Case History
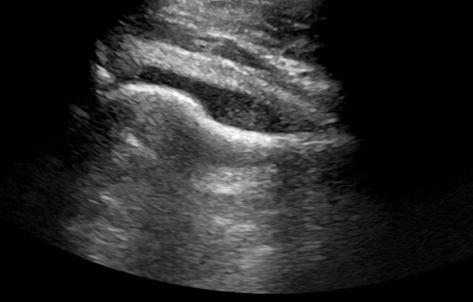
A young man presented to the emergency department with the primary complaint of severe right hip pain persisting for 2 days. This pain began after standing uncomfortably for hours at an event. His right hip was tender to palpation with some erythema and swelling. He had no recent fall or known injury. He denied recent fever, chills, aches, constipation, diarrhea, changes in urinary habits, chest pain, and shortness of breath. An ultrasound (US) of the right hip joint showed moderate amount of effusion (Image 1). Laboratory results also showed an elevated white blood cell count (WBC).
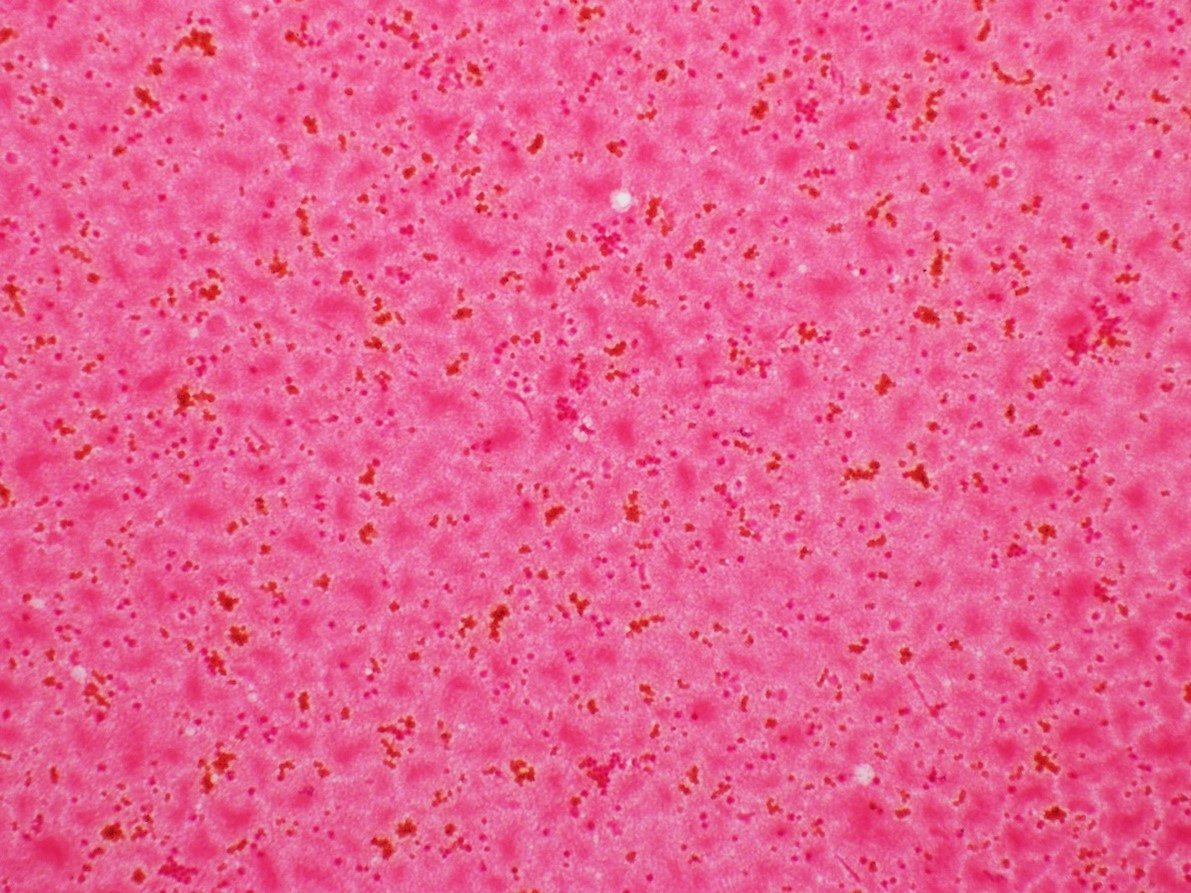
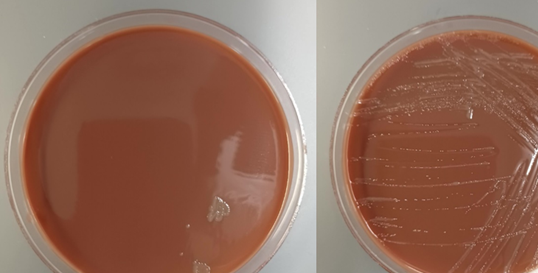
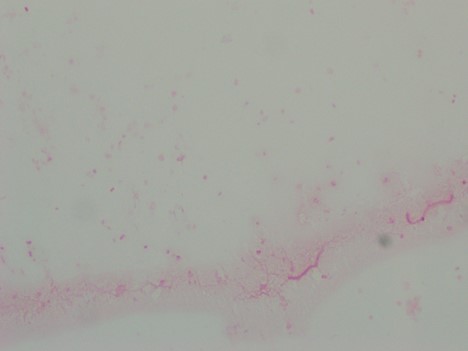
The patient underwent incision and drainage of his right hip to relieve the swelling, and samples were collected for Gram stain and aerobic and anaerobic bacterial culture. Blood was also collected from two separate sites for culture. The blood cultures showed no growth following 5 days of incubation. Gram stain of the effusion showed 4+ WBC with no organisms seen (Image 2). The joint fluid was set up for aerobic and anaerobic bacterial culture. Anaerobic bacterial culture showed no organism growth. However, a few small, grey-ish mucoid colonies grew in the first quadrant on Chocolate agar in the aerobic culture (Image 3). Gram stain was performed on one of the colonies (Image 4). MALDI-TOF confirmed the identification of Neisseria gonorrhoeae.
Discussion
Neisseria gonorrhoeae is a fastidious, gram negative diplococci bacteria that can grow inside neutrophils after surviving phagocytosis. It is oxidase positive and aerobic, and generally transmitted through sexual contact such as vaginal, anal, or oral sex.1,2 After a gonococcal infection has resolved, the patient does not develop immunity to future infections from the bacteria. Reinfection is possible due to its ability to evade the immune system by varying its surface proteins, therefore making it appear novel to the immune system.3 Signs of septic arthritis include chills and fever, pain at the joint, inability to move infected joint, erythema, and swelling.4
Multiple factors increase the risk of septic arthritis, including a systemic blood-borne infection, IV drug use, osteoarthritis, past history of septic arthritis, rheumatoid arthritis, alcoholism, diabetes, HIV, lung or liver disorders, old age, and a suppressed immune system.4 Other forms of gonococcal infection are genitourinary infections, which are the most common, disseminated gonococcemia, and gonococcal ophthalmia neonatorum. Genitourinary infections can be particularly dangerous in women if left untreated, as this can lead to pelvic inflammatory disease that could result in infertility due to scarring of the fallopian tubes.5,6 Gonococcal infections of the eyes are one of the leading cause of blindness in neonates in the United States, but can be successfully prevented through treating the mother with antibiotics before birth and administration of eye drops to the baby at birth.7
Identification of N. gonorrhoeae can be done using Gram stain, aerobic bacterial culture on Chocolate or Modified Thayer-Martin (MTM) agar, or nucleic acid amplification test (NAAT). Testing can be done from a urethral swab, urine sample, or sample of body fluid from the area of suspected infection.8,9 Culture is slow with low recovery rates. In urogenital cases, where there is ample colonization of normal flora, genital flora may outgrow N. gonorrhoeae, reducing its recovery. MTM media is useful because it is a GC agar base that makes it selective for N. gonorrhoeae growth. It contains vancomycin, colistin, nystatin, and trimethoprim lactate, which suppresses growth of most other gramgnegative diplococci, gram negative bacilli, gram positive organisms, and yeast.10 The most common testing methodology for urogenital gonococcal infection is NAAT. Some FDA approved platforms also accept rectal or throat samples, however most only accept those from urogenital sources.11 Also, while NAAT is a quick and sensitive diagnostic test, it has the downside of not being able to distinguish between DNA obtained from living or dead bacteria.12
Intravenous (IV) or intramuscular (IM) ceftriaxone is the preferred treatment choice for N. gonorrhoeae infections. Alternatively, other third generation cephalosporins can be used as well, including cefotaxmine and ceftizoxime. Typically, patients with a beta-lactam allergy have been shown to tolerate ceftriaxone, and those who cannot should undergo desensitization due to its effectiveness against this infection. A single dose of azithromycin or a prescription of doxycycline taken twice daily for a week is usually added to the regimen to cover for a potential Chlamydia trachomatis co-infection. Patients presenting with purulent arthritis should also undergo drainage, either arthroscopically or through multiple joint aspirations.13,14
References:
- Ryan, K. J., Ray, G., and Sherris, J. C. (2004). Sherris Medical Microbiology: An introduction to Infectious Diseases, 4th edition. McGraw-Hill Medical.
- Centers for Disease Control and Prevention. Gonorrhea. Available from: https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea-detailed.htm. Last updated 2021 July 22; cited on 2022 March 21.
- Hill, S. A., Masters, T. L., and Wachter, J. Gonorrhea – an evolving disease of the new millennium. Microb Cell. 2016; 3(9): 371-89.
- Johns Hopkins Medicine. Septic Arthritis [Internet]. 2022. Available from: https://www.hopkinsmedicine.org/health/conditions-and-diseases/arthritis/septic-arthritis. Cited 2022 March 21.
- Levinson, W. (2014). Review of Medical Microbiology and Immunology, 13th edition. McGraw-Hill Medical.
- Jennings, L. K. and Krywko. D. M. Pelvic Inflammatory Disease. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499959/.
- Castro Ochoa, K. J. and Mendez, M. D. Ophthalmia Neonatorum. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551572/.
- Ng, L.-K. and Martin, I. E. The Laboratory Diagnosis of Neisseria gonorrhoeae. Canadian Journal of Infectious Disease and Medical Microbiology. 2005; 16: 1-11. Article ID: 323082.
- Van Der Pol, B., Ferrero, D. V., Buck-Barrington, L., Hook 3rd, E., Lenderman, C., Quinn, T., et al. Multicenter evaluation of the BDProbeTec ET system for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male uerthral swabs. J Clin Microbiol. 2001; 39(3): 1008–16.
- Tankeshwar, A. Modified Thayer-Martin Agar: Preparation, Uses. Microbe Online [Internet]. Available from: https://microbeonline.com/thayer-martin-agar-composition-preparation-uses-colony-characteristics/. Cited 2022 March 29.
- Workowski, K. A., Bachmann, L. H., Chang, P. A., Johnston, C. M., Muzny, C. A., Park, I., et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021; 70(4): 1-187.
- Janssen, K. J., Hoebe, C. J., Dukers-Muijrers, N. H., Eppings, L., Lucchesi, M., and Wolffs. P. F. Viability-PCR Shows That NAAT Detects a High Proportion of DNA from Non-Viable Chlamydia trachomatis. PLoS One. 2016; 11(11): e0165920.
- Guillot, X., Delattre, E., Prati, C., and Wendling, D. Destructive septic arthritis of the sternoclavicular joint due to Neisseria gonorrhoeae. Joint Bone Spine. 2012; 79(5): 519-20.
- Zaia, B. E. and Soskin, P. N. Images in emergency medicine. Man with severe shoulder pain. Gonococcal arthritis of the shoulder. Ann Emerg Med. 2014; 63(5): 528-71.

-Marika L. Forsythe, MD is a PGY1 Pathology Resident at University of Chicago (NorthShore). Her academic interests include molecular diagnostics and its growing importance in the field of Pathology.

-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.

Hi,
In this case what was the source of infection? OR cause of infection?