A 50 year old female with a complex medical history consisting of lymphoma, diabetes mellitus (type II), sarcoidosis, congestive heart failure, chronic renal failure (stage 3), and pancytopenia presented to the emergency department with shortness of breath, cough, fever. She was found to be positive for SARS-CoV-2 and was transferred to the ICU due to hypoxic respiratory failure. She was treated for sepsis and respiratory failure, but her status continued to decline. The patient had multiple admissions due to COVID-19 in the past, received remdesivir and was on corticosteroid therapy due to the interstitial lung disease from last year. Initial evaluation included complete blood count which revealed anemia (hemoglobin=8.7 mg/dl), leukocytosis (WBC = 21,900/mcl), lymphopenia (910/mcl) and thrombocytopenia (Plt = 27000/mcl). The patient was treated with broad antibiotics and additional steroids. Additional tests revealed hyperproteinemia and hypoalbuminemia. Chest x-ray showed worsening infiltrates in lungs and chest CT scan revealed left apical hydropneumothorax, loculated left pleural effusion, pneumomediastinum, and chest wall subcutaneous emphysema. Lung biopsy revealed necrosis. Histopathology examination revealed broad, branching hyphae with sporulation in lung tissue biopsy and bronchoalveolar lavage. Respiratory cultures of lung biopsy and BAL grew rapidly and lactophenol cotton blue tape preps showed broad hyphae with round sporangium and rhizoids between the stolons. The patient was diagnosed with mucormycosis, infection with Rhizomucor, and was treated with Amphotericin B. Surgical debridement of the tissue was not possible due to her declining condition. She passed away after 5 days.
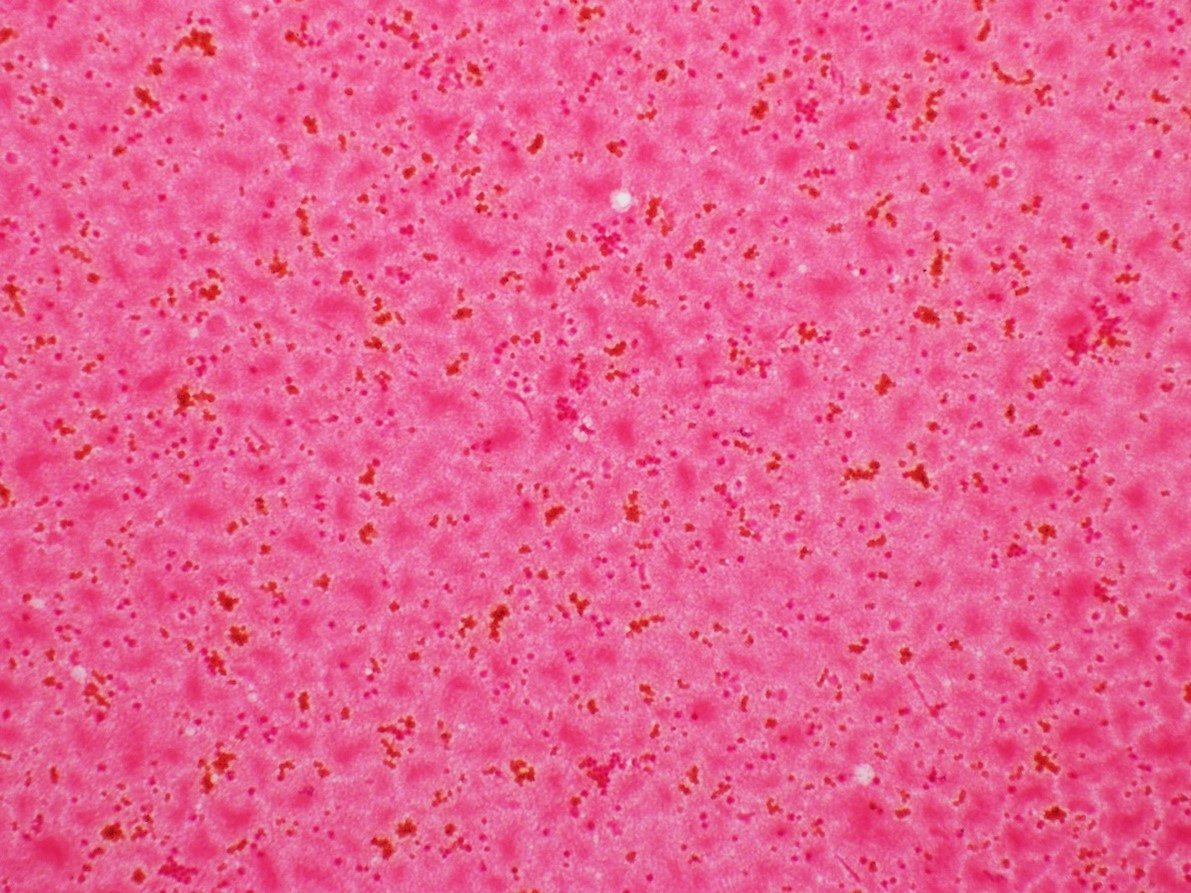
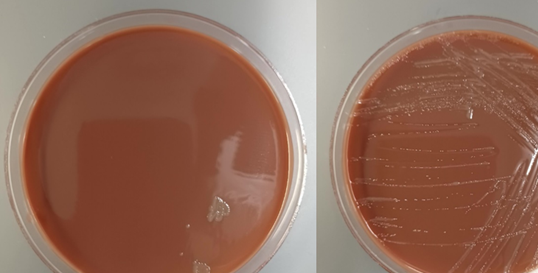
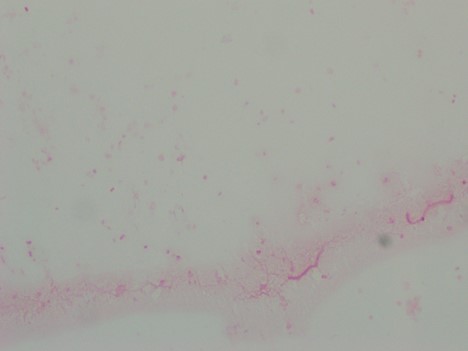
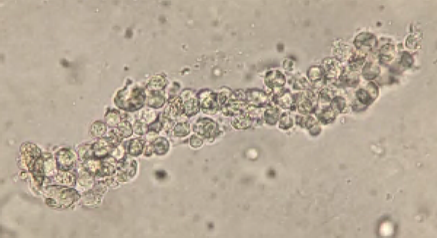
Figure 1. H&E stain of the lung biopsy (top, left) and Papanicolaou stain of bronchoalveolar lavage (top, right) revealed broad, ribbon-like, right-angle branching hyphae (visible in lung biopsy) with sporulation (credits to Dr. Elham Arbzadeh, George Washington University School of Medicine and Health Sciences). Rapid growth was observed from the respiratory cultures of the tissue biopsy by day 2 (bottom, left) where lactophenol cotton blue tape preps showed broad hyphae with sporangium (bottom, right) and intermodal rhizoids (not shown in this image).
Discussion
The term mucormycoses refers to infections caused by the Zygomycetes which is further separated into Mucorales and Entomophthorales. Some of the members of Mucorales are Rhizopus spp., Mucor spp., Lichtheimia (Absidia) spp., Syncephalastrum spp., and Rhizomucor spp.1,2 These organisms live in soil, dung, and vegetative matter. Infection is usually acquired by inhalation/ingestion of their spores or direct inoculation and contamination of wounds. The mold can invade the walls of the blood vessels causing angioinvasion and often results in dissemination of mycotic thrombi and development of systemic infection. Zygomycetes are most commonly known for causing rhinocerebral, pulmonary, cutaneous, and disseminated disease. Infections with Zygomycetes most commonly occur as opportunistic infections in immunocompromised hosts. Risk factors include diabetes, those with acidosis, neutropenia, and sustained immunosuppression such as after transplantation.
Zygomycetes grow very fast (within 48 to 72 hrs.) and is often called a “lid lifter”. The colonies have a wooly mycelium and can be described as cotton candy-like. Lactophenol tape preps of the mold would reveal broad hyphae, aseptate or pauciseptate, ribbon-like hyphae with irregular width. At the tip of the sporangiophore, there is a sack-like structure called a sporangia with contains all the spores. Fungal elements and hyphae seen on tissue biopsies from patients with mucormycosis typically have near right angle branching (usually >40o) broad, non-septate hyphae. In contrary, those with aspergillosis show acute angle branching (usually <45o) with narrow, septate hyphae.3
Genus-level identification can be achieved by microscopic morphology. Rhizomucor is an intermediate between Rhizopus and Mucor. Rhizoids found in Rhizomucor are few in number and are located on stolons, between the sporangiophores, as opposed to Rhizopus where the rhizoids are often seen directly at the nodes and Mucor which does not produce rhizoids. Sporangia (40-80 µm in diameter) are brown in color and round in shape. Apophysis is absent, which allows for differentiation from Lichtheimia (Absidia) where apophysis can be seen.4 The genus Rhizomucor includes three species: Rhizomucor pusillus, Rhizomucor miehei, and Rhizomucor tauricus.5
Treatment of mucormycosis consists of antifungal and surgical therapy. Amphotericin B is the most commonly used antifungal agent. Liposomal amphotericin B has also been successfully used in some cases with zygomycosis due to Rhizomucor.6 Early diagnosis and treatment are crucial and mortality rate is high.7 Of note, Zygomycetes are intrinsically resistant to voriconazole.
References
Rippon J W. Medical mycology. The pathogenic fungi and the pathogenic actinomycetes. Philadelphia, Pa: Saunders; 1974. Mucormycosis; pp. 430–447.
Scholer H J, Müller E. Beziehungen zwischen biochemischer Leistung und Morphologie bei Pilzen aus der Familie der Mucoraceen. Pathol Microbiol. 1966;29:730–741.
Mohindra S., Mohindra S., Gupta, R., Bakshi, J., Gupta, S. K. Rhinocerebral mucormycosis: the disease spectrum in 27 patients. Mycoses. doi: 10.1111/j.1439-0507.2007.01364.x.
de Hoog, G. S., J. Guarro, J. Gene, and M. J. Figueras. 2000. Atlas of Clinical Fungi, 2nd ed, vol. 1. Centraalbureau voor Schimmelcultures, Utrecht, The Netherlands)
Schipper M A A. On the genera Rhizomucor and Parasitella. Stud Mycol. 1978;17:53–71.
Bjorkholm, M., G. Runarsson, F. Celsing, M. Kalin, B. Petrini, and P. Engervall. 2001. Liposomal amphotericin B and surgery in the successful treatment of invasive pulmonary mucormycosis in a patient with acute T- lymphoblastic leukemia. Scand J Infec Dis. 33:316-319.
Ribes, J. A., C. L. Vanover-Sams, and D. J. Baker. 2000. Zygomycetes in human disease. Clin Microbiol Rev. 13:236-301.
-Maryam Mehdipour Dalivand, MD is a Pathology Resident (PGY-1) at The George Washington University Hospital. She is pursuing AP/CP training.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
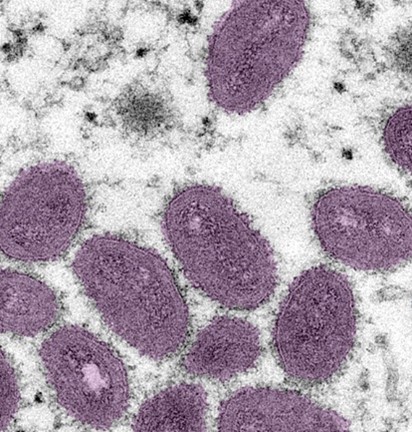
I have been hearing many concerned questions about Monkeypox lately, and I wanted to add onto the great job already done by Dan Scungio in his previous post on how laboratorians should be safe around Monkey pox suspected samples. As a part of the queer community, I’ve heard from several people who are very concerned as this is predominately spread among men who have sex with men. I’ll be focusing on what is new about Monkeypox, how it is different, where it is spreading, and what can be done about it so far. I’ll address questions like should we be sequencing Monkeypox like COVID-19 and does your smallpox vaccination will protect you.
What is Monkey Pox?
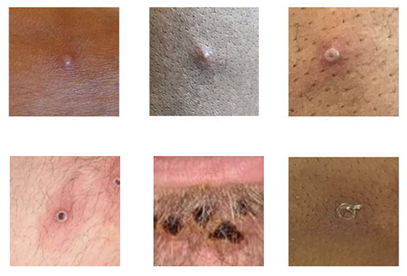
This is an orthopox virus that is from the same family as smallpox, which was so effectively cleared from human circulation that vaccines were discontinued in the U.S. in the early 1980’s. It causes a systemic disease characterized by lesions that start as a red, flat rash (macula) then form vesicles that break open, crust and resolve in 2-4 weeks. If you ever had chicken pox, you may recall how painful it was, and this is the major symptom that requires medical management.
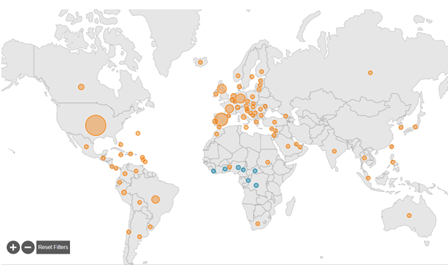
Initially case increases were attributed to undiagnosed disease just as happened with COVID-19 initially. However, now that commercial labs are testing for it and access to testing is not an issue, we still see case counts increasing. This indicates that the rapid spread is real and concerning. That rapid spread is one reason that it has now been declared a national public health emergency.
How is it tested for?
Initially testing was sent out to one of the CDC regional testing centers. However, there were only 60-70 of these sites and they had limited capacity for high throughput testing. Then Labcorp and Quest they can each perform PCR testing, which has expanded access greatly. However they have different specimen types they accept:
Labcorp: Lesion swab in VTM sent frozen or refrigerated (room temp not acceptable)
Quest: Lesion swab in VTM
What is new?
It has been in Sub-Saharan Africa for a long time.
Early summer it began to spread into other continents like Europe.
U.S. now has the highest levels of Monkeypox cases.
This all reinforces the impact of communicable diseases in a global society.
Thornhill JP, et al. Monkeypox Virus Infection in Humans across 16 Countries — April–June 2022. NEJM. July 2022. DOI: 10.1056/NEJMoa2207323
–Jeff SoRelle, MD is Assistant Instructor of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX working in the Next Generation Sequencing lab. His clinical research interests include understanding how lab medicine impacts transgender healthcare and improving genetic variant interpretation.Follow him on Twitter @Jeff_SoRelle.
During the warmer months here in the Midwest, ticks are abundant and our microbiology lab receives several tick submissions per day for identification. When possible, we provide species level identification as well as sex for any tick submitted. While this is common practice in most microbiology laboratories, our molecular laboratory accidently received a tick specimen and, in the process of routing it to the microbiology lab, was curious as to why the tick identification matters—what does that tell us clinically? This led to an impromptu plate rounds with both labs and prompted me to write this post.
How do we determine tick identity?
A tick is submitted in a cup and sent to the laboratory. Ideally the tick would be submitted whole without missing appendages or damaged in any way. The tick is placed in ethanol to kill the organism and to allow for examination under a microscope. The mouth parts, scutum, and festoons are examined for defining features. Thorough examination is challenging when the tick arrives damaged or only partially intact.
Why do we provide tick identification?
Certain ticks carry specific pathogens. For instance, Amblyomma americanum (lone star tick) can transmit ehrlichiosis, Francisella tularensis, Heartland virus, Bourbon virus, and Southern tick-associated rash illness, while Ixodes scapularis can transmit Borrelia burgdorferi & Borrelia mayonii (both are causative agents of Lyme disease), Anaplasma phagocytophilum, and Erhlicia muris as well as Powassan virus. Knowing which tick that the patient was bitten by can allow providers to understand what potential pathogens they may or may not have been exposed to. If Amblyomma americanum is submitted, for example, that tick does not carry Borrelia burgdorferi. However, it is important to note that the majority of patients who develop tick-borne illness have no recollection of a tick bite! So while one tick may be discovered and sent to the lab, the patient could still have been unknowingly bitten by a different tick, which could carry other pathogens. When a patient exhibits clinical symptoms that are consistent with a tick-borne disease, such as Lyme Disease, the patient should be tested for that disease regardless of their tick history.
The patient has an Ixodes tick! They are worried about Lyme Disease. Should we send the tick out for molecular testing?
We discourage the use of molecular testing on the ticks themselves because ticks carry a variety of pathogens and there is a high likelihood of carrying a particular pathogen in a high prevalence area. For Ixodes ticks in Lyme Disease endemic areas, 15-70% of ticks may carry the causative agent, Borrelia burgdorferi. However, just because a tick carries a particular pathogen, it does not mean that the patient is now infected. This can lead to unnecessary treatment and misdiagnosis. Moreover, ticks must feed for a certain amount of time before pathogens can be transmitted. For example, Ixodes ticks must typically feed for more than 24 hours before it can transmit Lyme Disease or other pathogens.
Image 1. A male Dermacentor variabilis (also known as the American dog tick) submitted by one of our patients.
In summary, tick identification can provide a glimpse into what the patient was potentially exposed to and if symptoms do arise days to weeks later, the tick identification may offer additional clues. However, just because a person was bitten by a tick does not mean that they are infected. Identification is just a piece of the puzzle!
References
Blaine A. Mathison and Sam R. Telford III, 2019. Arthropods of Medical Importance, In: Carroll KC, Pfaller MA Manual of Clinical Microbiology, 12th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.MCM.ch151
Bobbi Pritt, and J. Stephen Dumler, 2019. Ehrlichia, Anaplasma, and Related Intracellular Bacteria, In: Carroll KC, Pfaller MA Manual of Clinical Microbiology, 12th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.MCM.ch67
Blaine A Mathison, 2021. 9.11 Gross Examination of Helminths and Arthropods, Leber ALClinical Microbiology Procedures Handbook, 4th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.CMPH.ch9.11
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
While writing my last blog, I asked “What is your least favorite test to do in Hematology?” (I’m not ignoring our favorite tests! I will get to those in another blog.) And then, I started thinking about why we may not like certain testing. Is it because they are time consuming, or repetitive? Is it because they hurt our eyes, or necks, or fingers? Or is it because it’s a test that we perform but we may not be sure what the test is for, or we don’t understand the theory behind it? I started thinking about my coworkers and other tests that could be on those lists and I immediately decided that a good candidate in our lab is the T4T8 panel. Probably the primary reason is that the instrument we do these on has given us many problems over the last year. The instrument has spent most of the year with an “instrument out of service” sign on it. Service has been here many times, but the instrument just appears to have exceeded its life expectancy. In normal times, when the instrument was in its prime, setting up and running a T4T8 panel does require a number of steps, and some time. In the last year we have had to add lots of coaxing, even more time, and some luck to get the test to run. This can be frustrating in any lab situation, but is particularly frustrating when we are short staffed, trying to train new staff, and very busy. So, I don’t think it’s the test itself that techs dislike, it’s the time it takes, not being comfortable with setting up the test, juggling our other work while struggling with another instrument, and the fact that even after we get results, a percentage of the samples have results that don’t meet our criteria and still need to be sent out to the reference lab.
Another reason why this test may be a little intimidating is its unfamiliarity. It’s not a test that is done in every lab. I have worked as a Medical Laboratory Scientist for many years. I’ve worked in 6 labs since the mid 1980’s and the introduction of CD4 testing for human immunodeficiency virus (HIV) patients, yet my current place of work is the first place that we have done these in house. Before this job, if you asked me or any of my coworkers what a T4T8 panel was, we probably would have answered “a send out test”. A few weeks ago, we had a call from a doctor asking questions about his patient’s T4T8 assay results. The tech answering the phone got a blank look on their face and quickly handed the phone to me. This told me that techs, and even doctors, may not really understand what this test is testing and what the results mean. This further confirmed to me that the lack of knowledge about these tests may be another reason why these don’t win any popularity contests in our lab.
So, what exactly is a T4T8 panel?
Some other names for the test are a Lymphocyte subset panel, an Immuno T-cell (CD3/4/8) assay, T-Cell subsets Percent and Absolute panel or T-Lymphocyte Helper/Suppressor Panel. As a quick review, we know that lymphocytes are either B-lymphocytes or T-lymphocytes. Immunotyping lymphocytes can provide information for disease diagnosis and monitoring. All T-lymphocytes express CD3 antigens on their surfaces, which can be used to differentiate B-cell disorders from T-cell disorders. T-lymphocyte subsets include T-helper/inducer cells which express both CD3 and CD4, and T-cytotoxic/suppressor cells, which express CD3 and CD8. In a T4T8 panel we are concerned with identifying T-lymphocytes, and the percentage of each subset both individually, and compared to one another.
The test we perform uses monoclonal antibodies, anti CD3, anti CD4 and anti CD8, which recognize specific human lymphocyte subsets. Our reagents come as antibody containing tubes and are run on the Cell-Dyn Sapphire. After performing a CBC on the sample, the instrument is programmed to add an aliquot of the sample to the CD3 +CD4 reagent tube and a second aliquot to the CD3 + CD8 reagent tube. Immunophenotyping is performed by flow cytometry on these 2 aliquot tubes. The CD3 antibody in both tubes separates out all T-lymphocytes, and the addition of the CD4 in the first tube identifies the cells which are also CD4 positive, the T4 or helper cells. The CD3 + CD8 tubes identifies the percentage of T cells that are T8 or suppressor cells. The assay uses the CBC results and the immunophenotyping runs to calculate the helper/suppressor ratio, also known as T4/T8 ratio or CD4/CD8 ratio.
Why is this test performed?
After the discovery of lymphocyte subset abnormalities in human immunodeficiency virus (HIV) patients in the 1980s, lymphocyte immunophenotyping has become widely used in this patient population for the evaluation of their prognosis, immune deficiency status, response to therapy, and diagnosis of AIDS. The test is most often done to assess HIV infection status but may also be useful in the diagnosis and monitoring of other diseases or after organ transplantation. Some examples of conditions in which this assay may be useful include other viral and bacterial infections, severe combined immunodeficiency, Hodgkin disease, certain leukemias, multiple sclerosis, and myasthenia gravis. A newer application of CD4/CD8 ratios are as potential biomarkers of cancer progression. The most interesting new use of T-cell subset testing that I have read about has been with the recent COVID-19 pandemic. Several studies have shown that CD4 and CD8 T- cell counts reflected disease severity and can predict clinical outcomes of COVID-19 infection. These studies have concluded that COVID-19 patients presenting with relatively low CD4 and CD8 T-cell counts are more severely infected and may have a worse prognosis. The Abbott test we use was designed to be used to monitor immune status in (HIV)-infected individuals. It is not intended for screening for leukemic cells or for phenotyping samples in leukemia patients.
What do the results mean?
The absolute CD4 count and CD4/CD8 Ratio can be used as a snapshot of immune system health. Normal absolute CD4 counts are 600 to 1200 /mm3. In immune suppression, values drop below 500/mm3 and in advanced infection, values of less than 200/mm3 are consistent with a definition of acquired immunodeficiency syndrome (AIDS). In advanced disease, some patients may have a normal CD4 count but experience a weakening immune system. Or the immune system can become exhausted and unable to produce sufficient T-cells. The CD4/CD8 ratio is useful for judging the strength of the immune system. A normal CD4/CD8 ratio is between 1.0 and about 3.0-4.0.
T-helper cells start the defensive immune response by signaling other cells that infectious pathogens are present. At initial infection with HIV, T-suppressor cells increase in an effort to destroy infected cells. We see an increase in CD8 cells as the CD4 cells are destroyed. These events result in a low CD4/CD8 ratio. When HIV antiretroviral therapy (ART) is initiated, the ratio will usually, gradually return to normal. However, if ART is not started or if the immune system is severely affected, the body may not be able to make adequate new CD4 cells and the ratio may never return to normal.
With the availability of very effective therapies available for the treatment of HIV, the CD4/CD8 ratio has become more important in patients with long term HIV infection. Recent studies have suggested that people with a low CD4/CD8 ratio who have been on treatment for years are at an increased risk from non-HIV illnesses such as cardiovascular and renal disease.
CD4 counts are important in HIV management and used to guide treatment including the decision to initiate prophylactic treatment against opportunistic infections. It is recommended that CD4 counts be performed every 3-6 months after initiation of ART. After the first 2 years on ART, CD4 monitoring can be decreased in frequency to every 12 months for people whose CD4 count is between 300 and 500 and may be considered optional for those with CD4 counts over 500. Table 1 and 2 shown below are examples of patient reports for the T4T8 assay.
Table 1. Patient with AIDS, CD4 count 200, T4/T8 ratio 0.16*Table 2. Patient with absolute CD4 within normal range, but CD4/CD8 below 1.0*
*There are times when the absolute or % CD3T may be less than the sum of the CD4T and CD8T. This is due to averaging of CD3T counts from the 2 monoclonal tubes
In our lab, these tests are performed daily, as they are received, from 7am to 7PM, 7 days a week. There are no commercial quality control materials available for the test, so we must choose negative and positive QC from our patient population. For the QC we choose patients with CBC and WBC differential values within normal ranges, with no flags. There are additional age and diagnosis/treatment related restrictions on samples that can be used as controls. Our in-house patients often have abnormal results, and our patient population also includes our large outpatient hematology/oncology center. Thus, at times, finding appropriate controls can be challenging. I can add this to the list of ‘problems’ with this test and why techs don’t like them. Call me weird, but I actually like doing these! I like the challenge of finding QC, I like that they are ‘different’ from the hundreds of CBCs we perform each day, and I look at them as a little change in routine and a chance to do something unique. Though I wish the instrument would run perfectly every day, I even (sort of) don’t mind troubleshooting when it’s not working. I like solving problems! I enjoy teaching others how to run these, and I enjoy answering questions about the test.
Many thanks to my great coworker Jacky Olive for her assistance always and inspiration for this blog. I know these are not your favorite test!
*There are times when the absolute or % CD3T may be less than the sum of the CD4T and CD8T. This is due to averaging of CD3T counts from the 2 monoclonal tubes
Li Raymund; Duffee Doug; Gbadamosi-Akindele Maryam F.CD4 Count. NIH National Library of Medicine. May 8, 2022
Domínguez-Domínguez L, Rava M, Bisbal O, et al. Cohort of the Spanish HIV/AIDS Research Network (CoRIS). Low CD4/CD8 ratio is associated with increased morbidity and mortality in late and non-late presenters: results from a multicentre cohort study, 2004-2018. BMC Infect Dis. 2022 Apr 15;22(1):379.
Liu Z, Long W, Tu M et al. Lymphocyte subset (CD4+, CD8+) counts reflect the severity of infection and predict the clinical outcomes in patients with COVID-19. Journal of Infection. Vol 81, Issue 2. P318-356, AUGUST 01, 2020
Kagan JM, Sanchez AM, Landay A, Denny TN. A Brief Chronicle of CD4 as a Biomarker for HIV/AIDS: A Tribute to the Memory of John L. Fahey. For Immunopathol Dis Therap. 2015;6(1-2):55-64
McBride JA, Striker R (2017) Imbalance in the game of T cells: What can the CD4/CD8 T-cell ratio tell us about HIV and health? PLoS Pathog 13(11)
Sinha A, Mystakelis H, Rivera AS, Manion M, et al. Association of Low CD4/CD8 Ratio With Adverse Cardiac Mechanics in Lymphopenic HIV-Infected Adults. J Acquir Immune Defic Syndr. 2020 Dec 1;85(4)
Wang YY, Zhou N, Liu HS, Gong XL, Zhu R, Li XY, Sun Z, Zong XH, Li NN, Meng CT, Bai CM, Li TS. Circulating activated lymphocyte subsets as potential blood biomarkers of cancer progression. Cancer Med. 2020 Jul;9(14)
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A patient with no previous cancer history presented to the Head and Neck Clinic after imaging performed for radial nerve palsy detected multiple (4) thyroid nodules. The 1.9 centimeter isthmus nodule met biopsy criteria due to its size, hypoechogenicity, solid composition, and punctate echogenic foci, placing the nodule into a TI-RADS risk category of TR5. An ultrasound-guided fine needle aspiration (FNA) was performed, and Rapid Onsite Evaluation (ROSE) determined that the sample contained atypical follicular cells. Two additional passes were collected in Veracyte Afirma fixative to be reflexed for a Gene Sequencing Classifier in the event of an indeterminate final diagnosis, such as follicular lesion of undetermined significance (FLUS), atypia of undetermined significance (AUS), or suspicious for follicular neoplasm. The Diff-Quik smears, featuring nuclear inclusions and papillary formations, are presented below.
The following day, the Pap-stained smears demonstrated more pronounced cytologic features of papillary thyroid carcinoma, including nuclear invaginations, nuclear grooves, papillary clusters, and limited colloid. Rare tumor cells were also identified on cell block sections (not shown), and immunohistochemical (IHC) stains showed that the cells of interest were positive for thyroglobulin and TTF-1. Although there were a few pleomorphic and histiocytic areas on the smears which appeared different than classic papillary thyroid carcinoma, the thyroid isthmus FNA was signed out as papillary thyroid carcinoma (Bethesda Category VI), and correlation with clinical and radiological findings was recommended.
Due to the final cytology diagnosis, the patient was scheduled for a total thyroidectomy and possible neck lymph node dissection within three weeks of the initial biopsy. During the total thyroidectomy, the 2 centimeter isthmus nodule was noted, and there was no gross evidence of extrathyroidal extension or suspicious lymphadenopathy, as this was diagnosed as non-invasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP). Adjacent to the NIFTP, but still within the isthmus, was a 1.6 cm hyalinizing trabecular tumor, which alludes to the other cells of interest identified on the FNA smears. No tumor was identified in three lymph nodes, and a less than 0.1 cm incidental micropapillary thyroid carcinoma (follicular variant) was found. The margins were negative for all three elements.
IHC was performed on the dominant isthmus nodule showing that the tumor cells are positive for TTF-1, thyroglobulin, and PAX-8, while negative for calcitonin. Ki-67/MIB1 at 37 degrees Celsius demonstrated no membranous staining, supporting the diagnosis of NIFTP. The same stains were performed on the neighboring 1.6 isthmus tumor with all of the immunostains yielding the same results, except positivity in Ki-67/MIB1. This single stain differentiates a diagnosis of hyalinizing trabecular tumor, a very rare (less than 1%) follicular-derived thyroid tumor that has strikingly similar features to papillary thyroid carcinoma and NIFTP.1 While hyalinizing trabecular tumors are typically a histologic diagnosis due to the solid trabecular growth pattern, hyalinization of extracellular spaces and lack of vascular or capsular invasion, careful cytologic analysis could postulate the presence of this tumor especially in FNAs that do not demonstrate classic papillary thyroid carcinoma features.1 It is important to note, especially in hindsight thanks to this case, that the histiocytic cells identified on the FNA smears had elongated nuclei with abundant cytoplasm and cells radially arranged around hyaline globules. While nuclear grooves and intranuclear inclusions are prominent in both tumors, the nuclear shape and presence of hyaline can help cytologists morphologically distinguish between papillary thyroid carcinoma and hyalinizing trabecular tumors and trigger the inclusion of MIB1 IHC staining (LiVolsi, 2022).
-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
A 47 year old male with an extensive ocular history including laser assisted in situ keratomileusis (LASIK), multiple ocular traumas with repair, and myopic degeneration with neovascularization for which he was prescribed hard and soft contact lenses presented for bilateral eye redness, watering, and stinging pain. Recently, he had forgotten his soft contacts and wore his hard lenses to his job in construction which he reported doing once every 1-2 months. Ocular exam revealed only his usual chronic changes. His symptoms improved with moxifloxacin eyedrops, but never fully resolved. A month later he returned with what was initially assessed as diffuse corneal edema and conjunctival injection in his left eye, but no ring infiltrate or epithelial defect. Two days later, a large epithelial defect with surrounding ring infiltrate and hypopyon (settling of white blood cells at the base of the anterior chamber) developed in his left eye. Confocal microscopy showed findings concerning for Acanthamoeba infection and the contact lenses and case were sent for culture. Environmental organisms including Klebsiella varicola, Chryseobacterium gleum, and Pseudomonas fluorescens were recovered. In addition, cultures for Acanthamoeba sp., where sample is overlaid on a lawn of E. coli grown on a non-nutrient agar plate, were sent to a reference laboratory.
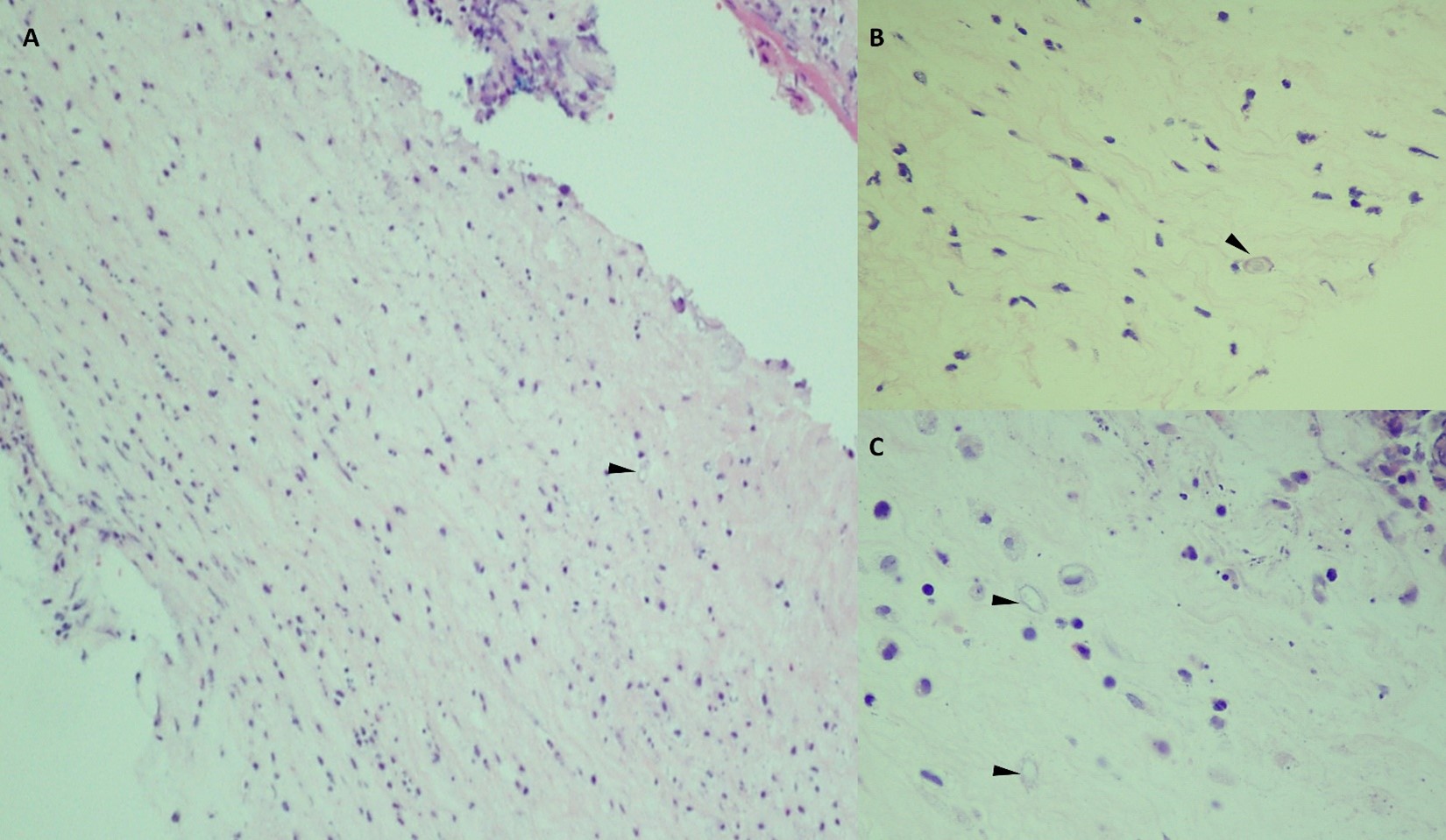
The patient was treated with Brolene, polyhexamide biguanide (PHMB), and chlorhexidine for Acanthamoeba as well as with antibacterial agents. Three months later his LASIK flap failed and was removed and sent for cultures and pathology which both grew Acanthamoeba sp.(Image 1). He continued treatment for another two months, but the corneal defect expanded. He underwent a therapeutic penetrating keratoplasty, and the explant cornea was sent for pathology. Sections showed acute and chronic inflammation of the corneal epithelium and stroma with rare cysts of Acanthamoeba with atypical morphology possibly representing treatment effect or nonviable organisms (Image 2). The patient continued treatment for another month afterward with resolution of symptoms.
Image 1. Representative photomicrographs of cornea with multiple Acanthamoeba cyst forms at differing stages of development (H&E, 400x magnification) and trophozoite with associated acute inflammation (inset, 500x magnification, oil immersion).Image 2. Photomicrograph of this patient’s explanted LASIK flap. A) Low power magnification demonstrating acute and chronic inflammation in a background of degrading corneal tissue. An empty cyst is highlighted by the arrowhead (H&E, 100x magnification). B and C) High power magnification of likely nonviable cysts indicated by the arrowheads (H&E, 400x magnification).
Discussion
Acanthamoeba sp. are free-living amoebae found ubiquitously in the environment including in water, soil, dust, and air conditioning ducts.1 Over 20 species of Acanthamoeba have been identified, with eight known to cause human disease. A. castellani and A. polyphaga are the most common species identified from clinical infections.2Acanthamoeba sp. are a primary reservoir of Legionella pneumophilia and can serve as vectors for other bacterial infections.3 These organisms may colonize the nasal passages of normal hosts.4 Acanthamoebal infections have varied clinical presentations depending on the route of transmission, organ(s) infected, and immune status of the host. These include amebic keratitis, granulomatous amebic encephalitis, and disseminated disease.3 Of these, Acanthamoeba keratitis (AK) is the most frequently encountered clinically.
AK can occur when the organisms are inoculated into corneal micro-abrasions, most often from contaminated hard contact lenses rinsed with tap water. AK represents 5% of all cases of contact-lens-associated keratitis, and 70-85% of AK cases are associated with contact lens use.1 Diagnosis of AK is heavily dependent on a high index of suspicion as AK presents with nonspecific ocular symptomology including blurred vision, photophobia, inflammation, and eye pain. A corneal ring infiltrate is characteristic, but only present in 50% of cases.1 Although historically culture is the gold standard for diagnosis, advanced technologies like confocal microscopy and PCR have greatly improved sensitivity and time to diagnosis.5 Cultures are usually grown on agar plates coated with gram negative bacilli such as E. coli.2 If Acanthamoeba are present, trails of bacterial clearing can usually be seen within days but may take up to several weeks.2 They have dormant cyst and active trophozoite forms. Microscopically they appear as round heterogeneous bodies with a distinct nucleus and surrounded by ruffled membrane and are 15-35 μm in length.3 PCR, given its analytical sensitivity, specificity and turn around time, is the more common method of diagnosis of AK and has replaced many instances of culture today.
AK has a poor prognosis and is potentially sight threatening. Factors contributing to disease severity include delayed diagnosis, pathogenic factors, and lack of effective medical management.1 Nearly 40% of patients fail initial therapy.1 Factors that contribute to Acanthamoeba pathogenicity include production of enzymes including elastases and proteases, adhesion molecules, and physiologic tolerance to different temperatures, osmolarities, and pH.6 The cyst stage confers resilience to many therapies which is compounded by poor tissue penetration of the antimicrobial agents often used in therapy.6 Repeated exposure to therapeutic antimicrobials can also lead to the development of resistance.6 In our patient’s case, treatment was successful following the LASIK flap removal, facilitating increased drug penetration and supported by pathologic findings of treatment effect in the explanted cornea.
References
Somani SN, Ronquillo Y, Moshirfar M. Acanthamoeba Keratitis. 2021 Aug 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 31751053.
Maycock NJ, Jayaswal R. Update on Acanthamoeba Keratitis: Diagnosis, Treatment, and Outcomes. Cornea. 2016 May;35(5):713-20. doi: 10.1097/ICO.0000000000000804. PMID: 26989955.
Marciano-Cabral F, Cabral G. Acanthamoeba sp. as agents of disease in humans. Clin Microbiol Rev. 2003 Apr;16(2):273-307. doi: 10.1128/CMR.16.2.273-307.2003. PMID: 12692099; PMCID: PMC153146.
Clarke B, Sinha A, Parmar DN, Sykakis E. Advances in the diagnosis and treatment of Acanthamoeba keratitis. J Ophthalmol. 2012;2012:484892. doi: 10.1155/2012/484892. PMID: 23304449; PMCID: PMC3529450.
Hoffman, J.J., Dart, J.K.G., De, S.K. et al. Comparison of culture, confocal microscopy and PCR in routine hospital use for microbial keratitis diagnosis. Eye (2021). https://doi.org/10.1038/s41433-021-01812-7
Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10. doi: 10.1051/parasite/2015010. PMID: 25687209; PMCID: PMC4330640.
-Tim Kirtek is a fourth year AP/CP resident at UT Southwestern Medical Center in Dallas, Texas.
-Dominick Cavuoti is a professor at UT Southwestern Medical Center who practices Medical Microbiology, Cytology and Infectious Disease Pathology.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
The monkeypox virus is poorly named. The actual source of the virus is unknown, although it is possible that African rodents and non-human primates (like monkeys) might harbor the virus and infect people. Either way, the virus has entered the United States again recently and has caused new safety concerns for laboratories around the country.
As with the novel Coronavirus pandemic, the monkeypox outbreak has created new safety concerns among laboratorians. How easily can this be transmitted? How should samples be handled or packaged for transport? Will this create a critical lab staffing shortage? How should waste be treated? It is vital that lab leaders and safety professionals answer these questions for staff and relay as much information as possible to allay unnecessary fears.
First, one of the most important areas of focus for laboratorians potentially working with monkeypox patient samples is to continue to utilize Standard Precautions. As always, all specimens in the lab setting need to be treated as if infectious. When handling standard clinical specimens (blood, body fluids, etc.) from suspected monkeypox patients, no extra safety precautions or PPE should be necessary in the lab. The quantity of pox virus likely to be in clinical specimens is low, although procedures that generate aerosols should always be avoided.
Laboratory staff should also be trained to package and ship Category B specimens. The current West African strain (clade) of monkeypox in the U.S. is not considered Category A under the Hazardous Materials Regulations (HMR), so monkeypox swab specimens for virus testing should be shipped similarly to other clinical specimens. Use the packaging kit and follow the instructions from the receiving testing lab.
There may be concerns about the spread of monkeypox infection among employees in the laboratory. Any infected employee should be using PPE when working in the department, and the monkeypox virus is only spread by close physical contact, direct contact with the infectious rash, scabs, or body fluids, and touching items (such as clothing or linens) that previously touched the infectious rash or body fluids. If there was contact with infected PPE or if an employee had prolonged face-to-face contact with an infected co-worker, that should be reported. The CDC states that monkeypox can spread from the time symptoms start until the rash has fully healed and a fresh layer of skin has formed. The illness typically lasts 2-4 weeks. People who do not have monkeypox symptoms cannot spread the virus to others. Direct any concerns to the employee health practitioners.
Laboratories should have an emergency management plan in place which includes how to handle staffing shortages. That plan may include sending routine testing to an alternate location, using point-of-care testing or reducing services to a limited test menu. In most laboratories, however, this monkeypox outbreak is unlikely to create a massive staffing outage. The virus does not spread quickly or in public, and a pandemic of monkeypox is not expected.
Handling monkeypox waste is another consideration for laboratories. Normally, the waste associated with monkeypox virus is considered a Category A waste (waste contaminated with a known highly infectious substance). However, waste from patients infected with the current West African strain of monkeypox is considered exempt from the category A Infectious Substance Regulations according to the Department of Transportation. It can be managed as regulated medical waste. Soiled laundry, including lab coats, should never be shaken or handled in manner that may disperse infectious particles. Laundry should be contained (bagged) at the point of use. Organizations should contact their local public health authority for more information if needed. As the past few years have shown, new threats will continue to emerge, and they will raise safety questions in the laboratory. As always, laboratorians should stay vigilant, pay attention to the work they do every day to avoid injuries and exposures when handling any specimens. Communicate with the hospital departments to ensure proper internal specimen transport of clinical and diagnostic (swab) specimens. Handling laboratory specimens has never been monkey business- the use of Standard Precautions and safe work practices will keep employees safe through this outbreak, and for whatever comes next.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A 75 year old female with a past medical history of coronary artery disease, hypertension, pre-diabetes mellitus, chronic obstructive pulmonary disease, prior left lobe cavitary lesion of unknown etiology, and tobacco use presented to the ED after being found nonresponsive on the couch. Family reports the patient said she had emesis the night before and felt as if she had a “stomach bug”. MRI shows T2 hyperintensities in the right MCA distribution. CSF results as follows.
White Blood Cells
300
Red Blood Cells
12
Protein
990
Glucose
79
Cryptococcal antigen
Negative
Fungal culture
No fungi isolated
HSV
Negative
Laboratory findings
CSF was sent to the microbiology lab for bacterial and fungal smears and cultures. No fungi were identified. Cryptococcal antigen was negative. HSV was also negative. CSF Gram stain shows gram positive bacilli. CSF culture showed a small, white, smooth, translucent appearance on sheep blood agar. In semi-solid agar after overnight incubation at room temperature, an umbrella shaped pattern of motility was seen. The organism was identified as Listeria monocytogenes by MALDI-TOF mass spectrometry.
Image 1. Listeria monocytogenes on sheep blood agar. Image 2. Listeria monocytogenes showing “umbrella zone” pattern of motility on semi-solid agar.
Discussion
Listeria spp. is a genus of gram positive, aerobic, facultative intracellular, catalase positive bacteria. Listeria monocytogenes is a common colonizer in the environment (animals, soil, vegetable matter) and occasionally colonizes the human gastrointestinal tract. Listeria prefers colder environments and can be found as a food contaminant, most notably in milk, raw vegetables, cheese, and meats. In addition, colonized mothers can pass Listeria monocytogenes to the fetus.1
Listeria monocytogenes has 3 notable virulence factors:2
Listeriololysin O: a hemolytic toxin that allows for survival within phagocytes
Act A: induces actin polymerization that facilitate cell-to-cell spread
Siderophores: organisms capable of scavenging iron from human transferrin to enhance cell growth
Neonates, immunocompromised individuals, and the elderly are more likely to acquire infection. Infection can present as bacteremia and CNS infections including meningitis, encephalitis, brain abscesses, and spinal cord infections. Listeria monocytogenes is the 3rd most common cause of meningitis behind Streptococcus pneumoniae and Neisseria Meningitidis. In neonates, an in-utero infection can cause granulomatous infantisepticum leading to systemic infection and stillbirth.3Listeria monocytogenes can also present as gastroenteritis.
References
Allerberger F. Listeria: growth, phenotypic differentiation and molecular microbiology. FEMS Immunol Med Microbiol. 2003;35(3):183-189. doi:10.1016/S0928-8244(02)00447-9
Engelen-Lee JY, Koopmans MM, Brouwer MC, Aronica E, van de Beek D. Histopathology of Listeria Meningitis. Journal of Neuropathology & Experimental Neurology. 2018;77(10):950-957. doi:10.1093/jnen/nly077
-Nicholas Taylor, DO is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
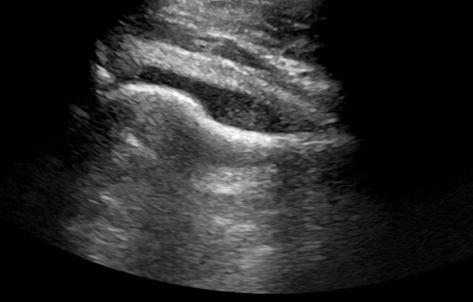
A young man presented to the emergency department with the primary complaint of severe right hip pain persisting for 2 days. This pain began after standing uncomfortably for hours at an event. His right hip was tender to palpation with some erythema and swelling. He had no recent fall or known injury. He denied recent fever, chills, aches, constipation, diarrhea, changes in urinary habits, chest pain, and shortness of breath. An ultrasound (US) of the right hip joint showed moderate amount of effusion (Image 1). Laboratory results also showed an elevated white blood cell count (WBC).
Image 1. US of the right hip joint showing moderate effusion.
The patient underwent incision and drainage of his right hip to relieve the swelling, and samples were collected for Gram stain and aerobic and anaerobic bacterial culture. Blood was also collected from two separate sites for culture. The blood cultures showed no growth following 5 days of incubation. Gram stain of the effusion showed 4+ WBC with no organisms seen (Image 2). The joint fluid was set up for aerobic and anaerobic bacterial culture. Anaerobic bacterial culture showed no organism growth. However, a few small, grey-ish mucoid colonies grew in the first quadrant on Chocolate agar in the aerobic culture (Image 3). Gram stain was performed on one of the colonies (Image 4). MALDI-TOF confirmed the identification of Neisseria gonorrhoeae.
Image 2. Gram stain of effusion obtained from the right hip joint showing increased WBCs. Image 3: Left) Bacterial growth on the Chocolate agar plate. Right) Bacterial growth subcultured on another Chocolate agar plate.Image 4: Gram stain of one of the colonies that grew on the Chocolate agar. The Gram stain showed organisms shaped like coffee-beans.
Discussion
Neisseria gonorrhoeae is a fastidious, gram negative diplococci bacteria that can grow inside neutrophils after surviving phagocytosis. It is oxidase positive and aerobic, and generally transmitted through sexual contact such as vaginal, anal, or oral sex.1,2 After a gonococcal infection has resolved, the patient does not develop immunity to future infections from the bacteria. Reinfection is possible due to its ability to evade the immune system by varying its surface proteins, therefore making it appear novel to the immune system.3 Signs of septic arthritis include chills and fever, pain at the joint, inability to move infected joint, erythema, and swelling.4
Multiple factors increase the risk of septic arthritis, including a systemic blood-borne infection, IV drug use, osteoarthritis, past history of septic arthritis, rheumatoid arthritis, alcoholism, diabetes, HIV, lung or liver disorders, old age, and a suppressed immune system.4 Other forms of gonococcal infection are genitourinary infections, which are the most common, disseminated gonococcemia, and gonococcal ophthalmia neonatorum. Genitourinary infections can be particularly dangerous in women if left untreated, as this can lead to pelvic inflammatory disease that could result in infertility due to scarring of the fallopian tubes.5,6 Gonococcal infections of the eyes are one of the leading cause of blindness in neonates in the United States, but can be successfully prevented through treating the mother with antibiotics before birth and administration of eye drops to the baby at birth.7
Identification of N. gonorrhoeae can be done using Gram stain, aerobic bacterial culture on Chocolate or Modified Thayer-Martin (MTM) agar, or nucleic acid amplification test (NAAT). Testing can be done from a urethral swab, urine sample, or sample of body fluid from the area of suspected infection.8,9 Culture is slow with low recovery rates. In urogenital cases, where there is ample colonization of normal flora, genital flora may outgrow N. gonorrhoeae, reducing its recovery. MTM media is useful because it is a GC agar base that makes it selective for N. gonorrhoeae growth. It contains vancomycin, colistin, nystatin, and trimethoprim lactate, which suppresses growth of most other gramgnegative diplococci, gram negative bacilli, gram positive organisms, and yeast.10 The most common testing methodology for urogenital gonococcal infection is NAAT. Some FDA approved platforms also accept rectal or throat samples, however most only accept those from urogenital sources.11 Also, while NAAT is a quick and sensitive diagnostic test, it has the downside of not being able to distinguish between DNA obtained from living or dead bacteria.12
Intravenous (IV) or intramuscular (IM) ceftriaxone is the preferred treatment choice for N. gonorrhoeae infections. Alternatively, other third generation cephalosporins can be used as well, including cefotaxmine and ceftizoxime. Typically, patients with a beta-lactam allergy have been shown to tolerate ceftriaxone, and those who cannot should undergo desensitization due to its effectiveness against this infection. A single dose of azithromycin or a prescription of doxycycline taken twice daily for a week is usually added to the regimen to cover for a potential Chlamydia trachomatis co-infection. Patients presenting with purulent arthritis should also undergo drainage, either arthroscopically or through multiple joint aspirations.13,14
References:
Ryan, K. J., Ray, G., and Sherris, J. C. (2004). Sherris Medical Microbiology: An introduction to Infectious Diseases, 4th edition. McGraw-Hill Medical.
Levinson, W. (2014). Review of Medical Microbiology and Immunology, 13th edition. McGraw-Hill Medical.
Jennings, L. K. and Krywko. D. M. Pelvic Inflammatory Disease. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499959/.
Castro Ochoa, K. J. and Mendez, M. D. Ophthalmia Neonatorum. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551572/.
Ng, L.-K. and Martin, I. E. The Laboratory Diagnosis of Neisseria gonorrhoeae. Canadian Journal of Infectious Disease and Medical Microbiology. 2005; 16: 1-11. Article ID: 323082.
Van Der Pol, B., Ferrero, D. V., Buck-Barrington, L., Hook 3rd, E., Lenderman, C., Quinn, T., et al. Multicenter evaluation of the BDProbeTec ET system for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male uerthral swabs. J Clin Microbiol. 2001; 39(3): 1008–16.
Workowski, K. A., Bachmann, L. H., Chang, P. A., Johnston, C. M., Muzny, C. A., Park, I., et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021; 70(4): 1-187.
Janssen, K. J., Hoebe, C. J., Dukers-Muijrers, N. H., Eppings, L., Lucchesi, M., and Wolffs. P. F. Viability-PCR Shows That NAAT Detects a High Proportion of DNA from Non-Viable Chlamydia trachomatis. PLoS One. 2016; 11(11): e0165920.
Guillot, X., Delattre, E., Prati, C., and Wendling, D. Destructive septic arthritis of the sternoclavicular joint due to Neisseria gonorrhoeae. Joint Bone Spine. 2012; 79(5): 519-20.
Zaia, B. E. and Soskin, P. N. Images in emergency medicine. Man with severe shoulder pain. Gonococcal arthritis of the shoulder. Ann Emerg Med. 2014; 63(5): 528-71.
-Marika L. Forsythe, MD is a PGY1 Pathology Resident at University of Chicago (NorthShore). Her academic interests include molecular diagnostics and its growing importance in the field of Pathology.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
A 35 year old male with chronic bilateral lower extremity lymphedema due to obesity presented with a one-week history of subjective fevers and malaise with associated left lower extremity pain, swelling and erythema. The left leg was markedly edematous with erythema present above the knee down. The leg was tender to palpation, and multiple ruptured bullae and areas of severe desquamation with excessive serous drainage were observed. Importantly, no areas of purulence were noted (Image 2). A clinical diagnosis of severe non-purulent cellulitis was made, and the patient was admitted for parenteral antibiotic therapy of vancomycin and piperacillin-tazobactam. Necrotizing fasciitis was ruled out based on imaging, and significant clinical improvement was seen after 5 days of intravenous antibiotics. The patient was transitioned to oral therapy with amoxicillin-clavulanic acid and doxycycline for a total of 14 days of antibiotics.
Laboratory Workup
During the admission, urinalysis revealed turbid urine with elevated protein (30 mg/dL), and 2+ blood with 5 RBC/HPF on microscopic examination. Given the presence of protein with microscopic hematuria, causes of glomerulonephritis were investigated. Workup revealed a markedly elevated anti-streptolysin O (ASO) titer of 5310 (0-330) and a total complement (CH50) level of 14, which was low given his age. Urine sediment examination revealed red blood cell casts (Image 3). These clinical and laboratory findings were consistent with post-streptococcal glomerulonephritis (PSGN) due to Streptococcus pyogenes skin and soft tissue infection.
Image 1. Colony appearance and biochemical testing of S. pyogenes. A) Typical gram positive cocci in chains characteristic of streptococci. B) Growth on Sheep’s Blood Agar of small, translucent colonies with a wide zone of beta-hemolysis indicative of S. pyogenes. C) Catalase-negative S. pyogenes (left) compared to catalase-positive S. aureus (right). D) PYR-positive S. pyogenes (left) compared to PYR-negative S. aureus (right).Image 2. Left lower extremity at presentation.Image 3: Red blood cell cast seen in urine sediment.
Discussion
Streptococcus pyogenes are gram positive bacteria that appear in pairs and/or chains by microscopy (Image 1A). In culture, these organisms produce relatively small colonies which elaborate a large zone of beta hemolysis on blood agar plates; colonies are translucent with smooth edges (Image 1B). The beta-hemolytic activity of S. pyogenes is due to the activity of two hemolysins: Streptolysin-S (oxygen-stabile) and Streptolysin-O (oxygen-labile). S. pyogenes is the primary organism which expresses the Lancefield Group A carbohydrate antigen. Less frequently encountered strains of S. anginosus and S. dysgalactiae subsp. equisimilis may also express this antigen, so biochemical identification of S. pyogenes may be helpful for a definitive diagnosis. MALDI-TOF MS may also fail to discriminate between S. pyogenes and closely related β-hemolytic streptococci (including S. dysgalactiae and S. canis), necessitating adjunctive biochemical testing. Like other streptococci, S. pyogenes is catalase negative (Image 1C). Unlike other beta-hemolytic streptococci, S. pyogenes expresses pyrrolidonyl arylamidase (PYR) making this test a rapid and useful adjunctive diagnostic tool (Figure 1D). Bacitracin susceptibility was used historically but has been largely replaced by PYR testing due to concerns over specificity and prolonged turnaround time.
Globally, S. pyogenes is responsible for a large percentage of infection-related morbidity and mortality. The organism colonizes the skin and the nasopharynx of humans, but most colonized individuals do not develop active disease. Colonization however can lead to infection or dissemination to susceptible individuals. S. pyogenes infections exhibit a diverse range of clinical manifestations which can include pharyngitis, impetigo, erysipelas, cellulitis, necrotizing fasciitis, pyomyositis, streptococcal toxic shock syndrome, and bacteremia. S. pyogenes remains susceptible to penicillin, making β-lactams first-line drugs of choice for management. Conversely, rising levels of macrolide, lincomycin, tetracycline, and fluoroquinolone resistance has been observed. Susceptibility testing may be warranted if these agents are to be used, most often in the cases of severe penicillin allergy.
S. pyogenes infection can be complicated by multiple post-infectious immune-mediated sequelae including PSGN and rheumatic fever. Post-Streptococcus glomerulonephritis (PSGN) has a global incidence of > 470,000 individuals per year and occurs due to the deposition of immune complexes in the glomeruli resulting from previous S. pyogenes pharyngitis or soft tissue infection (as seen in this case). Typical clinical presentation of PSGN includes hematuria, proteinuria, edema, hypertension, elevated serum creatinine levels, hypocomplementemia, and general malaise. The elevated ASO titer (5310) was diagnostic of an S. pyogenes acute infection as the cause of this patient’s cellulitis. The development of proteinuria and hematuria following infection further supports a clinical diagnosis of PSGN. Treatment of PSGN is largely supportive with the focus on management of the underlying infection. Most individuals with kidney failure from PSGN recover to baseline renal function; however, there may be a link between PSGN and the later development of chronic kidney disease/end-stage renal disease.
References
De la Maza LM, Pezzlo MT, Bittencourt CE, Peterson EM. 2020. Color Atlas of Medical Bacteriology, 3rd edition. ASM Press. Pg. 11-23
Madaio MP, Harrington JT. 2001. The diagnosis of glomerular diseases: acute glomerulonephritis and the nephrotic syndrome. Arch Intern Med. 161(1):Pg. 25-34. doi: 10.1001/archinte.161.1.25.
Stevens DL, Bisno AL, Chambers HF, Dellinger EP, Goldstein EJC, Gorbach SL, Hirschmann JV, Kaplan SL, Montoya JG, Wade JC. 2014. Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin Infect Dis. 59(2): Pg. e10-e52, https://doi.org/10.1093/cid/ciu296.
Walker MJ, Barnett TC, McArthur JD, Cole JN, Gillen CM, Henningham A, Sriprakash KS, Sanderson-Smith ML, Nizet V. 2014. Disease manifestations and pathogenic mechanisms of Group A Streptococcus. Clin Microbiol Rev. (2): Pg. 264-301. doi: 10.1128/CMR.00101-13.
Wong CH, Khin LW, Heng KS, Tan KC, Low CO. 2014. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 32(7): Pg. 1535-41. doi: 10.1097/01.ccm.0000129486.35458.7d.
-John Markantonis, DO is the former Medical Microbiology fellow at UT Southwestern and has recently completed his clinical pathology residency. He is also interested in Transfusion Medicine and parasitic diseases.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.