Specimen handling and transport is a vital training topic in
the realm of Laboratory Safety. There is much to consider here that affects
specimen quality and integrity, and ultimately affects patient results. There are
also considerations involving employee safety at every step of these processes.
One group of employees that can easily be overlooked when it comes to proper
safety training is lab couriers. They perform the important role of properly
and safely transporting specimens for testing, but without the proper education
and tools, these team members can quickly fall into situations of harm.
The courier was running late, and she had one last stop on
her route at a medical office building with multiple physician offices and drop
boxes. It was cold, and she decided to leave the vehicle running while she went
inside to pick up more specimens and deliver lab reports. The car was also left
unlocked. When she came back outside, the car was gone. It was found hours
later in am empty field, but it had been set on fire. There were lab specimens
and reports strewn all over the field and into the nearby woods.
Couriers need to be trained about the importance of their
role, and that training should include information about security and protected
health information (PHI). Be sure to include HIPAA training for all courier
staff. When discussing security, enforce specific processes such as always
turning off vehicles before exiting and properly securing all patient specimens
and any paperwork being transported. Whether couriers use company vehicles or
their own personal transportation for the job, making sure harm does not come
to the vehicle nor any contents being transported is key.
The courier knew he had a long drive ahead of him because of
the toll bridge, and he had several specimens that needed to be delivered as
frozen. He went to the lab’s cooler and scooped a large pile of the dry ice into
a big box using his hands. It was cold, but it helped to wake him up a bit. He
placed the specimens in the box and placed it in the back seta of his vehicle. It
wasn’t very warm out, so as he began his drive, the courier made sure the heat
was on high and that all windows were closed. After a few miles, the courier began
to fell very tired. He struggled to stay awake, and he couldn’t figure out why.
After sitting in traffic on the bridge for a time, he pulled off the road and
called the dispatcher to let them know he could not continue. When he got out
of his vehicle, he began to feel better.
CAP regulations require that laboratory staff have dry ice
safety training, but that requirement extends to anyone who may acquire the
dangerous substance in the lab. Make sure staff are aware of the need for
proper PPE use when handling dry ice. Insulated gloves, the use of a scoop or
tongs, and face protection are necessary when scooping ice into a container.
Couriers should carry no more than three pounds of dry ice in a vehicle, and
there should always be adequate ventilation, including open windows in the
vehicle when transporting dry ice. Dry ice converts rapidly from a solid state
to a gas, and that gas rapidly displaces oxygen in the air making it difficult
to breathe or stay conscious. High volumes of dry ice in a car can create a
very deadly road situation in a short amount of time.
The courier was transporting pathology specimens in a
cooler, but was unaware that the lid had popped off of one of the specimens and
formaldehyde was splashing all over the inside of the cooler. As time went by,
the courier began to feel queasy. After realizing that something did not smell
right in the vehicle, she eventually stopped the van and pulled to the side of
the road to investigate. She opened the cooler and quickly pulled out dripping
specimens and set them on the carpet before feeling too sick to continue
cleaning up the mess. She had to be taken to the Emergency Room for
formaldehyde exposure symptoms while the Lab safety Officer had to bring spill
clean-up supplies to the van to neutralize the formaldehyde. The carpet had to
be removed and disposed of properly.
Courier vehicles need to be equipped with spill clean up
supplies that can handle whatever types of spills could occur during transport.
If formaldehyde is transported, couriers need training in the proper transport
and clean up of that chemical. Biological spill kits should be available as
well, and spill training should be a regular part of overall courier safety
training.
I wish I could say that these were imaginary stories, but
sadly, that is not the case. The stories, though, illustrate clearly what can happen
when proper safety management and training are lacking. Every part of the laboratory
pre-analytical process is important, and every lab team member involved in the
process needs to be considered. Employ complete safety training, and assess safety
competency on a regular basis. By providing the proper tools and safety
training to couriers, you can ensure the quality of lab results, and you can prevent
incidents like these with your employees.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
The turn of the year is a quasi-inspiring time for many
people who attempt to change something about themselves or their situation with
“New Year’s Resolutions.” When my friends and I were heading to brunch on New
Year’s Day in southern California, there were many people running (alone or in
groups) which I hadn’t seen before and my one thought was, “How long will that
last?” When I returned to Chicago after the holidays, I dusted off my gym
membership card and logged some treadmill time—my one thought was, “I hope this
lasts!” But we are all too familiar with the breaking of these resolutions by
most of us, and the ultimate regret we feel in the latter part of the year when
our hopes and dreams of thinness/money/power/rare pokemon/fame have been dashed
by the collision with our actual lives and the limited time we have to get done
what needs to be done. Fortunately, we are human beings and we are allowed to
be disappointed with ourselves over this (or these) tiny failings as long as
our life trajectory is heading the way we want*. Then there are those handful
of people that each of us will ultimately know who stick to their resolution
and shed the weight, get a new job, or (hopefully with increasing numbers!)
quit smoking! And we are more inspired by their actual doing of these things
than by our lack of resolve.
As individuals, this trivial annual mindset is acceptable and even entertaining. But as a society, empty promises and feigned changes are simply unacceptable. To certain things, we must as a society—and as individuals in that society—commit. Recycling, for example, is a strategy that is both an economic and environmental boon. But as of January 2018, our major “solution” for plastics (especially from the West) that was China has now ended. Other nations willing to take these recyclables stopped their acceptance as well towards the end of 2018. What can we do to solve (not resolve) this situation permanently? Each country should consider first the role of plastics in their society and perhaps, like many African nations, simply ban the product(s). Secondly, encouraging personal recycling and reuse of plastics, for example through water filters to refill plastic bottles or fees on reusable grocery bags, can minimize impact. But, ultimately, each nation needs a sustainable recycling plan that represents a balance of production and utilization, creating a negative plastic total impact (i.e., no new plastic created).
In pathology, the theme of recycling is very important for any laboratory but can have major benefits for laboratories in developing nations. Formalin, xylene, alcohol, and paraffin (the four principle reagents for pathology processing), can be recycled using devices or process plans that can have minimal capital costs to set up. Consider that a given country may have shipping challenges such that an order placed today for 10 gallons of neutral buffered formalin may take 6 weeks to 6 months to arrive and cost 3 to 5 times the price in another country. In that setting, recycling formalin is clearly a superior approach and extrapolates to xylene and alcohol. Process approaches to paraffin (e.g., collecting waste paraffin from trimming and lids, using minimized mold sizes, lateral flow to minimize contamination) can optimize the use of the wax and reduce costs. As these four reagents represent core elements to the process, efficient utilization, reuse, and management can keep costs low and processes running. But the laboratory must commit to this process and adhere to it every moment of every day to change patient’s outcomes for the better.
Similarly, core histology equipment (unlike many clinical laboratory machines) is almost indestructible when properly managed and maintained. Laboratories in developed nations may replace this equipment when it is several years to a decade old when the equipment may have another decade (or sometimes two) left of life. Decisions to replace functional equipment are left to the individual laboratory; however, once this process occurs, functional equipment should not be left to collect dust and should be moved to a new location where it can be of value. Every laboratory considering the replacement of older equipment must ask the question, “What is the remaining functional life of this device?” If that number is many years or the often stated 70%, a plan for donation of the equipment is highly suggested. It is this philosophy that inspired the ASCP Center for Global Health program along with many other groups to actively seek out donated, functional equipment and transfer it to nations and colleagues who desperately need it to maintain their pathology services (Do you have equipment for donation? Email us!). This is especially important because the perceived demand for histology equipment in many low-income countries is so low that manufacturers and distributors refuse to become involved with the equipment (especially with trade and tariff barriers standing in the way). But, in truth, the demand is the same per population as in any other country with at least one high volume, functional pathology laboratory needed for every 1 to 3 million people (depending on population age structure and clinical utilization).
As we begin a new year together, reflecting on what we did (and didn’t) do in 2018 and what we can (and should) do in 2019 is an iterative process that can guide us through many decisions. I hope that everyone reading this blog takes a few moments (or even an hour if you can spare it!) to delve into 2018 and really plan for 2019 with true solutions in mind for any challenges you identify. And, lastly, always take some time every day to think outside yourself and even your laboratory to others in your local community or in foreign lands. Consider what little (and big) things you can do that may improve the life of just one person other than yourself and commit to those things.
*If your life trajectory is not going the way you want, consider performing a personal SWOT (strengths, weaknesses, opportunities, threats) analysis and think outside the box about where you are and where you want to be. Don’t be afraid to make life changes or new life choices that give you a better piece of mind and stronger sense of self and self-awareness. A room full of happy people who are self-aware and emotionally intelligent can solve problems at light speed because their personal issues (good or bad) don’t get in the way. So, for 2019, I strongly encourage everyone to consider really solving (not resolving) the problems you perceive in your life so that we can all work together to solve (not resolve) the challenges we face as a society moving into the next decade.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
This is a longer one but, to me, there’s a lot of
interesting stuff I wanted to share with all of you!
(TL;DR Path and Psych
aren’t too different, but they are. There
are interesting overlaps, and doing research right is really critical.)
The last month of 2018 has me rotating through my psychiatry clerkship in medical school. With that, I’ve had an interesting opportunity to look at pathology from a very distant lens. (Very distant; think diminutive picture of Earth from Mars far…) During one grand rounds session, Dr. Owen Muir, the medical director of Brooklyn Minds said something to the effect of, “[people say] Psychiatry is different, so much so that we’re the most removed from our tissue of concern.” That was pretty poignant. He was talking about the brain; in testing, treatment, and practice, it’s virtually inaccessible without a major neurologic undertaking and almost unreachable between pharmaceutical and external therapeutic interventions. Here’s the same thought another way: a neuropathologist can show you what parts of the brain do what in a particular pathologic process grossly and microscopically, while psychiatry focuses on pharmacologic, cognitive, and comprehensive behavioral therapies. A microscope versus a telescope—but both a way to focus on a problem. When I compared that to some things I heard during my orientations, it became clear that Psychiatry and Pathology might be very different animals.
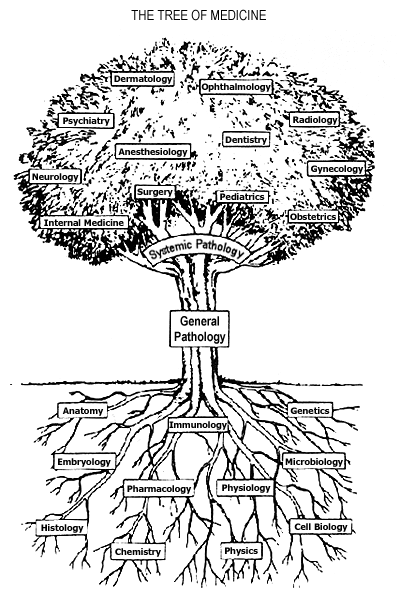
I’ll get back to Dr. Muir and the Brooklyn Minds’ work with cutting-edge deep Transcranial Magnetic Stimulation (dTMS)—yes magnets—in just a minute. First I want to show you that, despite being light-years apart in distance, these two specialties overlap more than people realize. No, not with regard to behavioral stereotypes; read my previous post on stereotypes in lab medicine, and let’s get that out of the way right off the bat. The foundational concept which continues to bring every specialty closer together is translational research. Consider the following, if the field of Medicine was a tree, specialties would be complex branches and basic scientific principles would be the roots of knowledge. And what connects the roots to the branches? All the years of scientific research that translates data gathered from experimentation in fields like physiology, microbiology, or chemistry into specialties like nephrology, infectious disease, or endocrinology. Wait! That’s pretty much our job—duh. Cool, so since we translate the data, we’re all the junk in the trunk! So within the realm of research in medicine, I want to show you examples of cutting edge limitations, intersectional data sharing, and shortcomings in translational research.
Cutting edge or the
bleeding edge?
So, I mentioned Brooklyn Minds. Sounds dramatic, like a movie title; but you won’t find any groundbreaking 90’s soundtrack by Coolio or a Michelle Pfeiffer-driven story about inner city youth. Instead, what their webpage outlines very nicely is the important and impactful work they do in psychiatry which includes repetitive or deep therapeutic magnetic stimulation (rTMS/dTMS). I promised I would explain the magnets thing, okay so here goes. Essentially, dTMS is a pulsatile magnet-driven energy wave directed at specific regions of a patient’s head. The energy works like a magnetic field to activate or inhibit (think “polarize” or “depolarize”) small patches of neurons within the brain, penetrating beyond the bony cranial vault and centimeters into the parenchyma of brain tissue. Using a premise which is basically similar to an MRI, patient’s brains are “mapped” for functional region analysis—a new, subtler way of looking into focal deficits. Two major mental illness that dTMS has literature supporting treatment include Major Depressive Disorder (MDD) and Obsessive Compulsive Disorder (OCD). So first, you have to understand one thing: neurons are basically our electrical circuitry, conducting energy potentials as signals back and forth translating and calculating motion, sensory input, and position. If nerves are electrical wires, think of myelin as a conductive insulator for higher signaling strength. The conduction potentials of certain mapped regions of the brain demonstrate decreased activity in particular areas with corresponding anatomical locations where we know disease processes can occur. For example, we understand the changes in brain chemistry to treat it pharmacologically, but depression has visible impacts on the hippocampus and prefrontal cortex. Why not treat this directly, like the way a surgeon would treat a hernia?
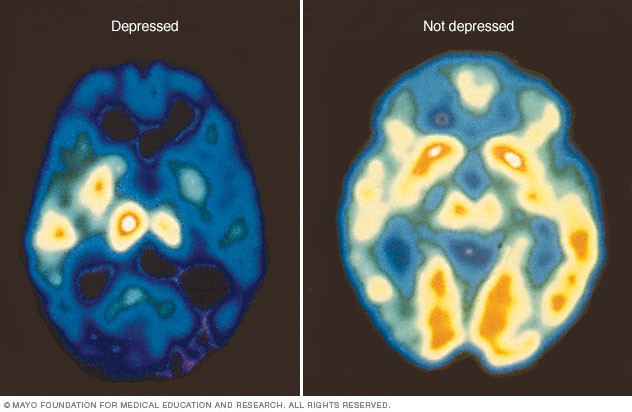
Image 4: Let’s take depression, for example. In the PET scan on the right, you can see what a “normal” brain functional status is mid-scan. On the left, however, would be a “depressed” brain. With cortisol in surge-mode and a poverty of available serotonin and norepinephrine in the brain, you can see widespread variable activity from the amygdala, hippocampus, prefrontal cortex, and beyond. (Source: Mayo Clinic)
This seems like some next-level Doctor Who science, right? So, the biggest question here would be: does this work? Since TMS (of which there are multiple types, with special equipment—not important for this discussion) is a medication-free treatment, doesn’t this sound almost perfect? Combine that with the fact that dTMS treatments often potentiate positive response for follow up treatment since the “rewiring” promotes future effectiveness and this might sound too good to be true. Studies are being published by the pound hailing this type of therapy as a potential life-saver for psychiatry which has been struggling to contribute longitudinal positive outcomes for patients. Evidence is strong for the use of dTMS in a variety of mental health issues, but it’s still early—you might find studies with large number of subjects, but you might not find ones with long-term analyses. So the research today is overwhelmingly positive and there are multiple studies in published literature about the effectiveness of this therapy in depression resistant to medication, or the utility as a maintenance therapy in an outpatient setting, or even potential use for substance use disorders. But, there are skeptics just as vocal as supporters. (Side note: If Dr. Oz does a story on a treatment like TMS, do we have to abandon it and move on completely?) As an emerging therapy, Psychology Today published a consumer report of sorts which discussed issues like access, refractory response, and more proven standard therapy like ECT (electroconvulsive therapy). Although it is FDA approved and non-invasive (minus some potential headaches), questions about TMS address things like how to get insurance to cover it, should it be reserved as a last resort after things like medications/ECT, and since it’s a relatively new treatment should we pursue more longitudinal studies first?
Image 5: Have a seat! This instrument has the potential to treat a myriad of psychiatric illnesses by using magnetic fields aimed at “adjusting” improperly firing neurons in the brain. Research still remains outstanding as to whether dTMS can affect someone’s …magnetic personality. (Source, except for my pun: Cognitive Psychiatry of Chapel Hill)
Taking it back to the
source
Way back in the beginning of 2018—if you can remember such a time—an article was quietly published in the journal Science. This was a large collaboration funded by the National Institute of Mental Health (NIMH) among many other supporters, with a team that spanned from UCLA, to Denmark, to Chicago (woot!). Printed in the section header “Psychiatric Genomics,” it was called “Shared Molecular Neuropathology Cross Major Psychiatric Disorders Parallels Polygenic Overlap”—wait, what? Yes, among some major psychiatric disorders we all know, love, and read about in the DSM-5, some of them share specific genetic mutations. Full stop. Pivot. Let’s leave our Freudian couch and walk over to the lab…
Image 6: Experimental rationale and design where section (A) illustrates the model of proposed psychiatric disease pathogenesis and the authors’ (B) experimental process which they concluded was “highly suggestive of a causative genetic component” (Source: Gandal et al. 2018, Science 359, 693–697)
What these authors suggest is that five major psychiatric disorders—autism spectrum disorders (ASD), schizophrenia (SCZ), bipolar disorder (BD), major depressive disorder (MDD), and alcohol abuse disorder (ADD)—all share specific gene-expression changes which indicate transcriptional dysregulation (i.e. mutations) at single nucleotide polymorphism (SNP) locations which is very consistent with inheritable genetic variants. In short, small, specific mutations seem to be identifying features for those five disorders, which might reveal genetic risk and potential future treatment targets. Even more than this, what we see commonly as overlapping features in patients’ clinical presentations may actually be explained by overlapping genetic expression and penetrance. We’ve long had historical evidence supporting the hypothesis of mental illness as an inheritable disorder. Twin studies have shown the increased probability of expressed diseases like bipolar disorder or schizophrenia in monozygotic twins compared to dizygotic ones—but the twins’ clinical presentations don’t always yield 100% confidence there. Clinicians are acutely aware of the genetic component present in diseases like these, but targetability has proven difficult. According to the National Institute(s) of Health and Mental Health (NIH/NIMH), “strong evidence may exist for genetic susceptibility, but no specific gene has been unambiguously identified for common forms of mental disorders,” and “the estimate of the influence of environmental factors on the disorder provides an index of how difficult the search will be.” (Source: NIH/NIMH Genetics and Mental Disorders: Report of the National Institute of Mental Health’s Genetics Workgroup – Mental Disorders and Genetics: What We Know Today) That was in 1997! A similar paper to this one published in The Lancet in 2013 addressed these same five psychiatric disorders correlating some genetic components to a region on Chromosome 3 against almost 30,000 normal/wild-type patients. The NIH responded then saying that though there were significant correlations presented therein, there isn’t enough evidence to show the risk associated with the mutation and further research is necessary. Fast forward to some further research and we now see evidence of overlap between particular mental illnesses as well as cell-to-cell signaling as a specific neuropathological mechanism of disease. Is it enough for a Nobel Prize? No. But think of it somewhere between a paper titled “We’ve Discovered Insulin!” and “Patients with Diabetes Often Have Elevated Blood Glucose.”
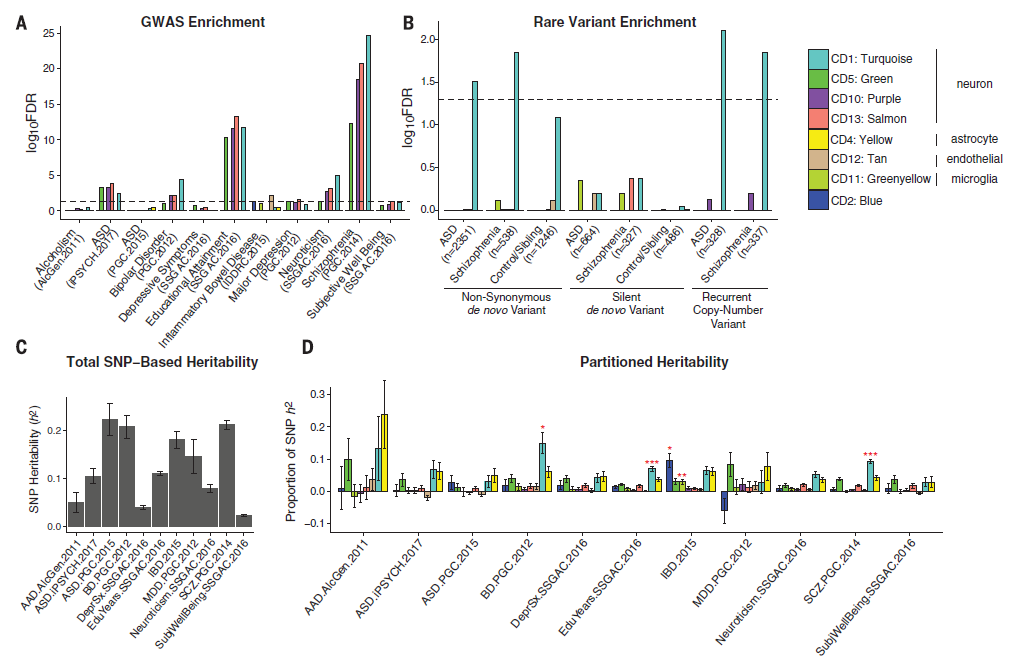
Image 7: Evidence to suggest that certain gene expression patterns overlap which demonstrates transcriptosome similarity between various two-disease combinations/overlaps (A) and that there seems to be a spectrum or progression of disease intensity relating to a gene’s mutability (B). However, gene expression can both show that normal biologic function can be associated with these variants (C) and that, even though disease overlap implies correlation, ASD seems to mutate independent from the rest (D). (Source: Gandal et al. 2018, Science 359, 693–697)Image 8: Hub genes are targets of research because of they are modeled as functionally significant markers of genetic variation and/or mutability. In this abbreviated data infographic, the top 20 gene hubs were collected for their association with gene activity in each of the five diseases. The functional aspects represent mutations (colored circles) in various aspects of neuronal cells including receptor activity (dark blue), mitochondrial structure (green), immune response/regulation (yellow-green), mitochondrial metabolism (purple), neuronal activity (pink and light blue), cellular architecture and growth (tan), and other neuronal metabolism (yellow). The lines connecting these mutations are a representation of Eigengene networking, which illustrate gene co-expression and functional relationships. (Source: Gandal et al. 2018, Science 359, 693–697)Image 9: What’s the take-home message here? Basically, the final conclusion is this: take all these demonstrated mutations as functional pieces of mental health and down-regulated neuronal expressions of genes highlight potential risk stratification. Genome-wide association studies (GWAS) shows high concentrations for SCZ, ASD, and BD variants (A) and those variants presence in the neuronal model for various nerve cell types is shown (B). The main lesson here is the projected diagnostic liability and risk assessments for patients who have these specific mutations (C & D) which may be correlated to this research’s co-expression models. (Source: Gandal et al. 2018, Science 359, 693–697)
Correlation does NOT
imply causation, but isn’t it so tempting!
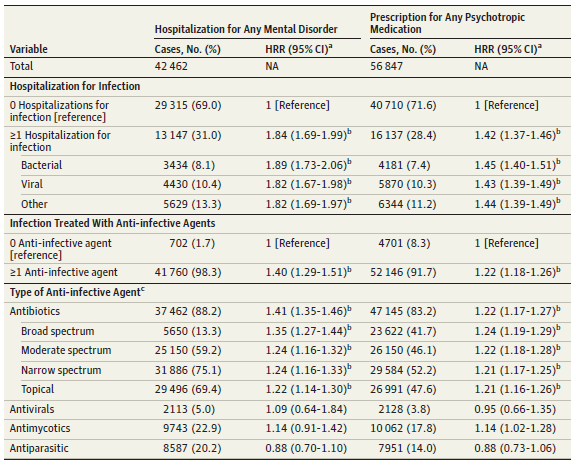
While promising articles like these offer amazing potential insights into a deeper understanding of clinical diagnostics for psychiatry, articles are as numerous and complex as patients. An article published this month from the Journal of the American Medical Association (JAMA)Psychiatry correlated an association between hospitalization and subsequent mental disorders in children. Anything that purports to associate new causality between disease entities and trends is always worth a read. And, like any other experienced clinician, you go straight to the title and design methods to determine your gut feeling about this paper before continuing. The title: “A Nationwide Study in Denmark of the Association between Treated Infections and the Subsequent Risk of Treated Mental Disorders in Children and Adolescents;” the number of patients studied: over 1 million. What? That’s amazing! 1 million cases, what amazing data, what amazing insights, what …a statistical nightmare. Finding results in a million is both exhaustively comprehensive and statistically problematic. Black holes are rare. But if you search the entire universe you’ll find millions. “With a large enough sample size, rare things become common…” this was said with a pregnant pause and the normal gravity delivered by astrophysicist Neil DeGrasse Tyson, PhD, during a live taping of Star Talk my wife and I attended a month ago.
Image 10: From Star Talk, November 14th at the Beacon Theatre in NYC, left to right: co-host and comedian Eugene Mirman, actress Ellie Kemper, comedian John Mulaney, scientist Julie Huber from Woods Hole Oceanic Institution, scientist Kevin Hand from the NASA Jet Propulsion Lab, and co-host and astrophysicist Neil DeGrasse Tyson. The show discussed life on other worlds, and the realistic expectations of research and what to look for when you’re looking for life in space. The most poignant point of the night came during Dr. Tyson’s conclusion where he talked about different specialties growing apart and coming together over the last few hundreds of years—we used to have an isolated biologist and astronomer, where today astro-biology is a new exciting front!
What came up during that show was the same theme I’m
discussing today: it’s very important to do research, collect data, and
translate that data appropriately. Especially in medicine, where conclusions
and results from research can affect patient outcomes, lab professionals like
us need to be leaders.
Back to this paper, the authors report a strong significant correlation between hospitalization events requiring antibiotics and the prevalence of mental illness later in life. Analyzing the hazard risk ratio (HRR) for these patients reveals values usually over 1.0 which show that they are above the regular risk when compared to patients not under these conditions. The authors associate treated infections with childhood/adolescent mental disorders, but include a very important remark at the very end which is ever-present in most good research. They address the fact that results and conclusions from their data may be explained by other, non-studied causes directly because of otherwise not understood pathophysiology. And, like 99% of pathology reports I’ve seen end with a dogmatic “suggest clinical correlation,” this paper closes with something similar to “further research is needed.”
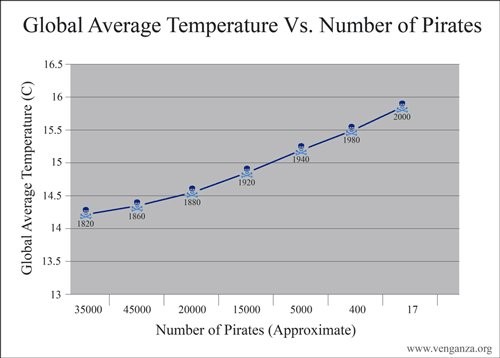
Image 11: Hazard risk ratios (HRRs) here demonstrate that individuals requiring hospitalization for infection were increased (with high confidence analysis) for having a hospitalization for any mental disorder and for redeeming a prescription for any psychotropic medication. (Source: JAMA Psychiatry 2018. doi:10.1001/jamapsychiatry.2018.3428)Image 12: You can find tons of funny causation-correlation infographs on the internet. They prove a great point: we have to be careful how we translate our data. Without arguing that because higher global temperatures melt the icecaps pushing more sailors to a life of pillage and plunder, these two findings are assuredly non-related.
So that’s it! Using data is great! It’s the best. Translating direct and clinically relevant findings from the bench to the bedside is what we do best. Consulting with our clinical colleagues, those of us in laboratory medicine have a responsibility to make sure of four main things. First, we have to make sure that the results we obtain are clear. Pre-to-post analytical analysis is paramount to testing efficacy and we’re the experts on standard procedures and accountability. Second, the interpretation of results whether it comes from a research lab or hematology bench must be valid. Protocols and metrics are great, and using them to ensure effective use of information is critical. Third, the conclusions we reach should be meaningful. If it’s a cancer staging diagnosis biopsy report or a groundbreaking publication on shared genetic variants, the implications must provide the best information for patients. Because finally, we do what we do for them. Our work and efforts always go back to improving patient outcomes, and giving each person the best chance at maximum health and quality of life. Pathology and psychiatry might be worlds apart, but only in vocabulary at best. We’re on the same team. And, despite finding each other as great neighbors in most Medscape physician job reports, we both work very hard to lead the charge in protecting, healing, and advocating for our patients.
Wishing you good mental health! Even outside the Seattle area, fictional Dr. Frasier Crane’s “I’m listening” catch phrase is great advice toward patients, colleagues, and generally everyone. Leadership is a great responsibility, but it’s worth nothing if you don’t pay attention to what needs to get done.
Work is central to the human experience, even though the actual practice of work has continuously changed through the decades. These changes impact personal life as well, since there is a strong correlation between work life and life outside of formalized productivity. There are certain factors that influence how work is practiced that impact people’s approach to work.
The first factor is technology. Technology has significantly altered the practice and implications or work. For example, try to compare what office work was like 50 years ago compared to now, or how laboratory diagnostics were different back then. In today’s age, the majority work tasks are conducted on the computer or through technological advances: emailing, writing, analyzing, diagnosing. Fifty years ago, such tasks were conducted via phone, typewriters, or by hand. Technology has also increased the amount of information available to workers. This information allows organizations to prepare to lead in a VUCA world, namely one that is volatile, uncertain, complex, and ambiguous.
The second factor that influences work is globalization. Through the increase in technology and information as mentioned above, cultural, linguistic, and national boundaries do not impact the work environment as much as they did. Such lack of confines pushes both organizations and individual workers to be more competitive due to reduced market and job security, respectively. On the other hand, it also increases collaborations and opportunities to help others. For example, through telepathology, we are now able to provide diagnostics to people in places that do not have access to local laboratory services.
The third factor that has an impact on work is the psychological contract between worker and employer. During the industrial age, this contract was mostly stable and predictable and was based on the assumption that if workers performed well, had integrity, and were responsible their work created a sense of connection. In today’s work culture, this contract has shifted towards a focus on self-development, experience, and personal long-term goals instead of a long-term relationship between worker and employer.
Lastly, a factor that influences work is the knowledge gap. Since many of the unskilled jobs are now conducted by computerized machines, employers will rely more on workers with specific skills and knowledge. However, educational opportunities are not equally distributed and the lower classes are at a clear disadvantage.
It is important to understand these factors when working with people from different educational, technological, and cultural backgrounds. All these factors influence people and how they perform their jobs.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
As a fitting end to my previous 3-part series on how to prepare for and survive your regulatory inspections, one of the hospitals we provide consulting services to was just visited by The CAP. Overall we did great and I’m proud of everyone there, but the inspectors found a weak area for us to improve upon that others may be struggling with as well: documentation of training and competency.
It is a common misnomer that training and competency are equivalent and essentially the same thing. Whether you’re subject to CLIA, CAP or your local state DOH requirements, you will be required to provide proof (documentation) of both training AND competency for each employee, for each task that they perform. This is not just limited to your technical staff, but also includes non-technical personnel (phlebotomists, lab assistants, LIS personnel,transport couriers, etc.), as well as staff outside of the immediate laboratory testing area (respiratory clinics with blood gas analyzers, Point of Care testing, etc.).
Simply put, training is coaching, mentoring, and teaching someone step-by-step how to perform a specific task. Proper documentation of this training includes:
Objectives for the training (i.e., “After completing training, staff will understand howto successfully perform maintenance tasks on the hematology CBC analyzer.”)
Identification of the methods to be used during the training (direct observation, monitoring recording & reporting of results, review of worksheets & preventive maintenance records, evaluation of problem solving skills)
Identification of the materials to be used during the training (cleaning agents, QC samples, previously tested & scored proficiency testing material)
Criteria used to assess the effectiveness of the training (minimum score of 90% on critical thinking quiz, ±10% correlation with previously tested sample)
Signature of both the trainee and trainer confirming that training was completed, and when
In addition to the obvious routine tasks a lab professional will need to perform (running QC, instrument maintenance, running patients), don’t forget to document their training for the low frequency tasks performed as well. Based on an employee’s job description, they may be involved in additional tasks such as specimen handling, safety precautions, packing and shipping of samples to reference labs, computer system training, telepathology training, and supervisory functions. These tasks too will require documentation of training.
Documentation of all of these tasks can be organized through the use of a departmental orientation checklist. This will help you keep track of what each staff members’ specific job junctions will include that they need to be trained on, and which tasks have been completed by each trainer. Depending on the task, training can be completed quickly after several minutes of demonstration (waived urine hCG testing), or may take several weeks for staff to fully understand and master the task (flow cytometry leukemia work-up). Keep in mind that until a staff member has documented training followed by successful assessment of competency of that task, they should not be permitted to perform or result patient testing independently of their trainer.
Once training has been completed and documented, you must then assess each staff member’s ability to successfully perform these tasks. This is their competency, where you assess if the training was successful and staff are able to perform each assigned task correctly. To fully demonstrate successful competency of non-waived tests, all 6 of the following elements must be documented for each employee, for each task:
Direct observation of patient test performance, including patient identification, specimen collection, handling, processing and testing.
Monitoring the recording & reporting of test results, including when appropriate the handling of critical results.
Review of testing worksheets, QC records, proficiency testing results, and preventive maintenance records.
Direct observation of performance of instrument maintenance and function checks.
Assessment of test performance through testing previously analyzed specimens, internal blind testing samples or external proficiency testing samples.
Evaluation of problem-solving skills.
Observation of compliance with safety protocols (based upon your specific local state DOH regulations).
The documentation of your competency elements should include the date each item was evaluated, as well as a way to identify and recreate the test performance if asked by an inspector. This is most easily accomplished with the specimen ID number, or PT survey name so records can be located or reprinted.
Be mindful of your local state regulations regarding the specific requirements for who can perform a competency assessment. In many cases, assessors will need an additional supervisor competency for themselves to confirm they are able to successfully assess the performance of their peers. If weaknesses are identified during the competency assessment, additional training should be performed with appropriate corrective actions documented. Competency should be reassessed to ensure staff are correctly performing all duties, prior to them resuming patient testing.
So to summarize:
During training, I am showing you how to do something. I will document all aspects of the training steps that I reviewed with you. When I assess your competency, you are showing me that you know how to do the task correctly. You will document your results as you were trained how to do, and I will validate the accuracy of your work.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018 Top 5 in the 40 Under Forty recognition program. She has worked in the medical laboratory profession for over 18 years. In her current position, she transitions between performing laboratory audits across the entire Northwell Health System on Long Island, NY, consulting for at-risk laboratories outside of Northwell Health, bringing laboratories up to regulatory standards, and acting as supervisor and mentor in labs with management gaps.
As this year comes to a close and we look forward to celebrating holidays with family and friends, we can also celebrate our accomplishments over the year. Our jobs in the clinical laboratory are vital in helping physicians make clinical decisions and we should celebrate the role we play in healthcare. In hematology, techs are busy doing daily tasks; QC,maintenance, and analyzing all the samples that come into the lab, 24 hours a day, 7 days a week. We work constantly to provide physicians with accurate and precise results in a timely fashion. But, what else goes on in hematology?
This past year has seen many changes and challenges in our hematology lab. In February, we switched our hematology analyzer to a new Sysmex system,and went to autoverification at the same time. This was a process that had begun months before with meetings with the Sysmex team, building rules for WAM,validations, training key operators, as well as site surveys and actual planning for the location of the instrument and water and electrical connections. Before we went live, new procedures had to be written and all techs had to be trained on the new system. Every tech in the department had to do competencies, everything had to be documented and the new procedures had to be signed. This doesn’t stop once the instrument is in use. There has been a continual learning process since then as techs become more familiar with the system.
During all the excitement and work involved with a new instrument, we, as have many labs, have had turnover in staff which has led to its own challenges. Techs have retired, moved out of state, been on maternity leave and have left us for other opportunities both in other areas of our lab and elsewhere. New staff needs to be hired and trained. Students need mentors during their rotations. It’s a cycle we go through every year, a never ending process. And, no sooner had we seemed to have everyone trained, then it was time for 6 month validations and competencies.
In September we moved to new Coagulation instruments, which, fortunately, was not as big a change as our Sysmex analyzers, because the coag instruments are newer versions of instruments we already used. Yet, there were validations to be done, training to be done on the new software, and procedures to write, all at a time when we were about to go live with a new LIS!
Perhaps our biggest project of the year came to fruition in September when we moved to Epic for a hospital wide software system. This was an undertaking which was well over a year in the making. Again, this transition involved many months of meetings, working with Epic and our IT department to create test codes and profiles and to build the system to our needs. We worked with Sysmex and WAM support to verify that there would be a smooth transition from the old system to the new. The month before go live, we did wet and dry testing of every possible scenario and tested every rule in WAM. And then we tested every rule in Epic. Many hours and late nights were spent entering test orders, creating spreadsheets, taking screen shots, and going back and forth to IT for changes and updates. An integral part of this Epic journey was more training for employees. Superusers were trained, training sessions were held for all, and then superusers helped to support other users at Go Live. And, of course, all of this this meant more procedures had to be written. The epic day arrived, and though things didn’t seem too smooth at first, the support teams were and continue to be available to help and make changes as necessary.
These are just a few of our particular challenges this year in the department. Even without these added projects, though, there is a lot that goes into operating a hematology laboratory. Every week, every month and every year, there are ‘extra’ or ongoing projects to be completed in every laboratory department. While we had some major changes this year, there were also many smaller ones. There are always new pieces of equipment that need to be validated, and new procedures or job aids to be written. Quality control has to be monitored, calibrations have to be performed, new lots need to be entered and tested, linearities have to be done. CAP surveys need to be assigned,reviewed and submitted. Inventory needs to be taken, vendors need to be met with or contacted and supplies need to be ordered. Equipment repairs ,troubleshooting and maintenance all need to be addressed. Training doesn’t stop at new hires and students. All techs have to complete annual competencies. Every year instruments have to be validated, new lot crossovers have to be done, and all procedures must be reviewed and updated. We need to get ready for inspections, or perform self-inspections. I’m sure I am leaving out a list of things, but this is a brief overview of all that goes into laboratory operations. It’s certainly more than just analyzing samples!
Who does all these ‘behind the scenes’ tasks? The department supervisor or technical specialist may be designated to make sure these are all completed, but often senior techs or career ladder techs can play an important role in meeting all these requirements. Many hospitals now have career ladders that allow techs to use the designation MLS II or III or MLT II or III. Our laboratory started such a program this year. For anyone interested in moving up the career ladder in their laboratory, there are many opportunities to be involved in lab operations and management. All the tasks that are required to run a lab cannot be done by one person alone. Tier program requirements differ from hospital to hospital but may ask candidates to submit a tier application and complete a list of achievements to show their commitment to the laboratory and their community before being designated a tier II or III.
Tier techs are generally required to meet education and certification requirements. They should be pro-active performers who are seen as leaders with excellent customer service skills. A tier level tech is a proficient performer with strong critical thinking and problem solving skills. They are mentors to coworkers and can train staff and perform competencies. Hospitals often look to these techs to contribute to the growth of the profession outside of the lab, as well. Being laboratory science community ambassadors, performing community service and upholding the mission and values of your facility all constitute qualities a hospital looks for in a tier tech.
Does this sound like you? We are constantly in need of techs to aspire to working in supervisory positions and management. With an increase in age of supervisors, managers and administrators, we are seeing an increase in retirements. We need more techs doing routine bench work to take the initiative and the steps to become tier techs and lead techs. We need aspiring supervisors and managers. Why wait? I encourage you to make a New Year’s resolution to seek out your facility’s tier or career ladder program. If one doesn’t exists, make it a project to see if one can be introduced!
Laboratories are often hidden in the basement, out of sight of visitors and out of mind of the general public. When we mention we work in a hospital, people ask “Are you a nurse?” Even though we may not be a well-known profession, we are a very important group of dedicated scientists and can be very proud of our accomplishments and contributions. I thank my supervisor and mentor, Gene Galligan, for her encouragement and support of the tier program and for all the things she has taught me in this very busy year.
PS: As I wrote this, The Joint Commission team arrived to
start their accreditation process. There is never a dull moment in the
laboratory!
Happy New Year!
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
While it doesn’t seem possible, another year is drawing to a close. At this time of year, I often ask my clients what they have worked on or what they have accomplished with regard to laboratory safety in the past twelve months. Sometimes they can readily answer, especially if there was a major project that took a big chunk of their time. Other people, though, struggle with an answer wondering if they did indeed accomplish any of their safety goals. I contend that we all have had successes and achievements, though, but we might need to dig a little deeper to find them.
Regulations in the realm of laboratory safety did not stay the same in 2018, and if you kept up with any of them, you made some progress. For many U.S. states, the beginning of the year brought about the Environmental Protection Agency’s Generator Improvement Rule (GIR). Among other things, this new set of regulations changed how labs (and other departments) label their waste containers. All hazardous (chemical) waste containers must now be labeled with the exact words “Hazardous Waste,” and there must be a description of the waste as well as some form of a hazard warning. That warning can be in the form of a pictogram or even a NFPA/HMIS warning legend. The GIR also now allows Small Quantity Generator sites to dispose of larger amounts of waste twice per year without needing to upgrade their EPA status to a Large Quantity Generator.
The College of American Pathologists (CAP) added some standards that affect lab safety practices as well. One new requirement includes the need for a laboratory security policy. Labs need to state how they restrict access of personnel into the area, and they need to spell out how to handle visitors to the department. Other new regulatory standards include the need for the safe handling of liquid nitrogen and dry ice. Labs must provide proper training and PPE for the handling of these dangerous materials, and there is even a new requirement for the placement of oxygen sensors where liquid nitrogen is used. If your CAP inspection window opens soon, you have probably already made these changes.
While keeping up with regulations might be your goal, sometimes lab inspection results can spur you on to making accomplishments for the advancement of safety. In one lab, an inspector found a freezer full of patient samples that were mixed with methanol. The freezer was not designated as explosion-proof as required by NFPA-45, the Standard on Fire Protection for Laboratories Using Chemicals. Upon further investigation, the lab safety officer found a few other freezers and refrigerators which were storing flammable materials inappropriately. This led to re-arranging some materials, and it also led to the purchase of more explosion proof units where needed.
Another lab received an OSHA inspection and received a fine for not following the training requirements of the Bloodborne Pathogens standard. The regulations state that during staff training, there must be an “opportunity for interactive questions and answers with the person conducting the training session.” Most labs offer an annual computer-based training for Bloodborne Pathogens, and that does not satisfy OSHA inspectors. The lab that was cited made a change to how the mandatory training program was offered, and they created a method for which staff could ask questions of the trainer. This was another example of an inspection which helped the lab make safety improvements.
In the world of lab safety, it sometimes feels like simply surviving day-to-day is the accomplishment. We’ve put out fires, we’ve responded to questions, and we’ve submitted our required monthly injury and exposure reports. It may feel like performing the job is simply a reaction to what is going on each day, and that is difficult for the lab safety professional. We realize that being proactive is better, we know that is how we decrease employee harm and improve the safety culture. However, I invite you to take a second look at your past twelve months. Yes, it may be that changes were made because regulatory agencies altered the standards- but there is no way to predict that unless you sit on the decision-making board of those organizations. Yes, you might have had to respond to inspection citations, but isn’t it good to have another set of eyes helping you to make safety improvements? Try not to always think about why safety improvements were made. Instead, remember to view them as positives- they are another step to improving safety the way you do it every year. They are truly accomplishments, and as you approach the new year, you can use them as stepping stones toward your next safety goals.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
For our next edition of transgender laboratory medicine, we will explore how transgender women use hormone therapy to physically transition to their affirmed female gender. While transgender men just take testosterone, transgender women take both estradiol and an anti-androgen. In the United States, that anti-androgen is spironolactone.
Figure 1. I was amazed in freshman biology by how structurally similar these hormones were and how they lead to such dramatically different phenotypes. Spironolactone is quite a bit different with the same cholesterol backbone. Credit Wikipedia
Estradiol is administered either as an oral pill, an injectable liquid or a transdermal patch. The estradiol pills are the cheapest option as they have been made generic for use as birth control. The transdermal can be the easiest to use, but is also the most expensive version and may not deliver as much estradiol as the other routes. Oral estradiol usually starts in adults at a low-dose (2 mg) then is titrated up to 4-6 mg and rarely up to 8mg. The end-point of estradiol titration is not to reach a certain hormone level, but to achieve desired physical traits. Endocrine guidelines do suggest keeping estradiol levels below peak physiologic levels (200 pg/mL).1 While little evidence currently exists for side effects of supraphysiologic estradiol, blood clots are a serious known side effect.
Part of the reason for anti-androgens in treating transgender women, is that even in women, testosterone levels are orders of magnitude higher. Spironolactone is primarily used as a glucocorticoid analog to block the mineralocorticoid receptor in the kidney to induce diuresis while retaining potassium. The structure of spironolactone is similar enough totestosterone that it also binds the androgen receptor and blocks the effect of testosterone. While enlarged breasts are considered a side effect in heart failure patients, it is an intended effect of spironolactone in transgender women. While hyperkalemia (high potassium) is a well known adverse effect of spironolactone, it seems to manifest more in patients with co-morbid conditions such as heart or kidney failure rather than in healthy patients.2
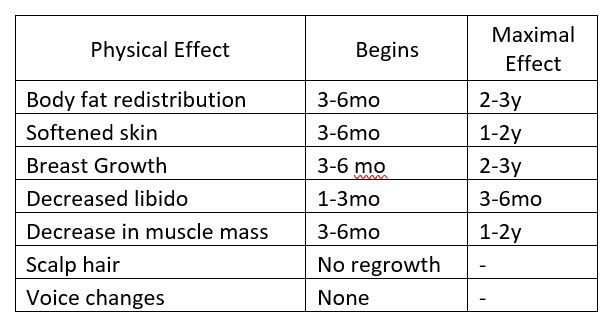
Table 1. This table describes the time frame of physical traits that manifest in transgender women while taking feminizing hormone therapy. Based on Hembree et al. 2017 (1).
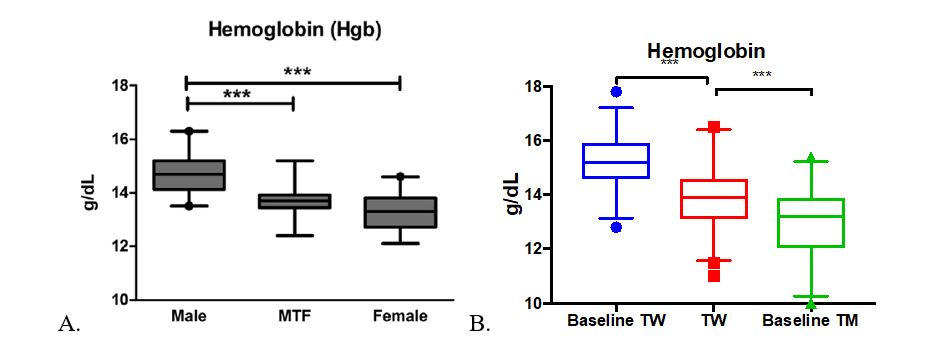
For feminizing hormone therapy, red blood cell indices are the one of the most responsive laboratory parameters. The hemoglobin, hematocrit, and RBC number are all seen to decrease during hormone therapy in transgender women. A previous study of 55 transgender women3 showed that hemoglobin levels decreased significantly from cis-gender male levels to be not significantly different from cis-gender female hemoglobin. With a larger patient group, we were able to confirm this previous finding of decreased hemoglobin, but transgender women’s hemoglobin levels are still significantly different from individuals with sex-assigned female at birth (Figure 2).
Figure 2. A. Figure from Roberts et al 2014. B. TW= Transgender women, Baseline TW= TW with no history of hormone therapy, Baseline TM= transgender men with no history of hormone therapy. ***p<0.0001 Data expressed as interquartile range with median (box) and 2.5th to 97.5th percentile (whiskers).
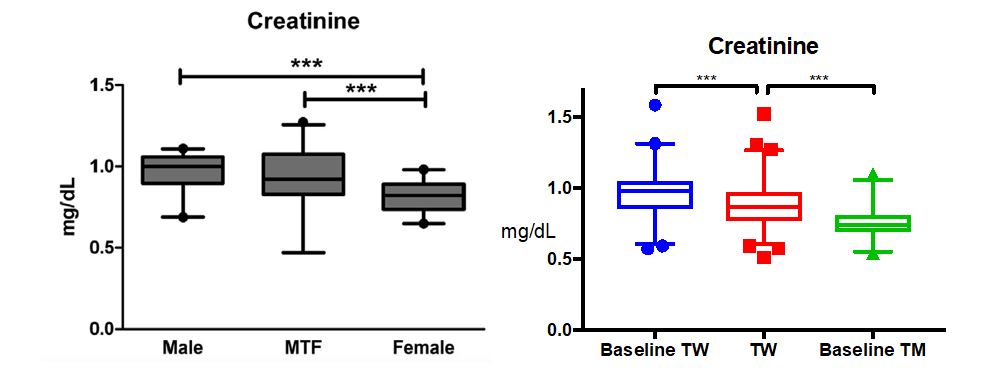
Roberts et al also found that creatinine levels remain closer to cisgender male levels compared to cisgender female creatinine values3. This brought up the concept that not all lab values change predictably to the reference interval of the opposite gender. We further confirmed this finding in our larger cohort, but we further found a significant difference in transgender women from their baseline levels (Figure 3).
Figure 3. A. Figure from Roberts et al 2014. B. TW= Transgender women, Baseline TW= TW with no history of hormone therapy, Baseline TM= transgender men with no history of hormone therapy. ***p<0.0001 Data expressed as interquartile range with median (box) and 2.5th to 97.5th percentile (whiskers).
Overall, red blood cell and creatinine levels change the most in transgender women taking hormone therapy, but they don’t go as far as being comparable to lab values of individuals of the opposite sex assigned at birth. Our summary of this data will be published soon and interested labs can note what we found to be the central 95th percentile of common lab values including those presented here. I will go into greater detail about some unexpected effects of hormone therapy in following blog posts. I hope you’re looking forward to it as much as I am!
References
Hembree WC,Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society*Clinical Practice Guideline. J Clin Endocrinol Metab. 2017
Roberts TK, Kraft CS,French D, Ji W, Wu AHBB, Tangpricha V, et al. Interpreting Laboratory Results in Transgender Patients on Hormone Therapy. Am J Med. 2014;127:159–62.
Plovanich M, Weng QY,Mostaghimi A (2015). “Low Usefulness of Potassium Monitoring Among Healthy Young Women Taking Spironolactone for Acne”. JAMA Dermatol. 151 (9):941–4.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
What do gopher holes have in common with quality improvement? More than you might think! In a paper available on Lab Medicine’s advanced access, Dr. Yaolin Zhou writes about a novel framework for quality improvement initiatives called EPIDEM, or “explore, promote, implement, document, evaluate, and modify.”
Traditionalists are the oldest working generation in today’s professional environments. They bring a wealth of information, knowledge, and experience with them. Therefore, organizations that work with Traditionalists either on their staff or on their Boards are fortunate to have access to their input. In order learn as much as possible from this generation, while they are still present in the workplace, it is critical to know and understand their preferred way of communicating, leading, and working. It is also important to know how and when to adapt your own preferred communication, behavioral, and leadership styles to meet the needs and preferences of this
generation.
Typically, Traditionalists prefer face-to-face communication. They grew up with limited communication technology and they prefer to connect in person when possible. If you cannot communicate in person, pick up the phone and call them. Not only is this respectful to their own preferences, it will allow you to increase your verbal communications skills when there is no written form used. Having a personal touch is important, so try not to talk business right away but take time to get to know one another.
When meeting with Traditionalists, some formal protocol is appreciated. Have someone else introduce you, or if you are in charge of the meeting make sure to introduce everyone properly. You can add a personal touch if appropriate. For example, say “This is Betty Jones. She is the current President of our Board of Directors and has been a member of our organization for over forty years. She is here to provide us with strategic details about our new direction. Also, she is an avid fly-fisher!” Additionally, pay attention to meeting protocols such as offering something to drink and sending the agenda ahead of time so that they can prepare. This is, of course, good to do with everyone, but Traditionalists respond especially well to such protocol.
Their leadership style is based on a chain of command and creating contingency plans. They dislike indecisiveness, disrespect, profanity, and poor dress. They appreciate a sense of formality and high quality work. I always think about how Traditionalists dressed, and sometimes still dress, when going on a plane. They dressed very formal, especially compared to today’s travelers. Keep this in mind when meeting with them in person. Forego the jeans and sweaters and wear something more traditionally professional. Finally, use formal address, such as Sir, Doctor, and Madam. Again, the more professional protocol you use, especially in the beginning, will set you up for success when working with them.
Personally, I learned and witnessed that if you include this generation in inquiry-based conversations and discussions that you can learn about additional leadership approaches to increase your own adaptability. Learn from other generations as much as possible, especially the ones that are currently leaving the workforce. There is a lot to be gained from generational diversity and increasing your own ability to meet the needs of every generation in the workplace.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
At the ASCP Annual Meeting this October, I had the privilege of facilitating a Roundtable Discussion about diversity in the workplace. I anticipated that we might be talking about issues such as culture, religion, gender, ethnicity, educational level, ability/disability and possibly age and generational issues. I was anticipating a very rich and “diverse” list of topics for this discussion.
To my surprise, generational differences was the primary topic for this Roundtable Discussion. There were nine people at our table with representation from both sub-sets of the Baby Boomer group, as well as, the Gen Xers, and Millennials (Gen Y). There seemed to be a strong disconnect between the Millennials and Gen Xers and the older people in the lab, meaning the Boomers and Traditionalists.
The Traditionalist generation only represents about 5% of the workers in clinical labs, however, the Baby Boomers still represent about half of the work force in the clinical labs. The strongest point of dissention seemed to center on “work life balance.” There was clearly a lack of knowledge and understanding on both parts. Baby Boomers are known for their work ethic and learned well from their Traditionalist’s parents and role models. They identify with their job, profession, and career. This is why we still have Traditionalists and Boomers working in the laboratories. They possess the institutional knowledge, relationships, and a strong sense of loyalty.
The Gen X and Y “work life balance” issue collided with the strong sense of work ethic characterized by the Traditionalists and Boomers. However, once each generation were able to share what they valued, there was a light bulb that appeared at the table and the bridge of understanding began to be built.
So what’s the key to collaboration? It’s all about talking with each other and asking good questions. The Traditionalists can learn from our Gen Xers and Millennials and focus on work life balance. Just as it is important for the Gen Xers and Gen Ys to learn about the institutional knowledge and work practices that can be gleaned from the Traditionalists.
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.