Case history
A 72 year-old female with a history of stage IA lung adenocarcinoma diagnosed in 2009 s/p resection underwent a surveillance CT scan of the chest which revealed an enlarged right upper lobe paramediastinal lung nodule. A subsequent MRI of the abdomen and PET scan revealed mediastinal lymphadenopathy with numerous boney lesions. Due to the prior history of lung cancer, a right iliac bone biopsy was performed.
Diagnosis





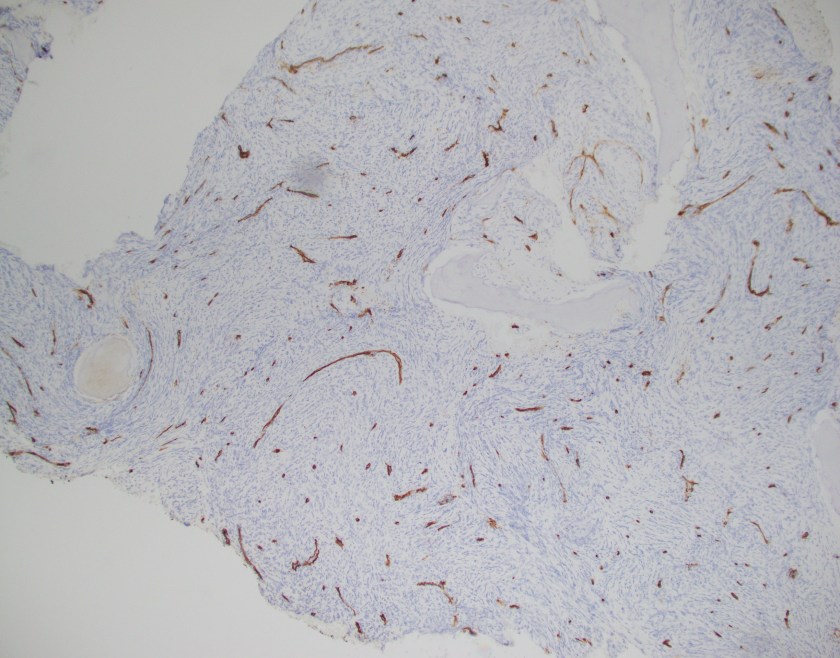
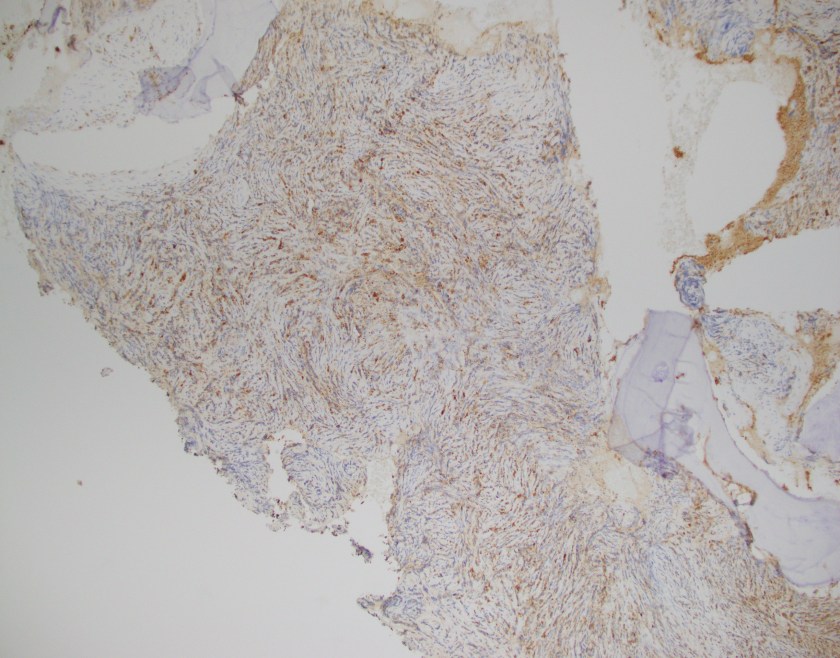

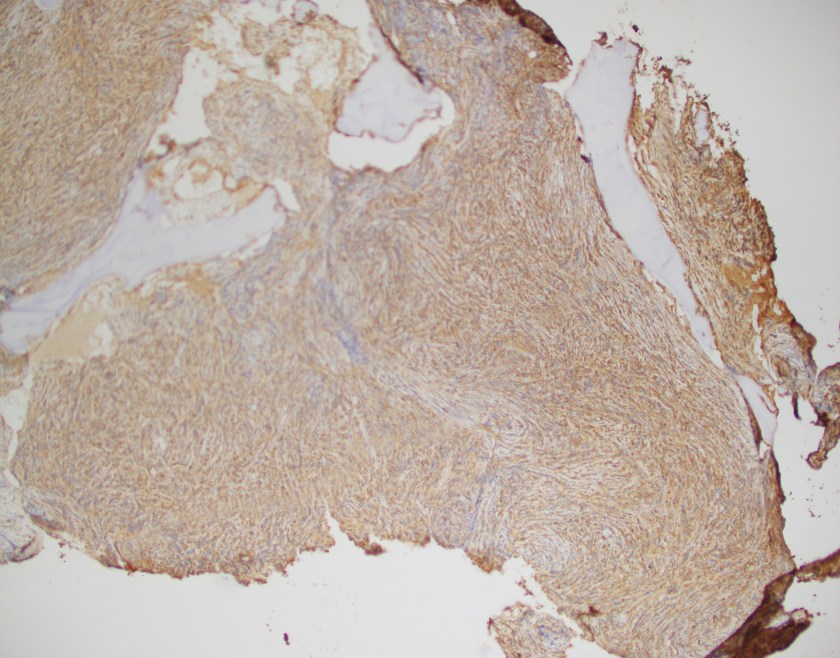

Sections of bone show an extensive intramedullary infiltration by large cells with moderate amounts of cytoplasm, irregular nuclear contours, moderately condensed chromatin and some cells with inconspicuous nucleoli.
By immunohistochemistry, the neoplastic cells are immunoreactive for CD45, MPO, CD68, CD56, and CD43. The cells are negative for cytokeratins, TTF-1, CD20, CD10, PAX5, BCL6, MUM1 and CD79a. CD3 and CD5 highlight rare scattered T-cells.
Overall, in the context of multiple osseous lesions, these findings are representative for a myeloid sarcoma.
Discussion
Myeloid sarcoma is a tumor mass consisting of myeloid blasts with or without maturation occurring at any site other than the bone marrow. Infiltration of blasts at any site are not classified as a myeloid sarcoma unless there is effacement of tissue architecture. Frequent sites for involvement by a myeloid sarcoma include skin, lymph node, gastrointestinal tract, bone, soft tissue, and testis.
Detection of a myeloid sarcoma is considered as an equivalent diagnosis of acute myeloid leukemia. It may precede or coincide with AML as well as be a presenting finding in those that relapse from AML.
Morphologically, the blasts may or may not show features of maturation and efface the architecture of the involved site. Immunophenotypically, CD68 is considered the most commonly expressed marker followed by MPO, CD117, lysozyme, CD34, TdT, CD56, CD30, glycophorin and CD4. Interestingly enough, CD123 may be expressed in those cases that also have inv(16). It must be emphasized that those cases that meet criteria for a mixed phenotypic acute leukemia (MPAL) cannot be classified as a myeloid sarcoma.
By cytogenetics, 55% of myeloid sarcomas have aberrant cytogenetic findings including monosomy 7, MLL rearrangements, inv(16), and other chromosomal changes. In the pediatric population, t(8;21) may be observed and is less frequent in adults. NPM1 is mutated in 16% of cases.
Lastly, the differential diagnosis should be kept broad in cases that appear lymphoid in nature yet do not mark appropriately. It is often expressed that the primary morphologic differential is a lymphoma, including lymphoblastic lymphoma, Burkitt lymphoma, diffuse large B-cell lymphoma, blastic plasmacytoid dendritic cell neoplasm, and other small round blue cell tumors of childhood.
Reference
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2008

-Phillip Michaels, MD is a board certified anatomic and clinical pathologist who is a current hematopathology fellow at Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. His research interests include molecular profiling of diffuse large B-cell lymphoma as well as pathology resident education, especially in hematopathology and molecular genetic pathology.
