A 74 year old female presented to the ED with a chief complaint of fever, right knee swelling and pain for three days. Past medical history was significant for a right total knee arthroplasty approximately 5 months prior, with no significant complications. Physical exam revealed the patient to be febrile (103 degrees Fahrenheit), a swollen right knee that was warm to the touch and erythema surrounding the surgical incision site. Routine labs were obtained while in the ED which revealed a leukocytosis with an elevated ESR and CRP. Imaging was ordered and showed a large joint effusion of the right knee with intact hardware. Arthrocentesis was performed which returned 80 cc of cloudy yellow fluid with no crystals identified by light microscopy, a nucleated cell count of 169,200/cmm of which 97% were neutrophils.
Laboratory Identification
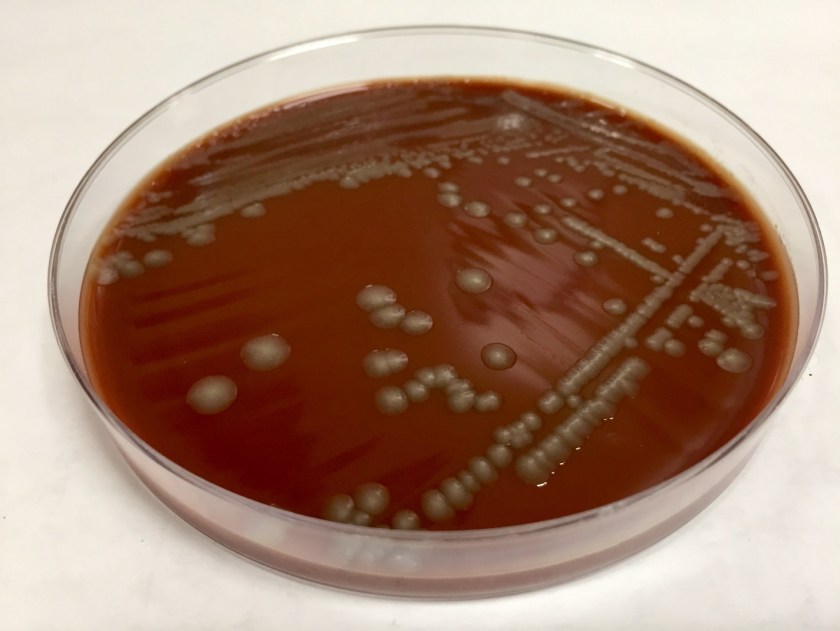
The primary gram stain was reported as polys and gram negative bacilli present. Cultures revealed a pure moderate growth on sheep blood and chocolate agar with no growth on the MacConkey agar. Colony morphology on the sheep blood agar was smooth, gray with no hemolysis appreciated. The key biochemical and physiologic characteristics of the isolate included: positivity for indole, nitrate reduction, catalase, ornithine decarboxylase, and fermentation of mannitol and sucrose; negativity for urea and maltose fermentation. The isolate was identified by MALDI-TOF as Pasteurella multocida. Upon further questioning, the patient admitted to living with two indoor cats but denied any recent history of bites or scratches.
Image 1. Chocolate agar with smooth gray colonies.
Discussion
Pasteurella multocida is a non-motile, oxidase positive, small -gram negative bacilli capable of fermenting glucose. This organism is part of the normal flora of the gastrointestinal tract and nasopharynx of wild and domestic animals. Humans who have extensive exposure to animals may be found to have Pasteurella multocida as part of their upper respiratory tract flora. With no significant virulence factors, this organism is often viewed as an opportunistic pathogen which requires mechanical disruption of anatomic barriers as occurs with bite and scratch wounds from cats and dogs. Though most infections are associated with bites or scratched from animals, infection can occur with non-bite exposure to animals. The typical disease caused by Pasteurella multocida is a focal soft tissue infection following a bite or scratch. However, chronic respiratory infections in patients with preexisting chronic lung disease and heavy animal exposure, and bacteremia with metastatic abscess formation have been documented.
Biochemical characteristics can be utilized in identifying the different Pasteurella species. The key biochemical and physiologic characteristics for Pasteurella multocida include: positivity for indole, nitrate reduction, catalase, ornithine decarboxylase, and fermentation of mannitol and sucrose; negativity for urea and maltose fermentation.
The vast majority of these organisms are susceptible to penicillin, thus susceptibility testing is generally unnecessary. Additionally, soft tissue infections caused by animal bites are frequently polymicrobial and warrant use of therapeutics with a broader spectrum. However, should the need arise to perform susceptibility testing, the Clinical and Laboratory Standards Institute (CLSI) does provide break points for Pasteurella multocida.
Koneman EW. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Lippincott Williams & Wilkins; 2006.
-Justin Rueckert, DO is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 62 year old Caucasian male was referred to the gastroenterology clinic with complaints of epigastric pain, diarrhea and unintentional weight loss over the past couple of weeks. Travel history was significant for a recent mission trip to rural areas of the Philippines. During his time there, he participated in building chicken coops and scuba diving. He reported he mostly ate pork & vegetables but did note he consumed a “runny, undercooked duck egg.” He did not eat any seafood during the trip. About a month after his return, he developed epigastric pain and clinically significant diarrhea, with anywhere from 2-8 bowel movements per day. Testing for blood counts, hepatitis and HIV was performed and stool was collected for culture and ova & parasite exam (O&P). He also underwent a colonoscopy with multiple biopsies.
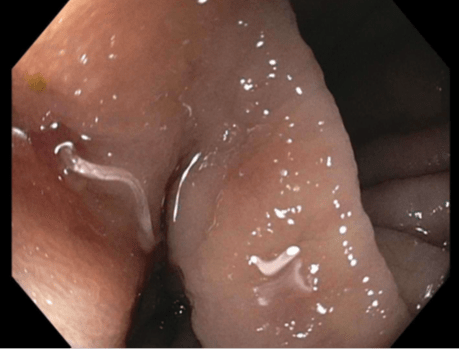
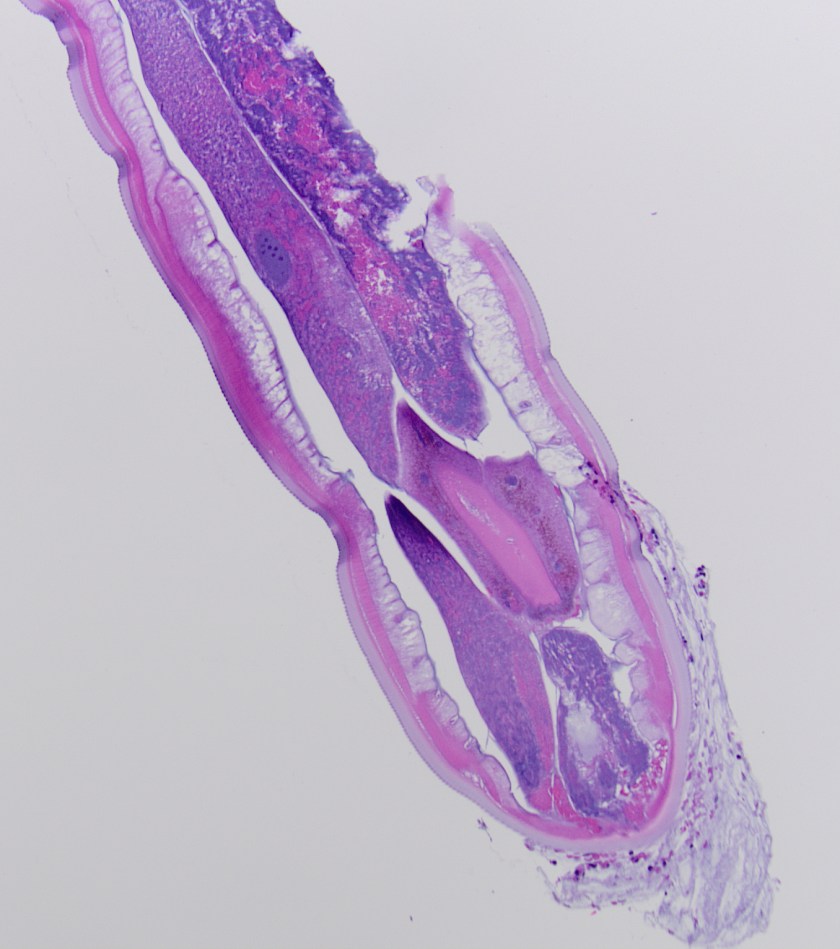
Image 1. During colonoscopy, the mucosa of the cecum was erythematous with small areas of ulceration and multiple helminths were noted.Image 2. Histologic section of an adult helminth showed a thick cuticle with annulations, thin hypodermis and a layer of somatic muscle cells (H&E, 100x).Image 3: Histologic section of a female helminth with numerous barrel shaped eggs identified (H&E, 400x).
Laboratory Identification
CBC revealed a white blood cell count of 17.9 TH/cm2 with 63.5% eosinophils. Acute hepatitis panel and HIV screen were negative as were two sets of stool cultures and O&Ps. Colonoscopy showed multiple helminths at the ileo-cecal junction (Image 1) and histology of the worms revealed architecture and eggs consistent with Trichuris trichiura (Images 2 & 3).
Discussion
Trichuris trichiura is classified as a nematode (roundworm) and is the third most common round worm causing disease in humans. It has a worldwide distribution and infections are most frequent in areas with tropical climates and resource poor settings with inadequate sanitation practices, especially among children. It is estimated that 800 million people are infected worldwide. While most cases diagnosed in the United States occur in immigrants, travelers and military personnel, T. trichiura has also been documented in the southern United States. Clinical presentations are most frequently asymptomatic or mild. Heavy infections, especially in small children, can cause gastrointestinal problems (abdominal pain, diarrhea, rectal prolapse) and possibly growth retardation due to prolonged malnutrition and anemia.
Infection occurs when embryonated eggs are orally ingested with soil contaminated food & water or due to poor hygiene practices. T. trichiura larvae are released in the small intestine and then travel to the colon where they develop into adult forms. Females begin to produce large volumes of eggs (up to 20,000 per day) about 2-3 months after initial infection. Unembryonated eggs are passed in the stool and in warm, moist soil conditions become infective in 15-30 days.
In the laboratory, diagnosis of T. trichiura is most commonly made by identification of the barrel shaped egg with mucous plugs at either end. The eggs have a double shell and are approximately 50-55 um in length. For increased sensitivity, it is recommended that multiple stool specimens for O&P be collected over the course of 7-10 days as shedding is sporadic. Occasionally, adult worms are visualized on colonoscopy and have a long, thin anterior end which attaches to the mucosa and a thicker posterior portion giving the worm a “whip” like appearance. Adult worms typically measure between 3 to 5 cm in length.
Whipworm infections are routinely treated with albendazole or mebendazole. In the case of our patient, he received multiple doses of albendazole and responded well with resolution of symptoms.
-Joy King, MD, is a fourth year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
We recently had a case that made me stop to think about the lengths we sometimes have to go to understand what the bacteria are trying to teach us.
The Issue
Not only are there several methods for the detection of oxacillin resistance in staphylococci (1,2,3), but many laboratories employ a variety of those methods (image 1). This can be a blessing…or a curse. Blessing: alternate methods can be used to referee discordant results. Curse: testing additional methods may cause more confusion. To quote Frank Lloyd Wright, “Less is more only when more is too much.”
The mecA gene encodes for the alternate Penicillin Binding Protein 2a (PBP2a), which confers resistance to oxacillin. In recent years, cefoxitin has become the preferred surrogate for oxacillin to detect methicillin resistance (1, 2). Moreover, as molecular methods become more widely adopted, we open ourselves up to scenarios where the genotype does not match the phenotype. Depending on how your laboratory reports these results, it can be confusing to clinicians. All they want to know is, “Is this MRSA, or not?”
When molecular and culture results do not agree
Many laboratories have turned to polymerase chain reaction (PCR) assays to detect MRSA because of its rapid time to result and its superior sensitivity (compared to AST and PBP2a testing). Recent advances in technology allow for the detection of MRSA direct from positive blood cultures. Rapid organism identification and detection of resistance markers greatly improve patient care by reducing the time to appropriate antimicrobial therapy. However, the problem occurs when the PCR result does not match the PBP2a and/or AST results.
In our laboratory, when a blood culture flags positive the bottles are removed from the automated instrument, a Gram stain is performed, the specimen is subcultured (blood, chocolate, and MacConkey agars) and analyzed (if appropriate) by a multiplex PCR. This workflow allows us to report organism identifications on the majority of our blood cultures on day one of the culture flagging positive (image 1). Final AST results are usually reported by day three. Of note, additional steps are added depending on the Gram stain result. For example, if the Gram stain reveals gram-positive cocci in clusters (GPCL) suggestive of Staphylococcus, then we will also drop a cefoxitin disk onto the blood agar plate.
For this particular case, on day one the Gram stain revealed GPCL and the PCR assay detected S. aureus and mecA, which indicated that the patient had MRSA bacteremia. Nothing out of the ordinary. On day two, we confirmed the culture was S. aureus, but the PBP2a result was negative. Unfortunately, the cefoxitin disk was missed when the culture was originally subcultured (image 2A). Normally, we perform PBP2a testing from cefoxitin-induced growth around the zone of inhibition, but that did not occur in this case. Because the PBP2a and PCR results were discordant, the blood culture was subcultured again to include the cefoxitin disk (image 2B).
The Solution
Image 2A shows a homogenous culture of S. aureus. Under examination no differences could be detected among the colonies; it appears to be a pure culture. Image 2B shows that the culture is actually a heterogeneous culture with both MRSA and MSSA. There are two zones of inhibition around the cefoxitin disk. The white circle highlights the cefoxitin-resistant population and the blue circle highlights the susceptible population. The isolated colonies in the third quadrant look identical; one cannot distinguish between the two populations. This example displays the heterogeneous nature of S. aureus in terms of resistance, or rather its “heteroresistance” to oxacillin and the complexity involved in detecting MRSA.
For those that use phenotypic assays, the use of a cefoxitin disk can help improve your detection rates. Because cefoxitin is both a surrogate for oxacillin resistance and a strong beta-lactamase inducer, it is the perfect aid to enhance MRSA detection (image 2). For this reason, our laboratory implemented the addition of the cefoxitin disk to positive blood cultures with GPLCs. Because we had a few false-negative PBP2a MRSA cases, we decided to start performing PBP2a testing on cefoxitin-induced growth. This intervention has helped two-fold. First, it has seemingly reduced the number of false-negative results. Second, the zone of inhibition functions as an internal control. If the zone is small or non-existent, then it seems obvious that isolate should be resistant. If the zone is large, then we would expect the isolate to be susceptible. Moreover, if we see a double zone as in image 2A, then the culture is likely mixed. [As an aside, we once had a case where the mecA gene detected was from a coagulase-negative Staphylococcus and not the S. aureus (MSSA) that was also present in the culture.]
Image 1. S. aureus workflow. From the time the specimen comes into the laboratory, it can take anywhere from one to three days before a provider knows if their patient has methicillin-susceptible S. aureus (MSSA) or MRSA. MRSA isolates are multidrug-resistant, which require broad-spectrum antibiotics, such as vancomycin (3). For patients with MSSA, narrow-spectrum beta-lactam antibiotics, such as nafcillin or cefazolin are not only the first-line therapy, but superior in terms of outcomes compared to vancomycin (4). Also, patients with MRSA may be put in isolation depending on your institution’s infection control protocol. More importantly, delay of appropriate antibiotics can significantly increase mortality, especially in the case of sepsis (5).Image 2. Cefoxitin induces methicillin resistance. A) A positive blood culture was subcultured to blood agar (no cefoxitin disk). B) The same positive blood culture was subcultured with a cefoxitin disk (30 mg). FOX= cefoxitin. Recall that cefoxitin is a surrogate for oxacillin, therefore resistance to either (oxacillin or cefoxitin) denotes resistance to methicillin.
The Conclusion
Depending on the S. aureus isolate, the detection of methicillin resistance can be a challenge regardless of which method(s) your laboratory utilizes. Fortunately, there is a clear-cut solution. CLSI recommends that isolates should be reported as MRSA if oxacillin resistance is detected by any method (1, 2).
As you saw from our case, the phenotype did actually match the genotype. A combination of heteroresistance and human error (un-induced growth for PBP2a) led us astray. As you read this, you may be thinking, “why did they do all of that?” Good question! We felt that this was a good case to teach and/or learn. “Smart people learn from their mistakes. Geniuses learn from others.” If this can help others learn, then it is all worth it. My gift to you. Merry Christmas!
References
Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; approved standard- tenth edition. CLSI document M07-A10. Wayne, PA: Clinical and Laboratory Standards Institute; 2015.
Performance standards for antimicrobial susceptibility testing. CLSI document M100-S27. Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
Centers for Disease Control and Prevention (CDC). Methicillin-resistant Staphylococcus aureus (MRSA). https://www.cdc.gov/mrsa/lab/index.html. Accessed December 18, 2017.
Schweizer, M.L., Furano, J.P., Harrris, A.D., Johnson, J.K., Shardell, M.D., McGregor, J.C., Thom, K.A., Cosgrove, S.E., Sakoulas, G. and Perencevich, E.N. (2011). Comparative effectiveness of nafcillin or cefazolin versus vancomycin in methicillin-susceptible Staphylococcus aureusBMC Infect. Dis. 11:279. doi: 10.1186/1471-2334-11-279
Kumar, A., Roberts, D., Wood, K.E., Light, B., Parrillo, J.E., Sharma, S., Suppes, R., Feinstein, D., Zanotti, S., Taiberg, L., Gurka, D., Kumar, J. Cheang, M. 2006. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Care Med. 34:1589-1596. doi: 10. 1097/01.CCM.0000217961.75225.E9
-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
A 57 year old male presented to the ED with the chief complaint of fever (103 degrees Fahrenheit), urinary retention, backache and headache. The patients past medical history is significant for penile cancer status post total penectomy with perineal urethrostomy and pelvic lymph node dissection approximately 12 months prior, recent urinary tract infection (2 weeks prior, treated with 7days of antibiotics), recent pace maker placement (2 months prior), Group B Streptococcus cellulitis of the left leg complicated by bacteremia (7 months prior). The patient requires use of in and out catheters for urination as a result of the penectomy and perineal urethrostomy; however he has had difficulty with catheterization recently secondary to urethral stenosis.
Physical examination revealed the right inner thigh to be erythematous, warm, and mildly tender, clinically consistent with cellulitis. The cellulitis appeared to be spreading along the medial aspect of the thigh and involving the lower leg. While in the ED, two sets of blood cultures were obtained and a urinalysis was significant for 1+ blood, 1+ nitrite, 1+ leukocyte esterase. He was subsequently treated with intravenous fluids and ceftriaxone and admitted to the hospital.
Laboratory Identification
Both sets of the blood cultures were positive (3/4 bottles), with the first bottle being positive after 11 hours of incubation. Gram smears of the bottles revealed the presence of gram positive cocci resembling Streptococcus. Per laboratory procedure, the positive bottles were analyzed utilizing the Luminex Verigene platform and resulted as Streptococcus species. The blood culture broth was subcultured to sheep blood agar and revealed a pure isolate of medium sized slightly opaque gray colonies with a large zone of beta hemolysis. The bacteria were found to be catalase negative and PYR negative. The organism was identified by a latex agglutination assay as Group C streptococci.
Image 1. Sheep blood agar plate with beta hemolytic colonies.
Discussion
Group C streptococci designates Streptococcus species which react with Lancefield group C typing serum. Group C streptococci are comprised of several different Streptococcus species including S. dysgalactiae subspecies equisimilis, S. dysgalactiae subspecies dysgalactiae, S. equi subspecies equi, and S. equi subspecies zooepidemicus. The most commonly isolated species in human clinical specimens is S. dysgalactiae subspecies equisimilis. Group C streptococci are considered normal flora of human skin, nasopharynx, gastrointestinal tract and genital tract. The mode of transmission for these organisms includes endogenous isolates gaining access to sterile sites and person to person transmission. No definitive unique virulence factors have been identified to date; however similar virulence factors to those of S. pyogenes and S. agalactiae are likely. The diseases caused are similar to those caused by S. pyogenes and S. agalactiae including bacteremia, endocarditis, arthritis and skin and soft tissue infections. Disease generally occurs in patients in immunocompromised states or with multiple comorbidities. There have been documented cases of zoonotic infections with S. equi subspecies zooepidemicus in patients with farm animal exposure, however not all infections are associated with animal exposure. S. equi subspecies zooepidemicus is a causative agent of bovine mastitis and has been documented as the etiologic agent in several outbreaks attributed to ingestion of inadequately pasteurized dairy products. Group C streptococci are susceptible beta-lactam antibiotics, and penicillin is considered the drug of choice for treatment.
Koneman EW. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Lippincott Williams & Wilkins; 2006.
Pelkonen S, Lindahl SB, Suomala P, et al. Transmission of Streptococcus equi subspecies zooepidemicus infection from horses to humans. Emerging Infect Dis. 2013;19(7):1041-8.
-Justin Rueckert, DO is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
The courier suddenly became sleepy in the middle of his daily driving route. It was cold outside and he had all of the windows in the vehicle closed. He also had filled his cooler with four pounds of dry ice, and it was sitting in his back seat.
There was no education at the hospital for specimen collection staff regarding proper label placement on collection tubes. Since the CBC analyzer would not accept tubes with labels that were too long, the lab techs kept a razor blade handy to slice off extra label paper. It wasn’t long before someone cut their finger.
The phlebotomist completed the outpatient collection, but the large elderly patient was unable to stand up from the chair without assistance. The phlebotomist bent at the waist and attempted to lift the patient to standing. The back muscle pull that followed kept the phlebotomist out of work for two weeks.
Every laboratory professional understands the value of quality in the pre-analytic phase of laboratory testing. If you have ever worked where phlebotomy has been decentralized and is no longer overseen by the laboratory, you may have experienced the many pitfalls due to inadequate specimen collection techniques. Laboratory professional by nature want to provide good diagnostic results, and compromised specimens hinder that resolve. Sometimes, however, the aspects of safety that are important during the pre-analytic phase of lab testing get overlooked.
Needle safety and ergonomics should be considered during blood collection from patients. Using a needle with an attached safety device and activating it as soon as possible are important steps in needle stick prevention. Make sure there is a sharps disposal container near the point of collection or wherever needles are used so that the potential hazard can be eliminated quickly. When collecting blood, be sure to raise the bed height (or the arm height if in a chair) so that excessive bending is avoided. Use a chair or a task stool to sit on while performing the collection to maintain a better posture throughout the procedure. Never attempt to lift patients by yourself, always ask for help. Thousands of back injuries occur every year in healthcare due to avoidable patient lifting errors.
For many laboratories, couriers are a vital part of the pre-analytic process. They bring specimens from clients and other labs, and their safety should be considered as well. Teaching dry ice safety is vital if it is used, and both couriers and lab staff need to be taught how to handle it appropriately. Dry ice sublimates (or changes to gas from a solid state), so it should never be placed into a sealed container, or the building pressure from expansion will cause the container to explode. Couriers should never place more than one pound of dry ice inside a vehicle, and the windows should be opened when transporting it to create good ventilation. The gas created from dry ice quickly reduces the oxygen content in the air, and the elevated Carbon Dioxide levels can quickly cause unconsciousness or even death. Never place dry ice leftovers in the sink for disposal. While it might be fun to run water on it to see movie special effects, the cold temperatures can burst sink pipes and even make the entire sink fall out of place.
If specimens for analysis arrive in the testing area, and they frequently aren’t ready for analysis- for instance the labels aren’t placed properly- go to the source of the error to make corrections. If inappropriate labeling is a constant problem, staff will create work-arounds to get the work done, and some of these work-arounds may not be safe. Poorly-labeled samples may prompt a lab tech to remove gloves in order to adjust the sticky labels, and that should never occur. The use of sharp blades may be another work-around, and staff injuries can occur. Be sure to explain to specimen collection staff the importance of proper labeling. Turnaround times are delayed, but staff safety is also a concern.
Lab Quality and Safety are often related, and rarely is it more so than during the pre-analytical phase of testing. Proper collection, labeling, and processing are all vital in order to provide high quality lab results, and that is the crux of what laboratorians wish to do. The same can be said for laboratory safety: that pre-analytical process can’t be done well without proper safety considerations. Safety events here will create staff injury, turnaround time delays, and potential errors with test results. Make sure staff understand the impact of good quality as well as safety in the pre-analytical phase.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A 45 year-old man presented with vomiting and diarrhea for 5 days. Laboratory studies demonstrated anemia and thrombocytopenia, an elevated ferritin level (23,772 ug/L) and methemoglobinemia. Chest roentgenography revealed cardiomegaly. A follow-up ECHO showed a desreased ejection fraction of 15%. Work-up confirmed viral myocarditis and G6PD deficiency as the cause of the cardiac findings and methemoglobinemia respectively. His clinical condition deteriorated despite therapy: he developed acute kidney and liver failure and had worsening cytopenias. A bone marrow biopsy was performed.
Evaluation of the peripheral blood (not pictured) confirmed a macrocytic anemia with marked anisopoikilocytosis including schistocytes, polychromasia, nucleated red blood cells, absolute neutrophilia, monocytosis and thrombocytopenia. The marrow aspirate smear demonstrated appropriate maturation in all cell lines. Scattered hemophagocytic histiocytes (pictured above) were noted. The bone core biopsy was high-normocellular for age with progressive trilineage hematopoeisis. Scattered histiocytes with internalized erythroid cells and debris were visualized. There was no increase in blasts. Flow cytometry analysis performed on the bone marrow aspirate did not show a significant increase in blast population. Gating on the lymphocytes did not show a B-cell monoclonal population or T-cell abnormality by markers assayed.
Diagnosis
High-normocellular marrow with progressive trilineage hematopoeisis and prominent hemophagocytic histiocytes.
Overall the patient met the clinical criteria (see below) for Hemophagocytic Lymphohistiocytosis (HLH); with fever (≥38.5 C), splenomegaly, bicytopenia, presence of hemophagocytic histiocytes in bone marrow and high ferritin level (>500ng/mL).
A clinical diagnosis of HLH was rendered.
Discussion
HLH is an uncommon hematologic disorder that is often fatal. The underlying pathogenesis involves an exaggerated but ineffective inflammatory response of excessive macrophage and T-cell activation, and impairment of natural killer (NK) and cytotoxic T-cell function. HLH has familial and acquired forms. Secondary, or acquired HLH can be associated with infections (especially viral etiologies), underlying malignancy (particularly lymphomas and leukemias), and medications used for systemic lupus erythematosus. Clinically, autoimmune disease-associated HLH overlaps significantly with macrophage activation syndrome (MAS).
HLH is a clinical diagnosis that can be established with molecular testing or by meeting five of eight clinical and laboratory diagnostic criteria according to the HLH-2004 guidelines.
HLH-2004: Revised diagnostic guidelines for HLH10
The diagnosis HLH can be established if one of the two criteria below is met:
A molecular diagnosis consistent with HLH (i.e., reported mutations found in either PRF1 or MUNC13-4); or
Diagnostic criteria for HLH are fulfilled (i.e., at least five of the eight criteria listed below are present:
Persistent fever
Splenomegaly
Cytopenias (affecting ≥2 of 3 lineages in the peripheral blood):
Hemophagocytosis in bone marrow* or spleen or lymph nodes, no evidence of malignancy
Serum ferritin ≥ 500µg/L (i.e., 500 ng/ml)
Low or absent NK cell activity (according to local laboratory reference)
Increased serum sIL2Rα (according to local laboratory reference)
*In hematopathology, the finding of relevance is the presence of hemophagocytic histiocytes in the marrow or other biopsies organs. While debris-laden histiocytes are commonly noted in marrow aspirates, the findings of engulfed erythroid cells is warranted to call a ‘hemophagocytic’ histiocyte.
Often a bone marrow biopsy will be performed in cases where there is clinical suspicion for HLH. This serves to try and visualize the hemophagocytic activity, and to rule out other diseases with similar clinical presentations as HLH. The pathologic evaluation of HLH is tricky, since there is no established criteria for quantitation of hemophagocytic histiocytes in a bone marrow aspirate. Furthermore, hemophagocytosis is not specific to HLH and can be seen in other conditions such as: post-blood transfusion, chemotherapy, sepsis and major operations. Published data shows that the presence of hemophagocytosis has a sensitivity of 83% and a specificity of only 60% in diagnosing HLH.
What about immunohistochemical staining for the histiocytes? While IHC can help outline histicoytic cells, unfortunately, quantitation of hemophagocytic histiocytes in the core biopsy or clot sections with the aid of CD68 immunostains does not correlate well with disease probability either.
Overall, the nonspecificity of hemophagocytosis in the marrow, even when present in high amounts, should remind both pathologists and clinicians that an isolated finding of hemophagocytosis lacks specificity and does not necessarily suggest HLH when the clinical presentation and laboratory findings are not compatible with the diagnosis. However, there still remains value in bone marrow biopsy examination in cases where clinical suspicion for HLH is high; in order to exclude other marrow processes; and in the rare case where there may not have been clinical suspicion of HLH but the presence of hemophagocytic histiocytes can raise that differential.
Ho C, Yao X, Tian L, et al. Marrow Assessment for Hemophagocytic Lymphohistiocytosis Demonstrates Poor Correlation with Disease Probability. Am J Clin Pathol. 2014 Jan;141(1):62-71
Hunter JI et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007 Feb;48(2):124-31.
-Ayse Irem Kilic is a 1st year anatomic and clinical pathology resident at Loyola University Medical Center. Follow Dr. Kilic on twitter @iremessa.
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
Laboratories occasionally get questions from clinicians about prolactin results, mainly to either rule out high-dose hook effect or assess interference from macroprolactin. In most laboratories, sandwich immunoassay is used to measure prolactin concentration and it is widely known that older generations of prolactin assays suffer from hook effect and interference from macroprolactin. In the presence of extremely high concentration of prolactin, antibodies can be saturated, resulting in falsely low results, which is known as high-dose hook effect. Multiple cases have been reported in patients with giant prolactinomas, that their prolactin results were measured as normal or moderately elevated. In order to rule out high-dose hook effect, clinicians normally request laboratories to perform appropriate dilutions for prolactin in patients with large pituitary tumors. Newer generation of prolactin assays have better performance in this aspect, and most assays nowadays have no hook effect up to concentrations of 10,000 ng/mL, claimed by manufactures.
Another pitfall of prolactin assay is the interference from macroprolactin. Macroprolactin is a complex of prolactin bound to immunoglobulin, and thought to be biologically inactive. In the presence of elevated macroprolactin, patient is asymptomatic. However, macroprolactin can be picked up by prolactin immunoassays to some extent, and results in misdiagnosis as hyperprolactinemia. Reports showed that 15-20% of cases with hyperprolactinemia was due to elevated macroprolactin. Therefore, macroprolactinemia should be considered while evaluating hyperprolactinemia cases in the absence of symptoms or pituitary imaging evidence. Laboratories could easily perform dilution study to test if interference exists. To confirm the presence of macroprolactin, polyethylene glycol (PEG) 6000 can be used to precipitate macroprolactin followed by prolactin measurement in the supernatant. The presence of macroprolactin is suggested when the pull-down percentage is greater than 40-50%. This test is offered by many reference laboratories.
These two pitfalls of prolactin biochemistry assays should always be kept in mind by laboratorians, to provide better guidance to clinicians’ concern and workups on prolactin related cases.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
A 62 year old male without a significant past medical or smoking history was referred to pulmonology for an abnormal chest CT. Three months prior to presentation, the patient had developed a cough after doing some home remodelling that involved sanding drywall. The cough became severe and blood-tinged, including some clots, so the patient sought medical attention. The patient denied any other symptoms and reported feeling well overall. Physical exam findings were all within normal limits. A chest X-ray showed a round lesion in the left lower lobe. Follow-up chest X-rays showed that the lesion had decreased in prominence but had not resolved. Subsequently, a chest CT was performed that showed a 2.8cm mass-like focal area of consolidation in the left lower lobe without associated lymphadenopathy. Because malignancy could not be excluded, the patient underwent bronchoscopy with biopsies obtained for cytopathologic evaluation as well as mycobacterial and fungal cultures.
Image 1: Cytologic preparation (alcohol-fixed, Papanicolaou-stained) of lung, left lower lobe, 2.8cm mass, fine needle aspiration.
The cytologic preparation of fluid from a fine needle aspiration (Image 1) shows granulomatous inflammation with patchy necrosis. Typically, a mixed inflammatory reaction is observed, with neutrophils, granulomas, epithelioid histiocytes, and foreign body giant cells. Examination reveals several round-to-oval yeast cells, measuring 9-13μm in diameter. Single broad-based (4-5 μm wide) buds and thick, double contoured, refractile cell walls are also characteristic of the yeast forms visualized here, leading to a rapid presumptive diagnosis.
Image 2: Scotch Tape touch preparation of one white colony growing on potato flake agar (25°C) after 10 days of incubation.
Growth of the fungus on various culture media is more sensitive than direct examination and yields a definitive diagnosis. On potato flake agar incubated at room temperature (25°C), one white colony that was tan on the reverse began growing at 8 days. Typically, colonies appear in 1-4 weeks and range from white (initially) to brown (with age). Microscopic examination of a Scotch Tape touch prepared at 10 days (Image 2) demonstrates the mold form of this dimorphic fungus has delicate, septate hyphae with right-angle conidiophores that bear single, terminal conidia (resembling lollipops). A DNA probe is used to confirm the identification of Blastomyces dermatitidis.
Discussion
As described above, Blastomyces dermatitidis is a thermally dimorphic fungus. In the environment, the mold form of B. dermatitidis is found in wet soil, particularly when enriched by animal droppings and decaying organic matter (1). When a susceptible host (healthy or immunocompromised) disrupts wet earth that contains B. dermatitidis, infectious conidia are inhaled into the lungs. Adult men are more likely to have blastomycosis, likely because they partake in outdoor activities (ex. hunting, fishing) that are associated with environmental exposure to airborne conidia.
Symptoms of blastomycosis are variable, ranging from asymptomatic or transient flu-like to severe pulmonary involvement. Patients may present with symptoms of acute pneumonia (fevers, chills, cough, hemoptysis, and dyspnea) that can be indistinguishable from viral or bacterial causes. Other patients, with chronic pneumonia, have systemic symptoms (weight loss, low-grade fevers, night sweats, productive cough, and chest pain) that overlap with pulmonary tuberculosis, histoplasmosis, or bronchogenic malignancy. In addition to the primary pulmonary infection, approximately half of patients develop extrapulmonary symptoms from hematogenous dissemination to almost any organ; most commonly to skin, bones, male genitourinary, and the central nervous system.
Regardless of symptoms, a majority of patients with blastomycosis will have chest X-ray findings, alveolar infiltrates or a mass lesion involving any location that are non-specific and may mimic malignancy. The mortality rate is 0% in healthy hosts and up to 30% in immunocompromised people, frequently due to disseminated disease. There are no guidelines for susceptibility testing of dimorphic fungi. The preferred treatment of mild to moderate pulmonary blastomycosis is itraconazole for 6-12 months. Conversely, amphotericin B is used in moderately severe disease to treat chronic pulmonary symptoms, disseminated blastomycosis, CNS involvement, immunocompromised or pregnant patients.
Reference
Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Microbiol Rev. 2010;23(2):367-81.
-Adina Bodolan, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 72 year-old female with a history of stage IA lung adenocarcinoma diagnosed in 2009 s/p resection underwent a surveillance CT scan of the chest which revealed an enlarged right upper lobe paramediastinal lung nodule. A subsequent MRI of the abdomen and PET scan revealed mediastinal lymphadenopathy with numerous boney lesions. Due to the prior history of lung cancer, a right iliac bone biopsy was performed.
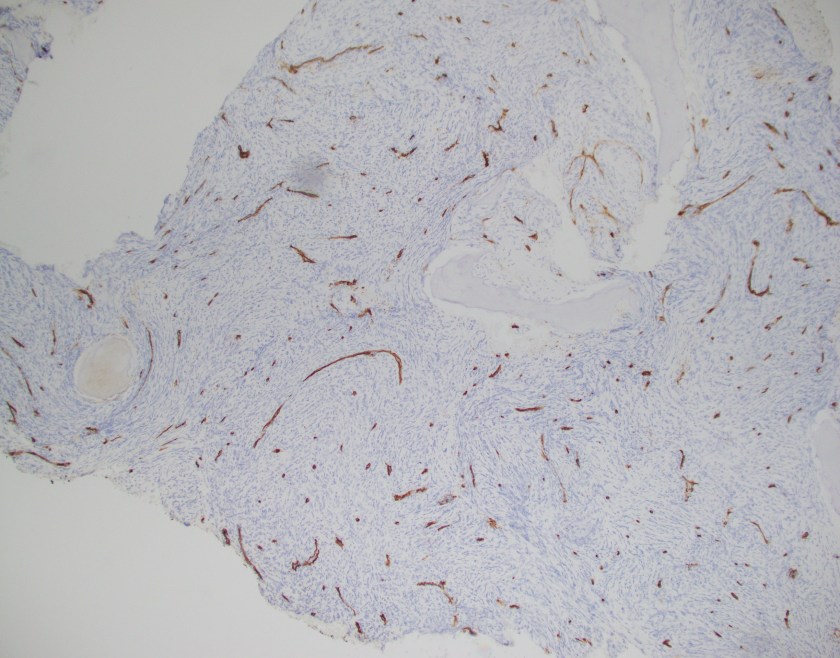
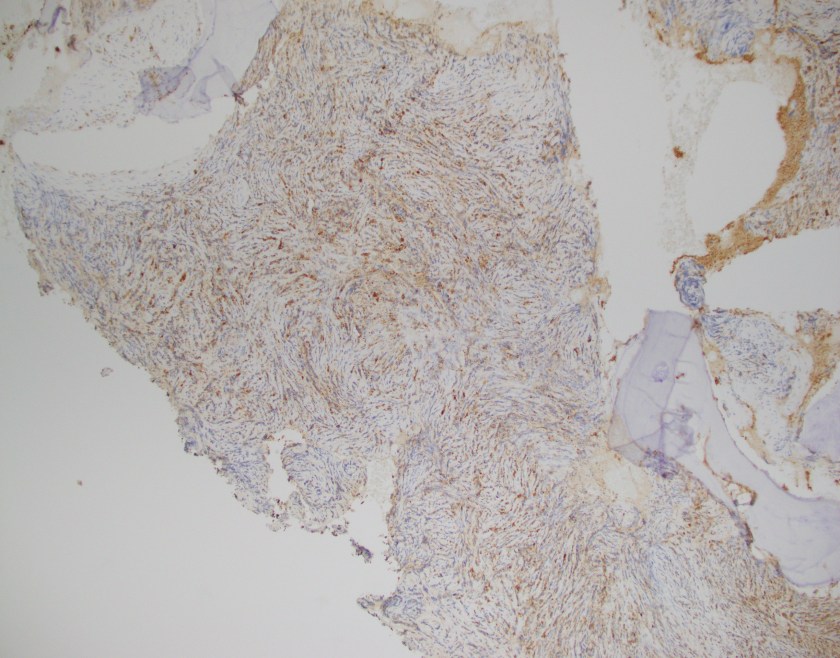
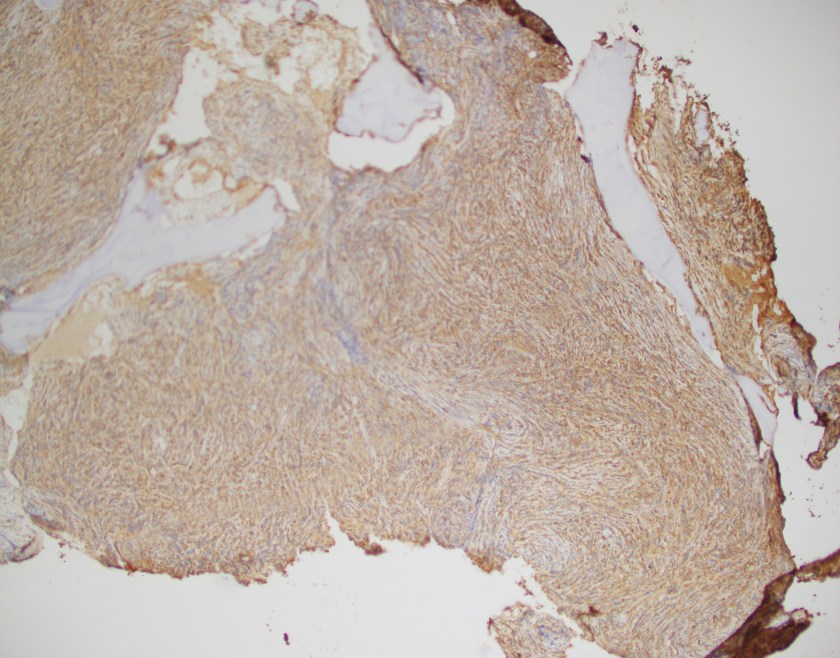
Sections of bone show an extensive intramedullary infiltration by large cells with moderate amounts of cytoplasm, irregular nuclear contours, moderately condensed chromatin and some cells with inconspicuous nucleoli.
By immunohistochemistry, the neoplastic cells are immunoreactive for CD45, MPO, CD68, CD56, and CD43. The cells are negative for cytokeratins, TTF-1, CD20, CD10, PAX5, BCL6, MUM1 and CD79a. CD3 and CD5 highlight rare scattered T-cells.
Overall, in the context of multiple osseous lesions, these findings are representative for a myeloid sarcoma.
Discussion
Myeloid sarcoma is a tumor mass consisting of myeloid blasts with or without maturation occurring at any site other than the bone marrow. Infiltration of blasts at any site are not classified as a myeloid sarcoma unless there is effacement of tissue architecture. Frequent sites for involvement by a myeloid sarcoma include skin, lymph node, gastrointestinal tract, bone, soft tissue, and testis.
Detection of a myeloid sarcoma is considered as an equivalent diagnosis of acute myeloid leukemia. It may precede or coincide with AML as well as be a presenting finding in those that relapse from AML.
Morphologically, the blasts may or may not show features of maturation and efface the architecture of the involved site. Immunophenotypically, CD68 is considered the most commonly expressed marker followed by MPO, CD117, lysozyme, CD34, TdT, CD56, CD30, glycophorin and CD4. Interestingly enough, CD123 may be expressed in those cases that also have inv(16). It must be emphasized that those cases that meet criteria for a mixed phenotypic acute leukemia (MPAL) cannot be classified as a myeloid sarcoma.
By cytogenetics, 55% of myeloid sarcomas have aberrant cytogenetic findings including monosomy 7, MLL rearrangements, inv(16), and other chromosomal changes. In the pediatric population, t(8;21) may be observed and is less frequent in adults. NPM1 is mutated in 16% of cases.
Lastly, the differential diagnosis should be kept broad in cases that appear lymphoid in nature yet do not mark appropriately. It is often expressed that the primary morphologic differential is a lymphoma, including lymphoblastic lymphoma, Burkitt lymphoma, diffuse large B-cell lymphoma, blastic plasmacytoid dendritic cell neoplasm, and other small round blue cell tumors of childhood.
Reference
Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2008
-Phillip Michaels, MD is a board certified anatomic and clinical pathologist who is a current hematopathology fellow at Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. His research interests include molecular profiling of diffuse large B-cell lymphoma as well as pathology resident education, especially in hematopathology and molecular genetic pathology.
Holiday season is around the corner! And, as such, I’d like to take this opportunity to share a few thoughts I have on how our professional scope as laboratorians extends all the way from the bench to the dinner table.
How many times have you been asked by friends and family what it is exactly you “do” at work? And how many times have you done your best to explain, being met with references to unrealistic television shows or generalizations that go beyond your scope of practice? It’s happened to me a million times. It’s the nature of our laboratory culture. It’s a vital role in patient outcomes, but often behind the scenes. But just for a moment, let’s say you get beyond those surface explanations—what happens next? Probably, in most cases, not much.
One of the main tenets of the ASCP mission which we all work together is advocacy: for our communities, our institutions, our teams, and our patients. More often than not I would bet that family members venture into that turnpike, mostly as patients. When a grandparent, uncle, sister, or friend says they’ve got an upcoming procedure or test, how many of us would share our knowledge with him or her? I know I would. Not in a way that goes beyond our scopes as phlebotomists, medical laboratory scientists, or cytotechnologists, or medical students, or pathologists—but as someone who wants to empower their loved one to be the most informed and prepared patient they can be. In 2012, the Agency for Healthcare Research and Quality (AHRQ) promoted their campaign “Questions to Ask Your Doctor.” In it, they cite that good health depends on good communication and that patients should not be afraid to ask their physician questions about their health outcomes. You remember, the commercials with the guy at the cell phone store that asked a hundred free train-of-thought questions but was speechless in front of his doctor…I loved those.
In that same holiday spirit that celebrates thankfulness, family, and relationships, let’s include laboratory professionals! If you have a loved one who it applies to, explain just what happens after those six different colored tubes were drawn, explain how that removed mole was set, sectioned, and reviewed, explain how staining different cells in a body fluid give a clinician important data about their health. Hundreds of thousands of laboratory professionals in the United States could offer not just invaluable information to their friends and family, but peace of mind. Demystifying the medical process might make those patience more confident in asking informed questions and, together with their provider, improve their health outcomes.
I find myself in an interesting position today. Having years of explaining what CBCs or CMPs actually measure and why someone might have to fast before a lipid panel, I’ve started a slow transition to learning how to explain what that means to an individual’s health. What a fantastic foundation lab medicine gave me to build on! (Really a recurring theme you’ll see in lots of my posts.) By moving from what different stains mean to a clinician, I am now on a path toward being able to use that information for the next step in professional scope: diagnosis and management.
Just like I’m on this academic and professional journey, lots of us are on a path through or toward something. But back to our ASCP message, advocacy for patients means recognizing their journey—especially when they’re our family and friends. The best outcomes for any patients rely on valuable information, communication, and rapport. And while you help your loved ones through the steps of their journey as a patient you might empower them to be a more involved member of their healthcare team. As a result, they might experience more personal and effective care. And a bonus just for us: maybe more people would appreciate some behind the scenes lab medicine. Who knows?
So, from me and mine to you and yours, have a great holiday season and a wonderful new year! I’ll return with stories, cases, and commentary on medical school clinicals in January!
Take care and thanks for reading!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.