Case History
A 49 year old male presented to the emergency department (ED) with complaints of chest pain, shortness of breath, and chills for the past two weeks. He describes the pain as sharp and located on the left side of his chest. Past medical history is non-contributory, except for current IV drug use. His temperature was 97.7°F, blood pressure 141/63, heart rate 87, respirations 18 with an oxygen saturation of 91-93% on room air. On physical exam, a regular rate & rhythm with no murmur or regurgitation was noted and lungs showed fine bilateral crackles. His white blood cell count was increased at 22.1 TH/cm2 and troponin I was also elevated at 0.19 ng/ml. Blood cultures were collected and the patient was started on ceftaroline and piperacillin tazobactam for presumed infective endocarditis. He was transferred to the medical intensive care unit and intubated due to respiratory distress. An echocardiogram revealed a large mobile vegetation on the aortic valve with severe insufficiency and a vegetation & thickening of the mitral valve with severe regurgitation.
Laboratory Identification
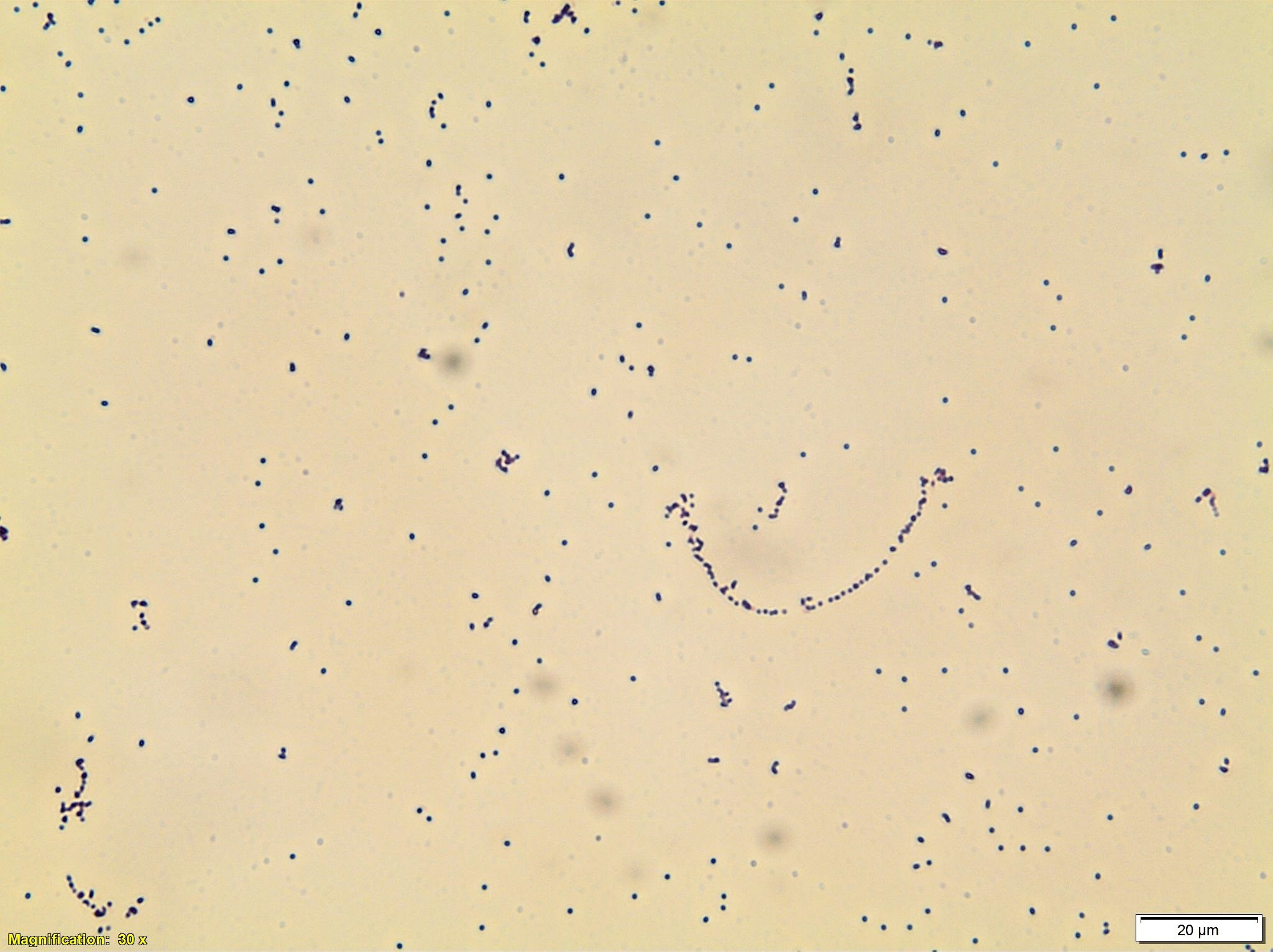

Blood cultures were positive within 24 hours of collection and gram positive cocci arranged in pairs and chains were noted (Image 1). Enterococcus spp., vancomycin resistance not detected was reported by polymerase chain reaction (PCR). Small, gray, non-hemolytic colonies grew after 2 days of incubation (Image 2). MALDI-TOF mass spectrometry identified the isolate as Enterococcus faecalis.
Discussion
Enterococcus spp. are gram positive, catalase negative cocci that are arranged in pairs & chains and are facultative anaerobes. Enterococcus spp. are widespread in nature and a component of the normal flora of the gastrointestinal tract and less commonly found in the oral cavity and on the skin. Commonly, Enterococcus spp. are opportunistic pathogens and cause infections of the urinary tract, intraabdominal cavity, surgical sites, bacteremia, and infective endocarditis.
In the microbiology laboratory, Enterococcus spp. grow readily on non-selective media and are usually alpha-hemolytic or non-hemolytic on blood agar. The two main species, E. faecalis and E. faecium, will grow in 6.5% NaCl, hydrolyze esculin in the presence of bile salts, and are positive for both leucine aminopeptidase (LAP) and L-pyrrolidonyl-beta-naphthylamide (PYR). Biochemically, arabinose utilization serves as a useful indicator to distinguish E. faecalis (negative) and E. faecium (positive). A variety of identification systems are able to identify the great majority of Enterococcus spp. to a species level.
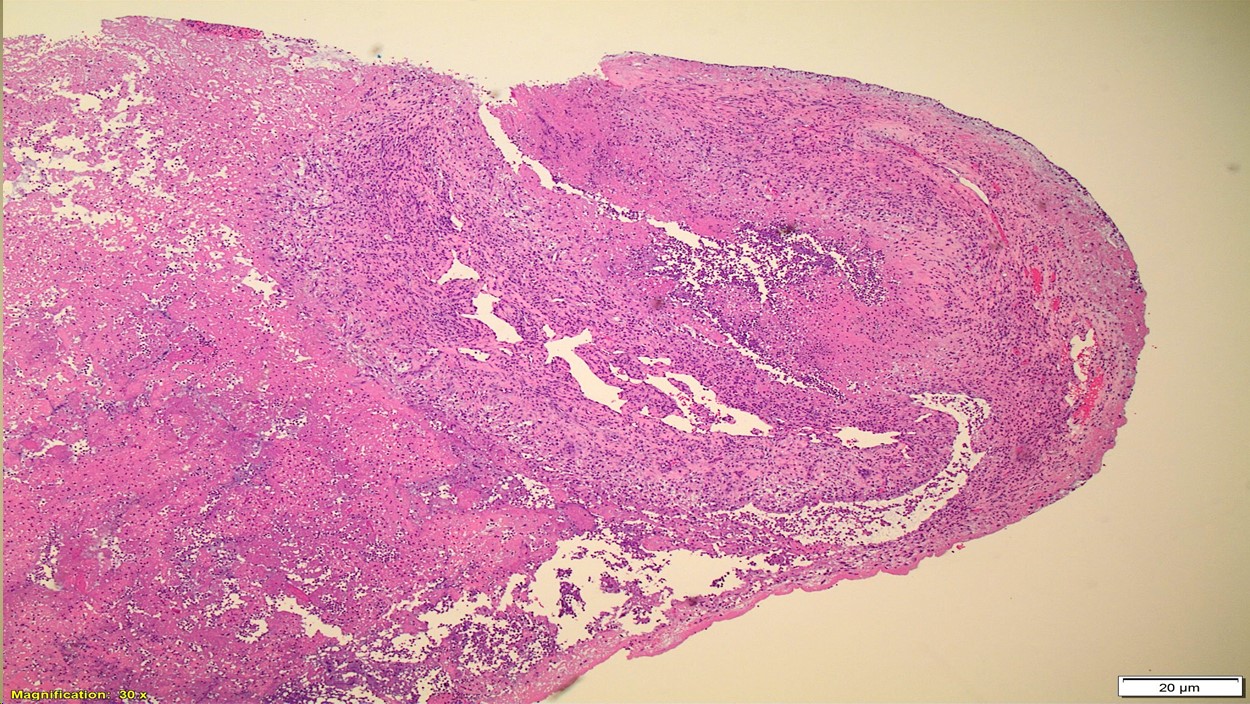
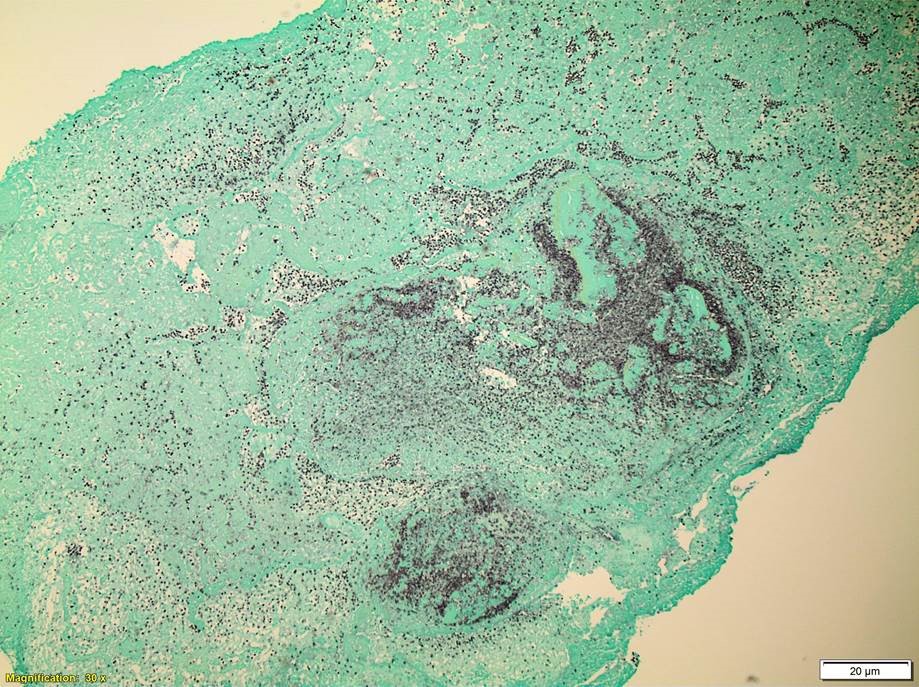
Ampicillin or vancomycin are acceptable treatment options for Enterococcal infections if found to be susceptible by antibiotic testing. It is important to note, Enterococcus spp. are intrinsically resistant to cephalosporins, aminoglycosides, trimethoprim-sulfamethoxazole, and clindamycin. For serious infections, including infective endocarditis, it is recommended to treat with a cell wall active agent such as ampicillin and an aminoglycoside (gentamicin or streptomycin) to create a synergistic bactericidal effect. Emergence of E. faecium acquired vancomycin resistance (VanA/VanB) is increasing and more board spectrum agents such as daptomycin and linezolid are necessary to effectively treat these infections. In the case of our patient, upon identification of E. faecalis from multiple blood cultures, his antibiotics were switched to IV ampicillin and gentamicin. He underwent valve replacement surgery and both the aortic and mitral valves grew E.faecalis as well and showed numerous bacterial cocci on histology (Images 3 & 4). He completed a six week course of ampicillin and gentamicin and was discharged home in good condition.

-Hansini Laharwani, MD is a first year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
