A 28 year old woman, gravida 1 para 0 presented to her OB/GYN for her first prenatal visit. A type and screen was ordered and the patient typed as A pos, with a positive antibody screen. Maternal history indicated that she had received several transfusions, for a total of 5 units of blood, following an automobile accident 15 months previously. An antibody identification was performed and Anti-K was identified in her plasma. The patient sample was phenotyped and was confirmed to be K negative.
Is the fetus at risk for Hemolytic Disease of the Fetus and Newborn (HDFN)? How can we know? And, if so, how should this pregnancy be monitored?
The answer to these questions is not a simple answer, and depends on several factors. Let’s look first at HDFN and its causes. HDFN is destruction of the RBC’s of the fetus and newborn by antibodies produced by the mother. This happens in 2 steps. The first step is that blood containing a foreign antigen enters the maternal blood stream and stimulates the mother to produce unexpected IgG antibody. But, how is a mother exposed to these foreign antigens? The mother is exposed either via a blood transfusion or a previous pregnancy. In this case, this was the mother’s first pregnancy, however her history revealed that she had been previously transfused. In order for the mother to produce anti-K , she must be K antigen negative, which was confirmed in the Blood Bank testing. She was exposed to the K antigen through transfusion and produced the anti-K antibody to the foreign antigen. The second step in the development of HDFN occurs when the mother’s antibody crosses the placenta and binds to this foreign antigen present on the red blood cells of the fetus. This can lead to RBC suppression, destruction, and fetal anemia.
Again, certain criteria must be met. First of all, the antibody must be IgG. Only IgG antibodies can cross the placenta. Active transport of IgG from mother to fetus begins in the second trimester and continues until birth. Secondly, the mother’s antibody is only of concern if the baby possesses the antigen that the mother lacks. Where does the baby get an antigen that is foreign to the Mom?? It’s the Dad’s Fault!! In HDFN, the mother lacks the antigen in question and the fetus possesses the antigen, which is of paternal origin.
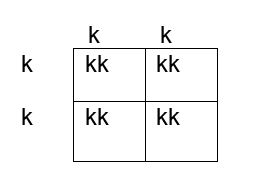
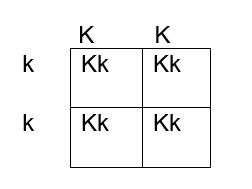
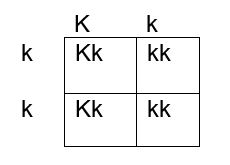
How do we determine if the fetus has the K antigen and is at risk? If you remember your genetics and Punnett squares, if the mother does not have the antigen and the baby does, the father must possess the antigen, because the baby gets an allele from each parent. This means that the fetus affected by HDFN is always heterozygous for the antigen in question. Figures 1, 2 and 3 below illustrate the possible inheritance patterns. In the first scenario, shown in Figure 1, the baby would not inherit a K antigen and would not be at risk for HDFN. In the Figure 2 scenario, the father is homozygous for K, and 100% of offspring from these parents would be K positive. Figure 3 illustrates a heterozygous father who would have a 50% chance of passing this gene to their offspring.
The father was phenotyped as K positive. The father’s blood sample was sent out for further zygosity testing, and he was found to be heterozygous for the K antigen. Thus, the fetus had a 50% chance of being affected by HDFN, and further testing was performed. The mother’s antibody titer was 1:4. To avoid an invasive procedure such as amniocentesis or chorionic villus sampling (CVS) which may worsen maternal alloimmunization, fetal DNA was isolated from the mother’s plasma at 12 weeks’ gestation and the fetal genotype was determined. The fetus was determined to be K positive and at risk for HDFN.
The mother’s titer and the fetus continued to be monitored. Diagnostic ultrasounds were performed to monitor fetal size, age, and structural changes. At 16-18 weeks’ gestation, ultrasounds of the middle cerebral artery (MCA-PSV) were performed to assess fetal anemia. MCV-PCA of 1.29 -1.5 multiples of mean (MoM) for the gestational age is indicative of mild anemia. Higher values predict moderate to severe anemia which require further intervention. At 18 weeks the MCV-PCA was 1.27 MoM and the fetus was determined to be developing normally.
A type and screen and antibody titer at 28 weeks showed the mother’s titer had increased, to 1:32, indicating that fetal RBCs with K antigen had entered the mother’s circulation and were stimulating further antibody production. Repeat MCV-PCA was 1.33, indicating mild anemia. Weekly measurements of MCA-PCV were recommended. At 32 weeks, a sudden increase was recorded, with MCV-PCA of 1.65 MoM. Cordocentesis was performed and fetal hemoglobin was 6.2g/dl. Fetal DAT was positive and anti K was identified in the eluate. An intrauterine transfusion (IUT) was performed. IUT was repeated at 34 and 36 weeks. The infant was delivered at 37weeks. The newborn required several neonatal transfusions while in the hospital and was discharged to home 3 weeks later.
Kell isoimmunization is the third most common cause of HDN after Rh and ABO and the most clinically significant of the non-Rh system antibodies in the ability to cause HDFN. It tends to occur in mothers who have had several blood transfusions in the past, but it may also occur in mothers who have been sensitized to the K antigen during previous pregnancies. Anti-K HDFN may cause rapidly developing severe fetal anemia. Anemia and hypoproteinemia are dangerous to the unborn child because they can lead to cardiac failure and edema, a condition known as hydrops fetalis. The MCA-PSV is a non-invasive doppler measurement of peak systolic velocity which is used to monitor fetal anemia. As mentioned previously, MCV-PCA of 1.29 -1.5 multiples of mean (MoM) is indicative of mild anemia. Values greater than 1.5 MoM are very sensitive and can be used to predict moderate to severe anemia that would need intervention.
HDFN due to anti-K differs from ABO and Rh HDFN in that, in HDFN due to K alloimmunization, Anti-K targets the RBC precursors. Remember that the K antigen can be detected on fetal RBCs as early as 10 weeks. The primary mechanism of K HDFN is due to maternal anti-K antibody actually suppressing the fetal production of RBCs, rather than hemolysis of mature fetal RBCS as seen in ABO and Rh HDFN. With reduced hemolysis, amniotic fluid bilirubin levels also do not correlate well with the degree of anemia. In addition, alloimmunization due to Anti-K differs in that even a relatively low maternal anti-K titer can cause erythropoietic suppression and severe anemia. In Rh HDFN, a critical titer is considered to be 16. In anti-K HDFN, a critical titer is considered to be 8, and newer research suggests a titer of 4 should be used to target clinical monitoring.4 Since fetal anemia can occur even with low titers, and the titer does not necessarily correlate to the degree of anemia, fetal MCA-PSV measured by Doppler ultrasound is the investigation of choice in the evaluation of anemia related to maternal K alloimmunization.

-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
