“The U.S. Food and Drug Administration today cleared for marketing the Xpert Carba-R Assay, an infection control aid that tests patient specimens to detect specific genetic markers associated with bacteria that are resistant to Carbapenem antibiotics.”
Have you ever felt like no one knows exactly what you do for a job; friends, family, even your colleagues? As a clinical pathologist, if you are ever asked what your job entails, it might take you a full 10 minutes to just explain the surface of it and by that time your audiences’ s eyes have glazed over and they are wondering when their next coffee break is. It can get pretty lonely when very few people understand your daily life of work.
I currently hold a general clinical pathology position and oversee the microbiology, chemistry, and immunology sections of a community hospital laboratory that services two hospitals totaling a little over 500 beds. I also get consulted on point of care testing and consult at two critical access hospitals that have a general AP/CP pathologist directing their lab.
As a new clinical pathologist, I was asked to blog about my experiences during the first year of working in the real world. I thought it would be a great venue to talk about how I have combatted the “loneliness” I face when I feel like no one knows what I do. Over the next couple of months I will highlight some of the tasks I have undertaken in my current position and I’d also love to hear what other clinical pathologist’s careers look like and/or how they have evolved over the years.
The beauty of a career in clinical pathology was explained to me by an attending during my residency training –you make of it what you want to. He also told me to not venture into the lab because they will ask you to do things, and since I am not very good at following advice, that is exactly the first topic I would like to explore: getting into the lab on a daily basis.
When I was in training, one of the best ideas I took away for my job was microbiology rounds. The first attending I observed holding these was a medical microbiologist that would round through the micro lab every day asking the techs if they had any odd cultures, questions that needed to be answered or anything that required follow up. When I took this job, I knew I wanted to incorporate this type of rounding as part of my work. My office is conveniently located at the back of the microbiology laboratory, so as I walk through the lab, I make it a point to say hi and ask the technologists if they have any issues, or any interesting cultures. It is not a formal rounding, but issues come out of these interactions and give me items to follow up with on a daily basis. Having my office located in the lab also allows the techs to come to me throughout the day with any questions they may have and has established a great rapport between us.
I also round through the chemistry and immunology section of the lab, specifically hitting second shift, as they lack a lot of interaction with clinicians. This has been a harder task for me because my subspecialty training was microbiology. I feel comfortable interacting with the technologists and lab staff, but when I first started I had the fear that I would not know the answer to a question I might be asked. Lucky for me, there are not as many questions that come out of these rounds. But of the questions I have gotten and I did not know the answer, it has never been a problem by me saying “I don’t know off the top of my head, but let me get back to you”. It also helps that I drop off candy in the break room while they wait on me – it is truly amazing how chocolate helps you make friends (thanks for the tip, Mindy Kaling). In addition to troubleshooting, rounding through the lab has given me the opportunity to interact with other people who have a passion for laboratory medicine. The techs will get just as excited about an interesting organism that was isolated or a new instrument we might bring in, and it is great to be able to share that passion you feel for your job with others.
Next month I will discuss a little more about the “formal” interactions I have set in the lab, but for now, let’s hear from you: how do you get involved in the lab and the technologists you work with?
-Lori Racsa, DO, is the director of microbiology, immunology, and chemistry at Unity Point Health Methodist, and a Clinical Assistant Professor at the University Of Illinois College Of Medicine at Peoria. While microbiology is her passion, has a keen interest in getting the laboratory involved as a key component of an interdisciplinary patient care team.
A 42 year old woman presented to her primary care physician after noticing a slightly tender lump in her left breast. After an inconclusive mammogram, the mass was biopsied, revealing no malignancy, but acute and chronic inflammatory changes with granulation tissue. Acid fast bacilli and Gomori’s methenamine silver stains were negative for organisms on this biopsy. The mass continued to enlarge over this time, and the overlying skin became erythematous with no active drainage. She underwent needle aspiration of the mass and the fluid obtained was sent for routine culture.
Laboratory Identification:
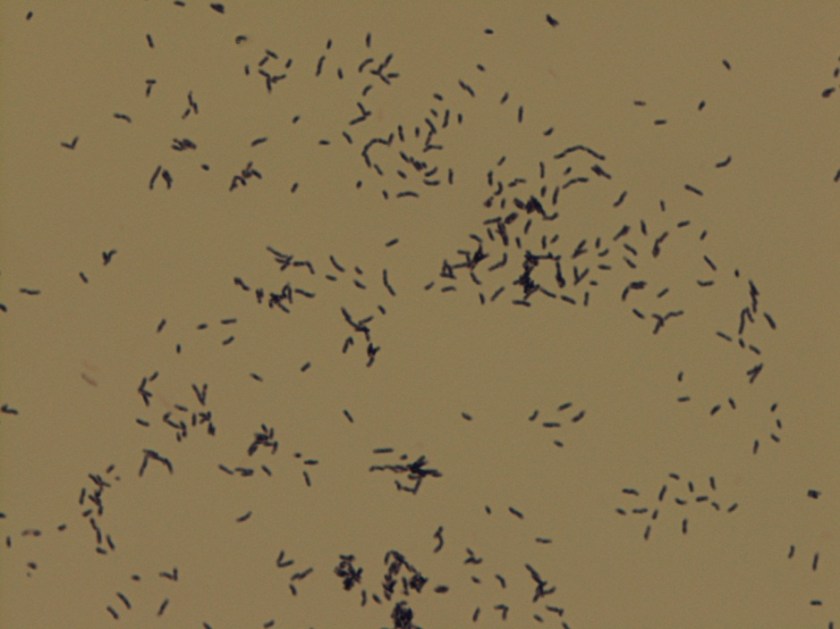
Colonies grown on routine culture were gram stained, and the smear revealed beaded gram-positive bacilli. Acid-fast and modified acid-fast stains were performed, revealing a partially acid fast organism. The culture was sent out for identification and susceptibilities, which came back as Gordonia bronchialis. It was susceptible to all drugs tested (amoxicillin/clavulanate, cefepime, ceftriaxone, imipenem, ciprofloxacin, moxifloxacin, amikacin, tobramycin, doxycycline, minocycline, TMP/SMX, linezolid) with the exception of an intermediate susceptibility result for clarithromycin.
Gordonia bronchialis is an aerobic, gram positive, partially acid fast, branching, filamentous bacteria that can fragment into rods and cocci. On agar, the colonies can be somewhat pigmented, dry, and raised. It is an uncommon pathogen, and is acquired from environmental sources such as soil, farm animals, and water.
Most infections occur in immunocompromised hosts, often in association with intravascular catheters. Gordonia bronchialis has been reported to cause osteomyelitis, bacteremia, pleural infection, intraventricular shunt infection, and sternal wound infection. One case series of seven patients in a single hospital contracting sternal wound infections with G. bronchialis traced these infections back to a nurse anesthetist. One case report was found in the literature of a recurrent breast abscess caused by Gordonia bronchialis, which required months of doxycycline therapy as well as repeated incision and drainage procedures.
It is unclear how the patient in this case acquired the organism; a thorough infectious disease work-up revealed no signs of immunocompromise, and she had no history of trauma or surgery to the area. Of note, she did have acupuncture performed on her shoulder several months prior to presentation, but no acupuncture was performed in the region of the abscess.
Gordonia bronchialis tends to be widely susceptible to antibiotics; however, treatment failures are frequent. It is believed that the tendency of the organism to form sessile colonies explains these failures.
The patient in this case is currently being treated with Bactrim and Augmentin. Her abscess was re-aspirated several weeks after initiation of therapy when it continued to enlarge, and the second culture is once again growing Gordonia bronchialis. The abscess seems to be improving since this second aspiration, so the treatment team currently plans to continue with oral antibiotics and forego a further incision and drainage procedure.
References:
Richet HM, et al. A cluster of Rhodococcus (Gordona) bronchialis sternal-wound infections after coronary-artery bypass surgery. N Engl J Med 1991;324:104–109.
Siqqiqui N et al. Tibial osteomyelitis caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2012;50(9):3119-21.
Werno AM et al. Recurrent breast abscess caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol 2005;43(6):3009-10.
-Laurie Griesinger is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Over the years, many safety standards and guidelines have been published regarding the Physical Environment of the laboratory (or the Environment of Care). The laboratory environment is not inherently a safe space, so training lab staff about their physical environment is critical so that they may work there without harm. The Physical Environment (PE) includes the overall laboratory space, electrical safety, and compressed gas safety. Physical Environment safety is concerned with ensuring that the facility is constructed, arranged, and maintained to ensure staff and patient safety.
Many labs I have visited are old, and space is often at a premium. Technology has changed over the years in the field of lab medicine, and that has led to the need for different floor plans, counter arrangements, and even work flow patterns. In any lab, the space should be arranged so that the quality of work performed, the safety of the staff, and any patient care given are not compromised. That means there should be enough space to perform the testing required in the department. There should also be room (offices or counter space) for those who perform the administrative work it takes to keep a lab running. Other facilities needs should be available as well such as storage space, rest rooms, staff lockers, a break room, and even meeting space.
One aspect of PE that needs scrutiny is the actual environment (temperature and humidity) of the lab space. The room temperature and humidity need monitoring and controls in order to properly store items in the space, and to ensure that testing is performed in the proper environment determined by the test manufacturer. Working outside of those parameters can have a direct negative impact on patient care. The other important consideration for the environment is staff comfort. Many building systems struggle with maintaining the proper temperature and humidity, especially in the extremes of hot and cold weather months. Will the lab staff remove PPE because it’s too hot? Of course that is an unsafe practice, and finding ways to manage the environment for staff comfort is critical.
Electrical safety should also be considered when evaluating the laboratory Physical Environment. Make sure employees have electrical safety training, and teach them about common errors made from not properly understanding electrical safety. One common error is the use of extension cords. In most locales, extension cords may be used in the lab in an emergency situation (such as accessing emergency power outlets during a power outage), but they should never be permanently placed and used for any lab equipment. The use of “daisy chains” is another common mistake. A daisy chain is made by plugging one multi-plug adapter into another for length. This is a fire hazard and should be avoided.
Compressed gas tanks are often found in the lab environment, and staff needs to adhere to special safety considerations regarding those tanks. Make sure all tanks are secured with a chain or other stabilizing device. A tipping tank, if it breaks open, can blast off like a rocket and cause great damage or even kill. Some tanks have even been propelled through walls or floors. Always transport tanks of compressed gas on a cart, dolly, or hand truck, and ensure all tanks are clearly labeled at all times.
Other considerations in the lab physical environment include the overall neatness and cleanliness of the space. Safety for the staff is improved in a clean and orderly work area. Biohazard work area floors should be wet-mopped at least once a day. Histology and other lab areas that use paraffin in their procedures should make sure the floors are cleaned and scraped so that they are not slippery from the wax. Laboratory counter tops should be neat and orderly, and they should be disinfected after each working shift using a 10% bleach solution or bleach product.
Education and training about PE topics is clearly important, but it is also valuable to regularly monitor the lab space to ensure that safety is maintained. Perform regular (monthly or quarterly) audits on the lab physical environment using a checklist. Use a complete list that covers all of the areas discussed, and be sure review every item on the checklist each time the audit is performed. It is surprising how quickly and easily things change in the lab work space. For example, an analyzer may have been moved for repair and placed back into its original location- but what if that movement caused fraying in the electrical cord? Now there is a fire hazard that didn’t exist just days before, and it needs to be rectified quickly. Sometimes we take for granted the spaces in which we work, but in the laboratory it is important to remember that PE safety needs attention, maintenance, and regular checks. Performing these functions can transform an inherently dangerous space into one in which patient results can be obtained safely.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Recent studies conducted by Brazilian researchers found “super bacteria” in the waters where Olympic athletes will be competing. According to MercoPress, “The Brazilian group’s lead researcher, Renata Picao, said Rio’s “super bacteria” made its way into the city’s waterways through sewage from local hospitals, due to a lack of basic sanitation in the metropolitan area.”
Maryn McKenna writes extensively about antimicrobial resistance. You can watch to her recent TED talk (or read the transcript) to learn why the presence of CRE in Rio’s water is so concerning.
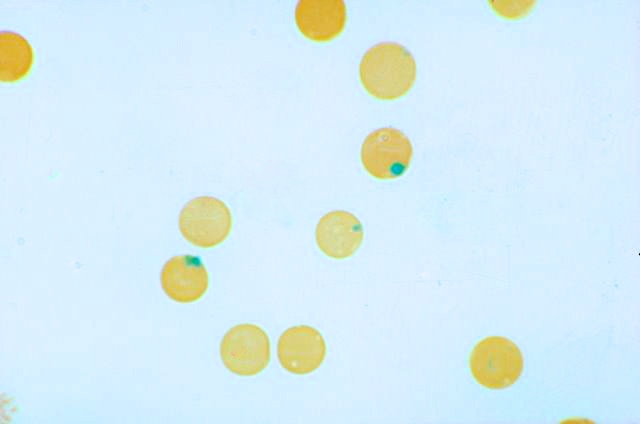
A 22-year-old male presents with shortness of breath and fatigue. He is planning a trip to an area in Africa in which chloroquine-resistant malaria is endemic, and he was started on a prophylactic antimalarial drug regimen several days ago. A blood smear is performed, and stained with a supravital stain. What are the round inclusions within the red cells?
Pappenheimer bodies
Howell-Jolly bodies
Heinz bodies
Hemoglobin H bodies
Warthin-Finkeldey bodies
The inclusions in these red cells are Heinz bodies, which are characteristic of G6PD deficiency. In this disease, the red cells are less able to handle oxidant exposure (common precipitating factors include infection, drug ingestion, and exposure to certain foods, such as fava beans). Following oxidant exposure, hemoglobin denatures and precipitates, forming so-called Heinz bodies which stick to the inside of the red cell membrane, leading to intravascular hemolysis and splenic destruction. Patients with G6PD deficiency typically develop symptoms of hemolysis after a period of two to three days following oxidant exposure. The anemia is usually short-lived and self-limiting.
-Kristine Krafts, MD, is an Assistant Professor of Pathology at the University of Minnesota School of Medicine and School of Dentistry and the founder of the educational website Pathology Student.
A 2-year-old male with no past medical history presented to the emergency department with fever and 2 days of bloody diarrhea. Stool cultures were sent to the laboratory. A Gram stain of the specimen showed the morphology seen in Figure 1. On the 5% sheep blood agar plate, the predominant organism had colonies that appeared flattened and spreading (Figure 2A). On MacConkey agar the colonies were noted to be non-lactose fermenting (Figure 2B). A Hektoen enteric (HE) agar was used as a differential and selective media to differentiate Salmonella from Shigella. On the HE agar the colonies were clear with a green appearance due to the color of the agar (Figure 2C).
Gram stain showing Gram-negative rodsIsolate growing on (A) 5% sheep blood, (B) MacConkey, and (C) Hectoen Enteric agars
Identification
Shigella is a bacterium in the Enterobacteriaceae family and is a Gram-negative rod that is facultatively anaerobic. It is non-motile, a non-spore former, and does not ferment lactose. There are four species of Shigella that are associated with subgroups A-D. Our isolate was identified as Shigella sonnei, which is the most common species in the U.S. and comprises subgroup D. The other subgroup/species correlations are listed in Table 1. The slide agglutination antisera test is used to aid in serogrouping. The suspected colony is mixed on a slide with antisera that contains specific antibodies to Shigella. If clumping (agglutination) occurs, it is considered a positive result for the specific subgroup. The organism was identified as Shigella sonnei by slide agglutination antisera testing. In addition, Shigella has certain biochemical properties that aid in further identification and confirmation.
Table 1: Shigella sp. determination by serogroup
Serogroup
Organism
A
Shigella dysenteriae
B
Shigella flexneri
C
Shigella boydii
D
Shigella sonnei
Clinical Significance
Shigella is one of the most common causes of bacterial gastroenteritis and is often associated with poor sanitation and overcrowded conditions. Transmission occurs through routes such as: fecal-oral and person to person contact. Of note, only a small amount of the bacteria (as low as 10 organisms) is required to cause disease. Hemolytic-uremic syndrome is a complication that may occur with shiga-toxin producing Shigella (the most commonly associated is S. dysenteriae). Shigella has demonstrated antibiotic resistance and therefore does undergo susceptibility testing.
References:
Nataro JP, Bopp CA, Fields, PI, Kaper JB, Strockbine, NA. 2015. Escherichia, Shigella, and Salmonella, p 603-626. In Jorgensen J, Pfaller M, Carroll K, Funke G, Landry M, Richter S, Warnock D (ed), Manual of Clinical Microbiology, Eleventh Edition. ASM Press, Washington, DC.
-Valerie Juarez, M.D., 3rd year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
The purpose of real-time PCR is to perform efficient amplification of a target sequence and quantify the PCR products in “real time” by employing the use of a fluorescent reporter. Fluorescent reporters can found in the form of DNA-binding dyes or fluorescently labeled primers or probes. It is extremely important to understand the difference between DNA-binding dyes, and the various fluorescent primer and probe based chemistries. The best way to grasp these theories is often to have a visual illustration of each of the different chemistries.
DNA-binding Dyes
SYBR Green Dye – SYBR Green I is a fluorescent DNA binding dye that is commonly used as it binds to all double-stranded DNA.
SYBR Green is detected by quantifying the increase in fluorescence during PCR.
Advantages to using SYBR Green are that it is inexpensive, easy to use, and easily incorporated into the PCR reaction.
Disadvantages of using SYBR Green are that there is usually an increase in background and non-specific binding that can lead to detection of false positive results.
Fluorescent PCR Primer and Probe Based Chemistries
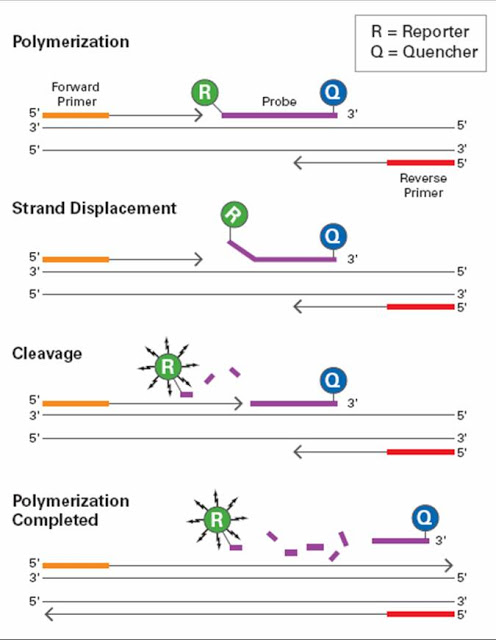
Taqman Chemistry – Utilizes 5’ – 3’ exonuclease activity of Taq Polymerase (enzyme that copies DNA and necessary for PCR) to generate a signal.
The probe is composed of a single stranded DNA oligonucleotide which is complementary to the specific target sequence of the PCR template.
The probe has a modification to the 3’ end so that the polymerase cannot extend the sequence.
The 5’ end has the fluorescent dye and the 3’ end contains the quencher
During DNA synthesis, the exonuclease activity of the Taq Polymerase will degrade the probe, thus resulting in release of the reporter from the quencher.
Molecular Beacon – This type of chemistry measures the accumulation of product during the annealing phase of PCR.
Signal is detected only when probes are bound to the template before displacement by the polymerase.
A chemical modification prevents degradation during the extension step of PCR.
The 5’ end contains the reporter fluorophore and the 3’ end contains the quencher.
The amount of fluorescence is directly related to the amount of initial template available for binding and inversely proportional to the cycle threshold (CT) value.
During extension, the probe is displaced by Taq Polymerase and the hair-pin (non-fluorescent) structure is restored.
Unbound molecular beacon probe à reporter is too close to quencher à no signal is generated.
Beacon probe binds to target à reporter is separated à signal is generated.
Understanding the various primer-probe chemistries including the interactions between the reporters and quenchers will provide some basic groundwork for those interested in pursuing a career in molecular biology.
-LeAnne Noll, BS, MB(ASCP)CM is a molecular technologist in Wisconsin and was recognized as one of ASCP’s Top Five from the 40 Under Forty Program in 2015.
Cryoprecipitate, or cryo for short, is a fresh frozen plasma (FFP)-derived concentrate including fibrinogen, factors VIII and XIII, von Willebrand factor, and fibronectin. Cryo contains only 40-50% of the coagulation factors found in a unit of plasma but is concentrated into a reduced 15-20 ml volume. Cryo is prepared from FFP as it is thawed slowly at 4° C. A precipitate forms at the bottom of the bag, which is then separated from the supernatant plasma. Cryo is stored frozen at at least 18° C and must be transfused within 6 hours of thawing or 4 hours of pooling. Each unit from a separate donor is suspended in 15 mL plasma prior to pooling.
Dose per unit
Half-life
Fibrinogen
150-250 mg
100-150 hours
Von Willebrand factor
100-150 U
24 hours
Factor VIII
80-150 U
12 hours
Factor XIII
50-75 U
150-300 hours
Cryo is used most commonly for replacement of fibrinogen in patients that are bleeding or at increased risk of bleeding. Fibrinogen replacement may be indicated for hypofibrinogenemia (fibrinogen < 100 mg/dL) or dysfibrinogenemia. The target increase in fibrinogen level is 30-60 mg/dL in adults and 60-100 mg/dL in pediatric patients. Many institutions transfuse cryo prior to administration of factor VIIa concentrate to ensure adequate fibrinogen for clot formation given the cost and short half-life of factor VIIa of about 4 hours. Fibrinogen replacement can be monitored with a fibrinogen level assay and clinical response.
Cryo may be used to treat von Willebrand disease, Hemophilia A (factor VIII deficiency), or Factor XIII deficiency only when the appropriate plasma-derived or recombinant factor concentrates are unavailable and/or desmopressin (DDAVP) is ineffective or contraindicated. Cryo is sometimes useful if platelet dysfunction associated with renal failure does not respond to dialysis or DDAVP. Cryo also contains fibronectin; however there are no clear indications for fibronectin replacement.
Topical application of cryo in combination with thrombin as a “fibrin glue” has been used as a surgical hemostatic agent. This application is being discontinued due to the preferred commercially available virus-inactivated fibrin sealants with higher fibrinogen concentrations.
Historically, the dosing was a 10-unit pool for adults and 1-2 units/10kg for pediatric patients based on fibrinogen content. However, Blood Bank and Transfusion services should check with their blood supplier on actual fibrinogen content in individual and pre-pooled units as the fibrinogen content has likely increased (~325 mg) due to improved preparation. Therefore Blood Bank and Transfusion services can probably decrease the standard dose to 4-5 pooled units for adults and 1 unit/10 kg for kids.
A previous version of this post said that cryo is frozen at 1-6°C; this is incorrect. The correct temperature is 18°C, and has been corrected in the text. Thank you, astute readers, for correcting our errors! –Lablogatory editors
-Thomas S. Rogers, DO is a second-year resident at the University of Vermont Medical Center, a clinical instructor at the University of Vermont College of Medicine, and the assistant medical director of the Blood Bank and Transfusion Medicine service.
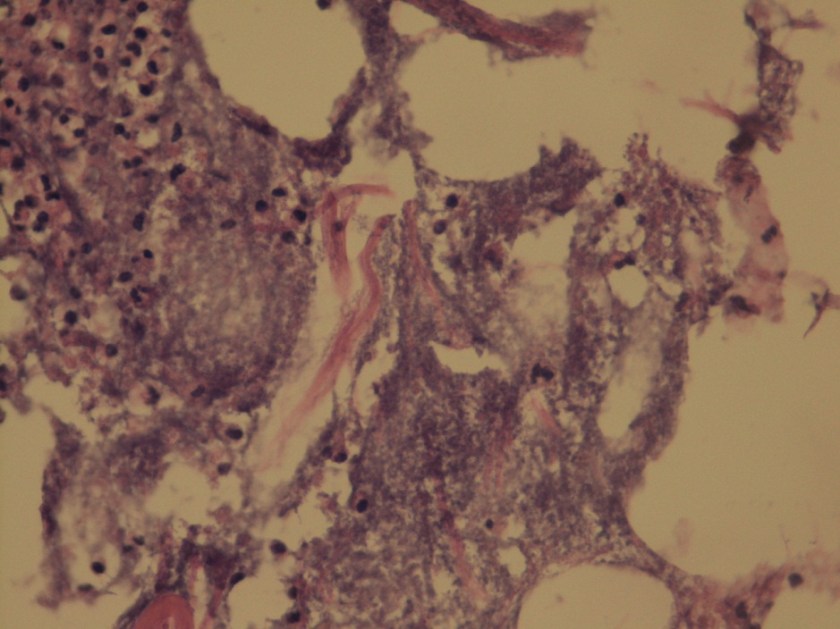
A 72 year old man had been complaining of many months of constipation followed by several months of severe diarrhea prior to admission. He did not receive medical care for these symptoms and had no medical history on file. He presented to an outside hospital unresponsive, and an emergent CT showed subcutaneous emphysema and stranding of the lower abdominal tissue extending to the left hemiscrotum. Also noted was irregular wall thickening in the distal rectum. Of note, his family reported that the patient had hit his left scrotum with a power cord recoil a few days prior to presentation. He was transferred to our hospital, where the surgical team reported severe cellulitis and necrosis of the scrotum, perineum, anterior abdominal wall, and upper thighs. Due to his poor prognosis, the family decided to transition his care to comfort measures only and he passed away several hours after presentation. An autopsy was performed, which revealed liquefaction of the subcutaneous tissue in the lower anterior abdominal wall, dusky gray connective tissue of the left testis as well as a small abscess at the superior pole, and a circumferential distal rectal mass.
Laboratory Investigation:
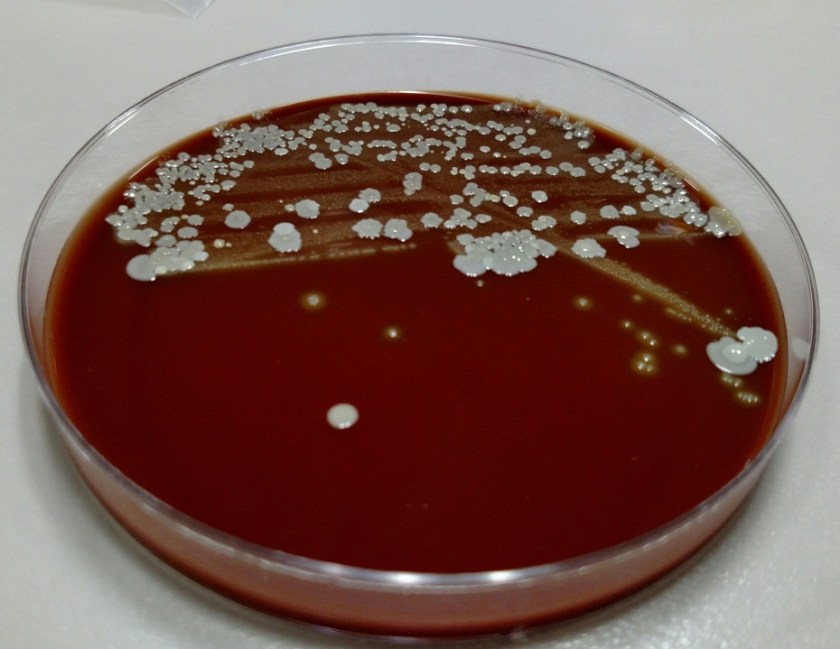
A gram stain of the scrotal abscess and tissue of the anterior abdominal wall both showed mixed gram positive and gram negative organisms. Cultures of these specimens both grew mixed gram positives including alpha hemolytic Streptococcus and coagulase negative Staphylococcus, as well as mixed anaerobes including Bacteroides fragilis group.
Gram stain of the scrotal abscess showing mixed gram negative and gram positive organisms.Histologic section of anterior abdominal wall (400X) showing many polys and many bacterial organisms.Chocolate agar plate showing mixed growth.
Discussion:
The case above represents an example of Fournier’s gangrene, a necrotizing infection of the external genitalia and/or perineum. These infections are most often polymicrobial and often include organisms that would not be particularly aggressive by themselves, suggesting a synergy between anaerobic and aerobic organisms. In a large literature review of over 4,000 cases of Fournier’s gangrene, the most common pathogens involved were Escherichia coli, Streptococcus, Bacteroides, Enterobacter, and Staphylococcus. Our case fits well with this profile, consisting of a mixture of gram positives and gram negatives including Streptococcus, Staphylococcus, and Bacteroides fragilis group. Antibiotic coverage in these cases must be broad spectrum and include coverage for aerobes, anaerobes, gram negative and gram positive organisms.
Risk factors for Fournier’s gangrene include diabetes mellitus, smoking, alcoholism, renal failure, hypertension, and coronary artery disease. It is unclear whether the patient in this case had any of these risk factors as he did not routinely seek medical care.
The rectal mass in this case proved to be adenocarcinoma. There have been multiple case reports of Fournier’s gangrene in association with rectal cancer. The theory behind the mechanism of this association is that perforation of the rectal cancer occurs with tumor infiltration of surrounding tissues spreading infectious organisms. It is possible that our case was caused by the patient’s rectal cancer, but it is also possible that the rectal cancer was simply coincidental. The recent trauma to the patient’s scrotum could also have acted as a vector for infection.
The patient in our case presented too late in the course of his disease to receive appropriate treatment, which would consist of broad spectrum antibiotic administration and aggressive debridement. Even with such treatment, the mortality rate of Fournier’s gangrene is quite high, ranging from 5% to 40% in different case series.
References:
Bjurlin MA et al. Causative pathogens, antibiotic sensitivity, resistance patterns, and severity in a contemporary series of Fournier’s gangrene. Urology 2013;81(4):752-8.
Bruketa T et al. Rectal cancer and Fournier’s gangrene – current knowledge and therapeutic options. World J Gastroenterol 2015;21(30):9002-9020.
-Laurie Griesinger is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.















{kind=link}
{kind=link}
{kind=link}
{kind=link}