Over on her blog, Maryn McKenna discusses the latest emerging microscopic threat: drug-resistant fungal infections. It mentions the organism Candida auris and states: “The Centers for Disease Control and Prevention (CDC) is so concerned that it recently sent an alert to U.S. hospitals, even though only one possible case of the resistant fungus has been identified in the United States so far.”
“The U.S. Food and Drug Administration today cleared for marketing the Xpert Carba-R Assay, an infection control aid that tests patient specimens to detect specific genetic markers associated with bacteria that are resistant to Carbapenem antibiotics.”
A 42 year old woman presented to her primary care physician after noticing a slightly tender lump in her left breast. After an inconclusive mammogram, the mass was biopsied, revealing no malignancy, but acute and chronic inflammatory changes with granulation tissue. Acid fast bacilli and Gomori’s methenamine silver stains were negative for organisms on this biopsy. The mass continued to enlarge over this time, and the overlying skin became erythematous with no active drainage. She underwent needle aspiration of the mass and the fluid obtained was sent for routine culture.
Laboratory Identification:
Colonies grown on routine culture were gram stained, and the smear revealed beaded gram-positive bacilli. Acid-fast and modified acid-fast stains were performed, revealing a partially acid fast organism. The culture was sent out for identification and susceptibilities, which came back as Gordonia bronchialis. It was susceptible to all drugs tested (amoxicillin/clavulanate, cefepime, ceftriaxone, imipenem, ciprofloxacin, moxifloxacin, amikacin, tobramycin, doxycycline, minocycline, TMP/SMX, linezolid) with the exception of an intermediate susceptibility result for clarithromycin.
Gordonia bronchialis is an aerobic, gram positive, partially acid fast, branching, filamentous bacteria that can fragment into rods and cocci. On agar, the colonies can be somewhat pigmented, dry, and raised. It is an uncommon pathogen, and is acquired from environmental sources such as soil, farm animals, and water.
Most infections occur in immunocompromised hosts, often in association with intravascular catheters. Gordonia bronchialis has been reported to cause osteomyelitis, bacteremia, pleural infection, intraventricular shunt infection, and sternal wound infection. One case series of seven patients in a single hospital contracting sternal wound infections with G. bronchialis traced these infections back to a nurse anesthetist. One case report was found in the literature of a recurrent breast abscess caused by Gordonia bronchialis, which required months of doxycycline therapy as well as repeated incision and drainage procedures.
It is unclear how the patient in this case acquired the organism; a thorough infectious disease work-up revealed no signs of immunocompromise, and she had no history of trauma or surgery to the area. Of note, she did have acupuncture performed on her shoulder several months prior to presentation, but no acupuncture was performed in the region of the abscess.
Gordonia bronchialis tends to be widely susceptible to antibiotics; however, treatment failures are frequent. It is believed that the tendency of the organism to form sessile colonies explains these failures.
The patient in this case is currently being treated with Bactrim and Augmentin. Her abscess was re-aspirated several weeks after initiation of therapy when it continued to enlarge, and the second culture is once again growing Gordonia bronchialis. The abscess seems to be improving since this second aspiration, so the treatment team currently plans to continue with oral antibiotics and forego a further incision and drainage procedure.
References:
Richet HM, et al. A cluster of Rhodococcus (Gordona) bronchialis sternal-wound infections after coronary-artery bypass surgery. N Engl J Med 1991;324:104–109.
Siqqiqui N et al. Tibial osteomyelitis caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2012;50(9):3119-21.
Werno AM et al. Recurrent breast abscess caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2005;43(6):3009-10.
-Laurie Griesinger is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Recent studies conducted by Brazilian researchers found “super bacteria” in the waters where Olympic athletes will be competing. According to MercoPress, “The Brazilian group’s lead researcher, Renata Picao, said Rio’s “super bacteria” made its way into the city’s waterways through sewage from local hospitals, due to a lack of basic sanitation in the metropolitan area.”
Maryn McKenna writes extensively about antimicrobial resistance. You can watch to her recent TED talk (or read the transcript) to learn why the presence of CRE in Rio’s water is so concerning.
A 2-year-old male with no past medical history presented to the emergency department with fever and 2 days of bloody diarrhea. Stool cultures were sent to the laboratory. A Gram stain of the specimen showed the morphology seen in Figure 1. On the 5% sheep blood agar plate, the predominant organism had colonies that appeared flattened and spreading (Figure 2A). On MacConkey agar the colonies were noted to be non-lactose fermenting (Figure 2B). A Hektoen enteric (HE) agar was used as a differential and selective media to differentiate Salmonella from Shigella. On the HE agar the colonies were clear with a green appearance due to the color of the agar (Figure 2C).
Gram stain showing Gram-negative rodsIsolate growing on (A) 5% sheep blood, (B) MacConkey, and (C) Hectoen Enteric agars
Identification
Shigella is a bacterium in the Enterobacteriaceae family and is a Gram-negative rod that is facultatively anaerobic. It is non-motile, a non-spore former, and does not ferment lactose. There are four species of Shigella that are associated with subgroups A-D. Our isolate was identified as Shigella sonnei, which is the most common species in the U.S. and comprises subgroup D. The other subgroup/species correlations are listed in Table 1. The slide agglutination antisera test is used to aid in serogrouping. The suspected colony is mixed on a slide with antisera that contains specific antibodies to Shigella. If clumping (agglutination) occurs, it is considered a positive result for the specific subgroup. The organism was identified as Shigella sonnei by slide agglutination antisera testing. In addition, Shigella has certain biochemical properties that aid in further identification and confirmation.
Table 1: Shigella sp. determination by serogroup
Serogroup
Organism
A
Shigella dysenteriae
B
Shigella flexneri
C
Shigella boydii
D
Shigella sonnei
Clinical Significance
Shigella is one of the most common causes of bacterial gastroenteritis and is often associated with poor sanitation and overcrowded conditions. Transmission occurs through routes such as: fecal-oral and person to person contact. Of note, only a small amount of the bacteria (as low as 10 organisms) is required to cause disease. Hemolytic-uremic syndrome is a complication that may occur with shiga-toxin producing Shigella (the most commonly associated is S. dysenteriae). Shigella has demonstrated antibiotic resistance and therefore does undergo susceptibility testing.
References:
Nataro JP, Bopp CA, Fields, PI, Kaper JB, Strockbine, NA. 2015. Escherichia, Shigella, and Salmonella, p 603-626. In Jorgensen J, Pfaller M, Carroll K, Funke G, Landry M, Richter S, Warnock D (ed), Manual of Clinical Microbiology, Eleventh Edition. ASM Press, Washington, DC.
-Valerie Juarez, M.D., 3rd year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
A 72 year old man had been complaining of many months of constipation followed by several months of severe diarrhea prior to admission. He did not receive medical care for these symptoms and had no medical history on file. He presented to an outside hospital unresponsive, and an emergent CT showed subcutaneous emphysema and stranding of the lower abdominal tissue extending to the left hemiscrotum. Also noted was irregular wall thickening in the distal rectum. Of note, his family reported that the patient had hit his left scrotum with a power cord recoil a few days prior to presentation. He was transferred to our hospital, where the surgical team reported severe cellulitis and necrosis of the scrotum, perineum, anterior abdominal wall, and upper thighs. Due to his poor prognosis, the family decided to transition his care to comfort measures only and he passed away several hours after presentation. An autopsy was performed, which revealed liquefaction of the subcutaneous tissue in the lower anterior abdominal wall, dusky gray connective tissue of the left testis as well as a small abscess at the superior pole, and a circumferential distal rectal mass.
Laboratory Investigation:
A gram stain of the scrotal abscess and tissue of the anterior abdominal wall both showed mixed gram positive and gram negative organisms. Cultures of these specimens both grew mixed gram positives including alpha hemolytic Streptococcus and coagulase negative Staphylococcus, as well as mixed anaerobes including Bacteroides fragilis group.
Gram stain of the scrotal abscess showing mixed gram negative and gram positive organisms.Histologic section of anterior abdominal wall (400X) showing many polys and many bacterial organisms.Chocolate agar plate showing mixed growth.
Discussion:
The case above represents an example of Fournier’s gangrene, a necrotizing infection of the external genitalia and/or perineum. These infections are most often polymicrobial and often include organisms that would not be particularly aggressive by themselves, suggesting a synergy between anaerobic and aerobic organisms. In a large literature review of over 4,000 cases of Fournier’s gangrene, the most common pathogens involved were Escherichia coli, Streptococcus, Bacteroides, Enterobacter, and Staphylococcus. Our case fits well with this profile, consisting of a mixture of gram positives and gram negatives including Streptococcus, Staphylococcus, and Bacteroides fragilis group. Antibiotic coverage in these cases must be broad spectrum and include coverage for aerobes, anaerobes, gram negative and gram positive organisms.
Risk factors for Fournier’s gangrene include diabetes mellitus, smoking, alcoholism, renal failure, hypertension, and coronary artery disease. It is unclear whether the patient in this case had any of these risk factors as he did not routinely seek medical care.
The rectal mass in this case proved to be adenocarcinoma. There have been multiple case reports of Fournier’s gangrene in association with rectal cancer. The theory behind the mechanism of this association is that perforation of the rectal cancer occurs with tumor infiltration of surrounding tissues spreading infectious organisms. It is possible that our case was caused by the patient’s rectal cancer, but it is also possible that the rectal cancer was simply coincidental. The recent trauma to the patient’s scrotum could also have acted as a vector for infection.
The patient in our case presented too late in the course of his disease to receive appropriate treatment, which would consist of broad spectrum antibiotic administration and aggressive debridement. Even with such treatment, the mortality rate of Fournier’s gangrene is quite high, ranging from 5% to 40% in different case series.
References:
Bjurlin MA et al. Causative pathogens, antibiotic sensitivity, resistance patterns, and severity in a contemporary series of Fournier’s gangrene. Urology 2013;81(4):752-8.
Bruketa T et al. Rectal cancer and Fournier’s gangrene – current knowledge and therapeutic options. World J Gastroenterol 2015;21(30):9002-9020.
-Laurie Griesinger is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 44 year old woman presented to an outside hospital with a chief complaint of abdominal tenderness and increased abdominal girth over the past few days. Her past medical history was significant for type II diabetes mellitus and associated complications including retinopathy and chronic kidney disease. As a result of her renal failure, she was currently undergoing peritoneal dialysis. Due to concern for infectious peritonitis, a paracentesis was performed and the resulting fluid obtained was sent to the Microbiology laboratory for Gram stain and bacterial culture. Because of difficulty in identifying the isolate, it was sent to our mycology section for further work up.
Laboratory Identification
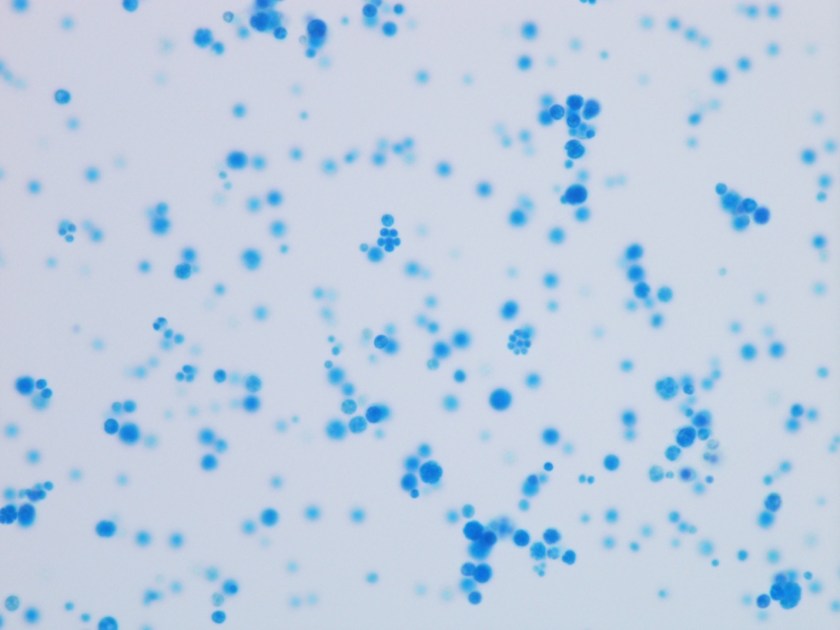
Figure 1. Many sporangia of various sizes containing endospores arranged in a “soccerball” like pattern or morula configuration (Lactophenol cotton blue prep, 400x).
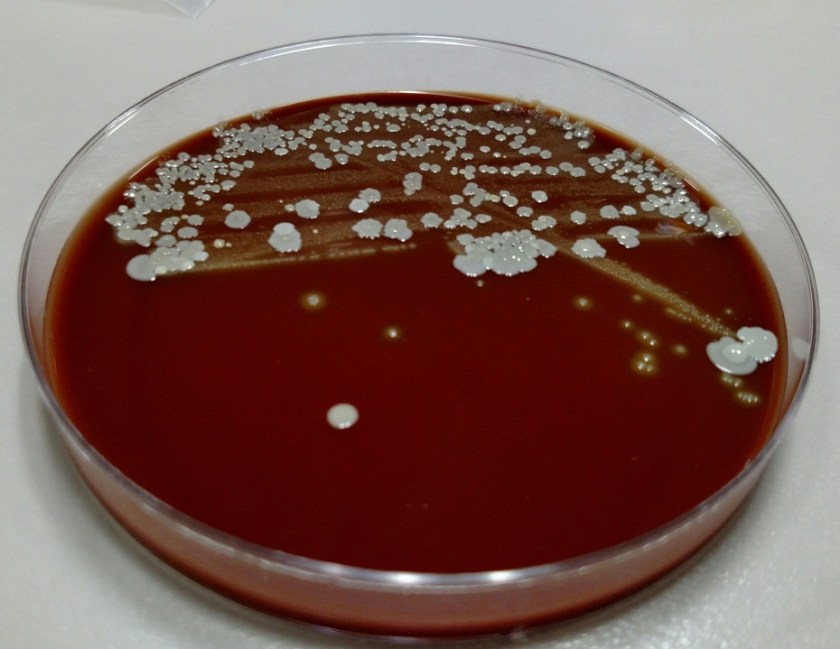
The isolate was received on potato dextrose agar (PDA) and appeared as discrete cream colored colonies, resembling a yeast. Upon transfer to cornmeal agar and incubation at 30°C, the isolate grew rapidly over the course of two days. The organism did not grow on media containing cycloheximide. A lactophenol cotton blue prep was performed (Figure 1) and showed many sporangia, ranging in size from 4-15 µm. In the larger forms, individual endospores were able to visualized and they were arranged in a “soccerball” like pattern. No budding or hyphae were present. Given these characteristics, the organism was identified as Prototheca wickerhammii.
Discussion
Prototheca wickerhammii is classified as an achlorophyllous algae and is known to cause human infections involving the skin and subcutaneous tissues, bursa of the elbow joint (olecranon bursitis) and rarely, systemic infections. P. wickerhammii is ubiquitous in nature and infection is usually the result from traumatic inoculation. Both immunocompetent and immunocompromised hosts can be affected, although more severe or systemic disease occurs in those who have defects in cell mediated immunity.
Prototheca spp. grow rapidly on PDA after incubation at 30°C for 2-3 days. Initially, it may be confused with a yeast based on plate morphology as they are cream colored and have a yeast-like consistency. When a lactophenol cotton blue prep is viewed under the microscope, sporangia of various sizes are identified (3-30 µm) that contain endospores arranged in a “soccerball” or symmetric daisy like pattern. Size of the sporangia, assimilation tests (such as the API 20C) and automated yeast identification systems (such as the Vitek yeast ID by bioMérieux) are helpful in identifying Prototheca to a species level. Both P. wickerhammii (4-11 µm in diameter) and P. zopfii (9-28 µm in diameter) can cause disease in humans, but P. wickerhammii is more common. While P. wickerhammii has symmetric internal divisions as seen in the above image, P. zopfii has random internal divisions.
The treatment of P. wickerhammii usually includes a combination of surgical management and anti-fungals depending on the site of involvement. For superficial skin infections, localized excision and the use of topical or systemic anti-fungals (azoles and amphotericin B) has been shown to have success. The treatment for olecranon bursitis focuses on bursectomy. In the case of systemic infections, amphotericin B has been the most successful treatment modality. Susceptibility testing is not routinely recommended to guide treatment of initial infections, as studies are few and results don’t always correlate with outcome.
Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
A previously healthy 30 year old man presents with a painful right eye. Three weeks before he had been cutting concrete with an electric saw when a piece of hard concrete hit him in the eye. The eye became painful the following day. He was treated with empiric antibiotics but the eye pain failed to improve. He was eventually seen by ophthalmology, where ophthalmologic exam demonstrated findings suspicious for fungal keratitis. Corneal scraping was performed and sent for bacterial and fungal culture.
Laboratory Identification:
Bacterial culture showed no growth. Fungal culture demonstrated rapid growth of multiple white, cottony molds on potato flake agar. Over time these white colonies turned dark grey/brown. The reverse surface of the agar was white at first but also turned dark grey/brown over time.
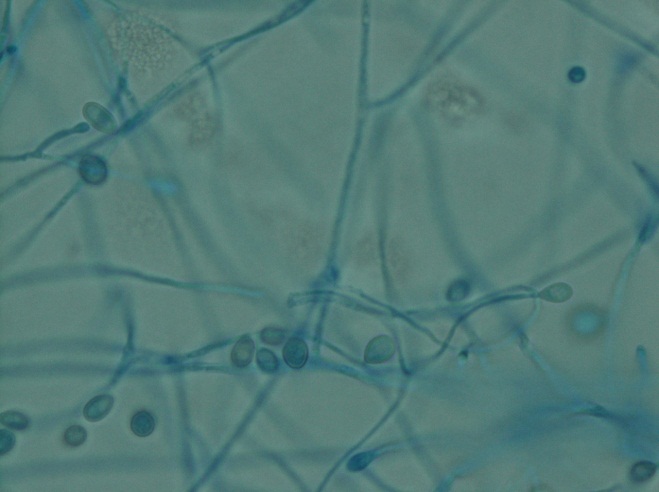
Microscopically (scotch tape preparation), there were thin hyphae with single conidia arising directly off the tips of tapered conidiophores of variable length. Occasional conidia were also observed arising directly off of the sides of hyphae. The conidia were small and oval in shape with a truncated base, and somewhat darker as compared to the surrounding hyphae. Sexual forms were not observed.
Potato flake agar showing a white, cottony mold with a central dark gray/brown coloration.
Scotch tape preparation demonstrating thin hyphae with single oval-shaped conidia with truncated base. The conidia are small and have a “sperm-like” or “tadpole-like” morphology.
Discussion:
The clinical history and laboratory findings are characteristic of Pseudallescheria boydii/Scedosporium apiospermum.
Pseudallescheria boydii/Scedosporium apiospermum is an environmental mold which can be isolated from rural soils, polluted waters, manure and compost. Infection occurs secondary to local trauma. In immunocompetent individuals, infection is limited to the site of trauma, with some of the more common presentations being fungal keratitis, endophthalmitis, eumycotic mycetoma, sinusitis and pneumonia in the setting of near drowning. In immunocompromised individuals, infection can disseminate and involve any organ.
Pseudallescheria boydii/Scedosporium apiospermum is the most common cause of eumycotic mycetoma. Mycetoma is a chronic granulomatous infection of the subcutaneous tissue, usually involving the distal lower extremities, which can be caused by either a fungus (eumycotic mycetoma) or an actinomyces species bacteria (actinic mycetoma). On clinical exam there are multiple draining sinus tracts. The causative microorganisms aggregate into macroscopically visible groups (“granules”) which can be white, yellow or brown in color. Mycetoma may progress over time to involve underlying soft tissue, muscle, fascia and bone. Other less common causes of eumycotic mycetoma include Madurella spp., Acremonium spp., Fusarium spp., and Curvularia spp.
This organism has two names because historically different names were assigned to the sexual state (Pseudallescheria boydii) and to the asexual state (Scedosporium apiospermum). Morphologically, Pseudallescheria and Scedosporium are identical, the only difference being the presence of the sexual form, cleistothecia, in Pseudallescheria. Cleistothecia, when present, can be recognized as very large, dark-brown asci containing numerous ascospores. Technically, in the absence of cleistothecia the correct diagnosis would be Scedosporium boydii, however in clinical practice both names are usually listed regardless of whether cleistothecia are seen.
Pseudallescheria boydii/Scedosporium apiospermum is resistant to amphotericin B, but should be susceptible to azole therapy. The patient is being treated with topical voriconazole and oral fluconazole and currently (two weeks of antifungal therapy) has near complete resolution of symptomatology.
-Javier De Luca-Johnson, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
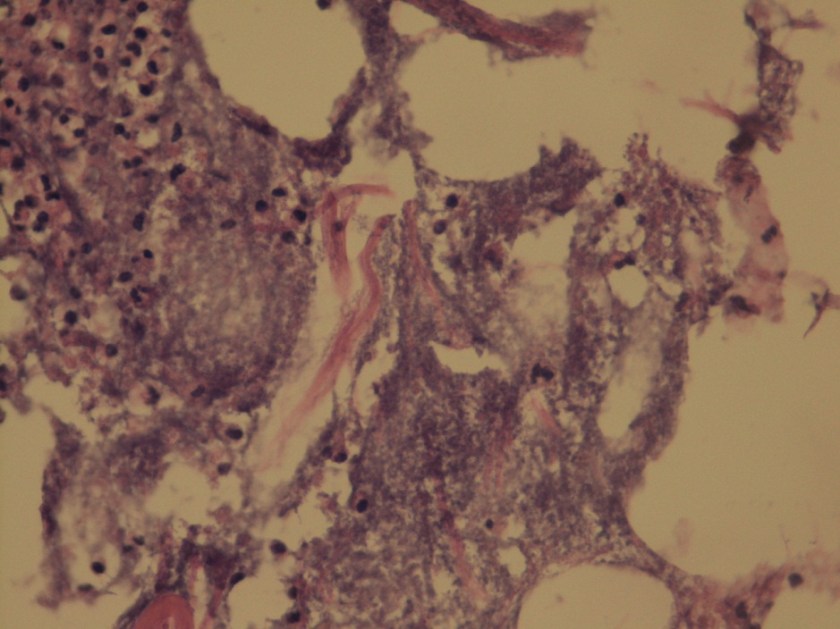
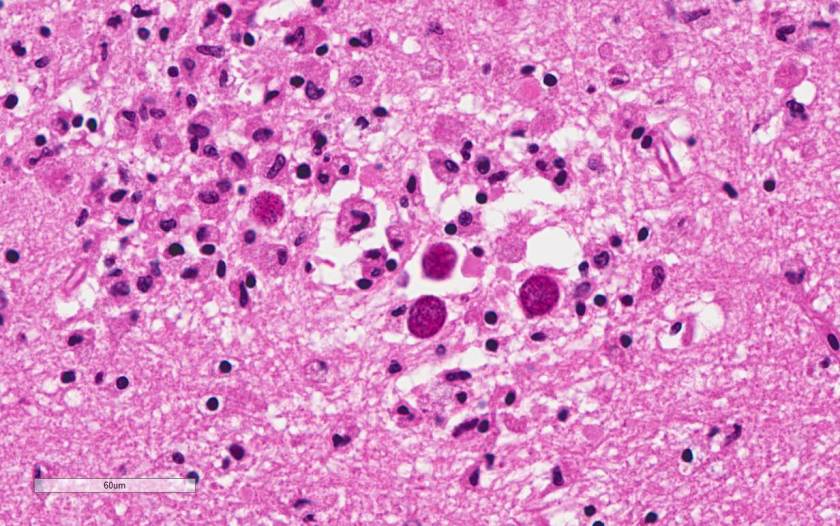
A 47-year old woman with a past medical history of Systemic Lupus Erythematosus (SLE) and liver cirrhosis of unknown etiology was admitted to the hospital for back pain and new onset neurological symptoms. She soon developed pancytopenia and study of her peripheral blood smear showed evidence of thrombotic microangiopathy. ADAMTS-13 inhibitor was negative ruling out thrombotic thrombocytopenic purpura (TTP). She then developed multiple thrombi, including a nonocclusive thrombus in the superior mesenteric vein with extension to the splenic vein as well as a femoral deep vein thrombosis. Her hospital course then became complicated by lupus cerebritis, a small ischemic focus in the left corona radiata and the left medial midbrain, and decompensated liver failure with hepatic encephalopathy. Despite intensive medical treatment, she became hypoxic and hypotensive requiring pressors, and expired in the ICU after several months of hospitalization. The autopsy was performed based on the relative’s request to better understand pathological processes that lead to patient’s demise. The flowing images were obtained from the brain at autopsy (Image 1).
Light microscopy of H&E-stained sections of the hippocampus reveal encysted Toxoplasma bradyzoites as well as extracellular Toxoplasma tachyzoites in the CA1 region, suggestive of a subacute focal infection.
Discussion
Toxoplasmosis is considered to be a leading cause of death attributed to foodborne illness in the United States. More than 60 million men, women, and children in the U.S. carry the Toxoplasma parasite, but very few have symptoms because the immune system usually keeps the parasite from causing illness.
People typically become infected with Toxoplasma by contaminated food or animal-to human routes of transmission. Toxoplasmosis is not passed from person-to-person, except in instances of mother-to-child (congenital) transmission and blood transfusion or organ transplantation.
Persons with compromised immune systems may experience severe symptoms if they are infected with Toxoplasma while immune suppressed. Persons who acquire HIV infection and were not infected previously with Toxoplasma are more likely to develop a severe primary infection. The diagnosis of toxoplasmosis is typically made by serologic testing. A test that measures immunoglobulin G (IgG) is used to determine if a person has been infected. If it is necessary to try to estimate the time of infection, which is of particular importance for pregnant women, a test which measures immunoglobulin M (IgM) is also used along with other tests such as an avidity test. Due to the high rate of falsely positive Toxoplasma IgM testing, the FDA advises physicians testing pregnant women not to rely on the results of any one positive IgM test as the sole determinant for diagnosis of acute Toxoplasma infection.
Diagnosis can be made by direct observation of the parasite in stained tissue sections, cerebrospinal fluid (CSF), or other biopsy material. These techniques are used less frequently because of the difficulty of obtaining these specimens. Molecular techniques that can detect the parasite’s DNA in the amniotic fluid can be useful in cases of possible congenital transmission.
Clinical correlation
The case patient was at risk for developing toxoplasmosis due to SLE disease, and chronic immunosuppressive therapy that she was receiving for the aggressive course of her illness. However, most likely Toxoplasma gondii organisms seen in the brain parenchyma were in a dormant state due to lack of associated inflammation or architectural distortion. Her neurological decline is most likely related to thrombotic microangiopathy. Opportunistic infection is common in patients with SLE. In some patients, it is difficult to distinguish between the effect of infection and exacerbation of SLE because both can produce similar symptoms. There have been many reports of toxoplasmosis in SLE patients, with conditions such as cerebritis and pericarditis mimicking SLE manifestations.
2) Seta N, Shimizu T, Nawata M et al. A possible novel mechanism of opportunistic infection in systemic lupus erythematosus, based on a case of toxoplasmic encephalopathy. Rheumatology (Oxford). 2002;41(9):1072-3.
3) Zamir D, Amar M et al. Toxoplasma infection in systemic lupus erythematosus mimicking lupus cerebritis. Mayo Clin Proc. 1999; 74(6):575-8.
Contributors
Written by Anastasia Drobysheva, MD, 2nd year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
Image provided by Bret Evers, MD, PhD, Neuropathology fellow,UT Southwestern Medical Center
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
A 59 year old woman with systemic sclerosis and history of lung transplant with chronic allograft rejection presented to the hospital for progressive dysphagia and acute kidney injury necessitating dialysis. She continued her home drug regimen: immunosuppressives such as prednisone, tacrolimus, and mycophenolate as well as antibiotic prophylaxis consisting of itraconazole, trimethoprim-sulfamethoxazole, and azithromycin. Six days later she began to experience increased sputum production with a cough and shortness of breath. Repeat chest x-ray showed persistent bilateral pleural effusions and lower lobe opacities consistent with a chronic inflammatory process but could also represent infection. A sputum culture was obtained and she was started on a course of levofloxacin.
Laboratory identification:
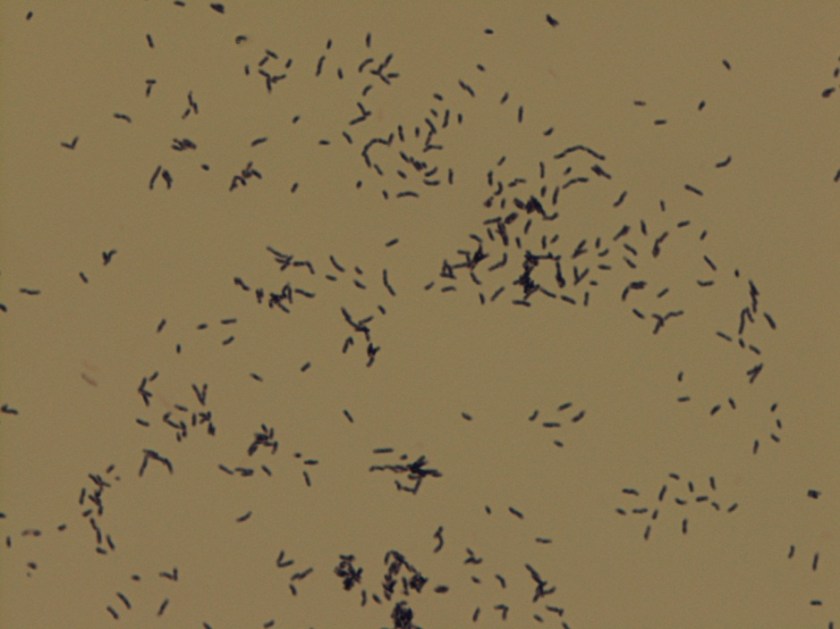
Gram stain of the sputum revealed moderate PMNS with abundant gram positive bacilli that appeared coryneform. The organism grew well on blood and chocolate agar, presenting as non-hemolytic white-gray moist smooth colonies.
Gram stain revealing numerous Gram-positive bacilli, some in pairs with characteristic “V” formation seen in coryneform bacteriaCreamy, white-to-gray colonies on blood agar
MALDI-TOF revealed Corynebacterium striatum.
Discussion:
Until the past fifteen to twenty years it was believed that Corynebacterium striatum and many other non-toxigenic species of the Corynebacterium genus were almost always avirulent. C. striatum is typical of human skin and nasopharyngeal flora and most coryneform species were largely ignored with the exceptions of the toxigenic strains such as C. diphtheriae, C. ulcerans and C. pseudotuberculosis. However, the incidence of serious C. striatum infections has been rising and is attributed to the prolonged survival of patients in immunocompromised states, patients with chronic lung disease such as COPD and cystic fibrosis, and the increasing use of indwelling medical devices such as infusion ports, dialysis catheters, and joint prostheses. More and more cases of endocarditis and respiratory infections have been attributed to C. striatum and with repeated and prolonged hospital stays; frequent patient exposure to broad-spectrum antibiotics create ample opportunity for C. striatum to cause outbreaks of nosocomial infections.
However, there is still little evidence to suggest how C. striatum is actually transmitted and how it can adapt. It is left to the microbiology lab to decide whether its presence in culture represents an actual infection and coryneform bacteria are difficult to speciate on the basis of biochemical testing alone. Most importantly, a culture from a true C. striatum infection should grow out pure or predominant colonies. They are aerobic Gram positive bacilli related to Mycobacteria and Nocardia with a characteristic appearance on Gram stain: often pleomorphic, slightly curved with clubbed or tapered ends, and cells may occur singly or in pairs in what is often dubbed “Chinese letter” formation. Toxigenic forms of Corynebacterium are catalase positive (as is C. striatum) but many species are catalase negative. Unlike the toxigenic species, C. striatum is pyrazinamidase positive. Urease and nitrate are also useful but many species overlap in their biochemical testing characteristics and in order to truly name the species it is recommended that MALDI-TOF mass spectrometry be used which has been shown in several studies to be an accurate test for coryneform species identification.
-Dwight Parker is a 4th year medical student at the University of Vermont College of Medicine.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.