath of the terrible flame of bright fire (1).” This mythical creature has a lion’s head, a goat’s middle and the tail of a serpent, and the siting of a chimera was considered to be an omen for disaster! Thankfully, not so much in blood bank. Though ABO discrepancies can be a challenge, even most chimeras can easily be resolved with a few additional steps and a patient history.
Figure 1. The mythical chimera.
To review, an ABO discrepancy occurs when unexpected
reactions occur in the forward or reverse grouping, or the forward typing does
not match the reverse typing. Some weak subgroups of A (notably A3)
are known for giving mixed field reactions. Weak activity with anti-A, anti-B or
anti-D can also in result mixed field reactions in leukemia patients. In these examples,
the mixed field reactions are due to the weakened expression of the
corresponding antigens.
Chimerism is the presence of 2 cell populations in a single
individual. There are scenarios
where ABO discrepancies causing mixed field reactions indicate an apparent
chimera. A group A positive patient who received several units of O
negative blood will have mixed field reactions due to the presence of two blood
types in their peripheral blood. This would be a temporary situation. A patient
who received a bone marrow or stem cell transplant from a non-group identical
donor will have 2 populations of red blood cells until the new type is
established. We refer to these as artificial chimera cases, as the second blood
type is not naturally occurring, but present due to the introduction of a
different blood type via transfusion or transplantation.
Table 1. Group A pos patient who received several units of group O neg red cells
Like the
mythical beast, a chimera in biology describes an organism that has
cells from two or more zygotes. When chimerism exhibits only in the blood, the phenomenon
can be termed an artificial chimerism, as described above, as dispermic
chimerism or as twin chimerism. Dispermic chimerism occurs in other animal
species but is a rarity in humans. It occurs when 2 eggs are fertilized by 2
sperm and these products are fused into one body. In this case, the chimerism
is not limited to blood, but may also result in hermaphroditism, or two
different skin colors or eye colors.
Twin chimerism occurs when, in utero, one twin transfuses
blood cells, including stem cells, to
the other. Sine the fetal immune system is immature, the host does not see
these transfused blood cells as foreign antigens. The stem cells can proliferate and this
results in the production of cells from both the donor and the host for the
rest of the individual’s life. Two non-compatible blood groups can co-exist in
one individual! This phenomenon is usually discovered by coincidence during a
routine type and screen. This patient could be found to have mixed field or
weak reactions on ABO typing, or could have missing reactions in the back type,
all with no history of transfusion, transplantation and no disorder that could
explain the findings. What is a tech to do? An important step in resolving all
ABO discrepancies is to review patient history.
In 1953 a human chimera was reported in the British Medical Journal. A woman was found to have blood containing two different blood types. Apparently this resulted from her twin brother’s cells living in her body (2). More recently, in 2014, a case described in Blood Transfusion describes a 70 year old female who was found to have mixed field reactions with ABO and RhD typing during routine testing before surgery. She had no history of transfusion or transplantation, and a history of seven pregnancies. Repeat testing by other methods and with different reagents gave the same results. On further questioning, the patient affirmed that she had been born a twin, but her twin brother had died as an infant. Since chimerism was suspected, molecular typing and flow cytometry were performed. The presence of male DNA was found by PCR testing and flow cytometry confirmed two distinct populations of red blood cells (3).
Twin chimeras with mixed blood types of 50%/50% or 75%/25%
are easily picked up in ABO typing as mixed field reactions. A twin chimera with
95% group O blood and 5% group A may show a front type of a group O and a back
type that lacks anti-A . Because there is immune tolerance to A cells from the
twin, the expected naturally occurring anti-A is not present. On the other
hand, a twin chimera who is primarily group A with 5% O cells would not be
recognized as a chimera in routine ABO typing.
Table 2. Group O chimera with 5% minor cell population A cellsTable 3. Group A chimera with 5% O cells
How common is blood group chimerism? A 1996 study found that such blood group chimerism is not rare. Though we do not often encounter this in blood bank, their study of 600 twin pairs and 24 triplet pairs showed that this occurs more often than was originally thought, with a higher incidence in triplets than in twins. Because it does not cause any symptoms or medical issues, many such chimeras go undetected. In addition, the study found that many of these chimeras had very minor second populations, making them undetectable in serological testing. In blood bank, we generally test for ABO/RH and do not test for other antigens in routine testing. The study used 849 marker antigens. They also used a very sensitive fluorescent technique which they developed for detecting these very subtle minor populations. This study showed that while chimeras are not rare, they are something that, with present testing methods, we will not encounter too often (4).
Dual cell populations induced by chimeras have been the subject
of many studies. Historically, most chimeras were naturally occurring. With
newer medical interventions and therapies, we may see more situations that lead
to mixed cell populations. Transfusion, stem cell transplants, kidney
transplantation, IVF and artificial insemination can all lead to temporary and
sometimes permanent chimeras. These can present challenges in the blood bank
laboratory in interpreting results and for patient management. A question of
chimera presentation can usually be solved by putting on our detective hats and
investigating patient history. Further testing can be done with flow cytometry
and molecular methods, if needed. Modern medicine may have given us more blood
bank challenges but modern technology has equipped us with newer methods to
solve them. A chimera is no longer a sign of impending trouble!
References
Homer, Iliad. In Richmond Lattimore’s Translation.
Bowley, C. C.; Ann M. Hutchison; Joan S. Thompson; Ruth Sanger (July 11, 1953).“A human blood-group chimera” (PDF).British Medical Journal: 8
Sharpe, C.; Lane, D.; Cote J.; Hosseini-Maaf, B.; Goldman, M; Olsson, M.; Hull, A. (2014 Oct ). “Mixed Field reactions in ABO and Rh typing chimerism likely resulting from twin hematopoiesis”, Blood Transfusion:12(4): 608-610
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.