A 69 year old male with complicated past medical history of
sarcoidosis, pulmonary nodules, atrial flutter, right septic arthritis,
pulmonary embolism and coronary artery disease presented to the emergency
department with worsening cardiac symptoms for the past few days. He denied any
symptoms of fever, cough, dyspnea, or palpitations. He has no history of TB
exposure, high-risk occupation or volunteer work. Chest x-ray, echocardiogram and computerized tomography (CT) scan
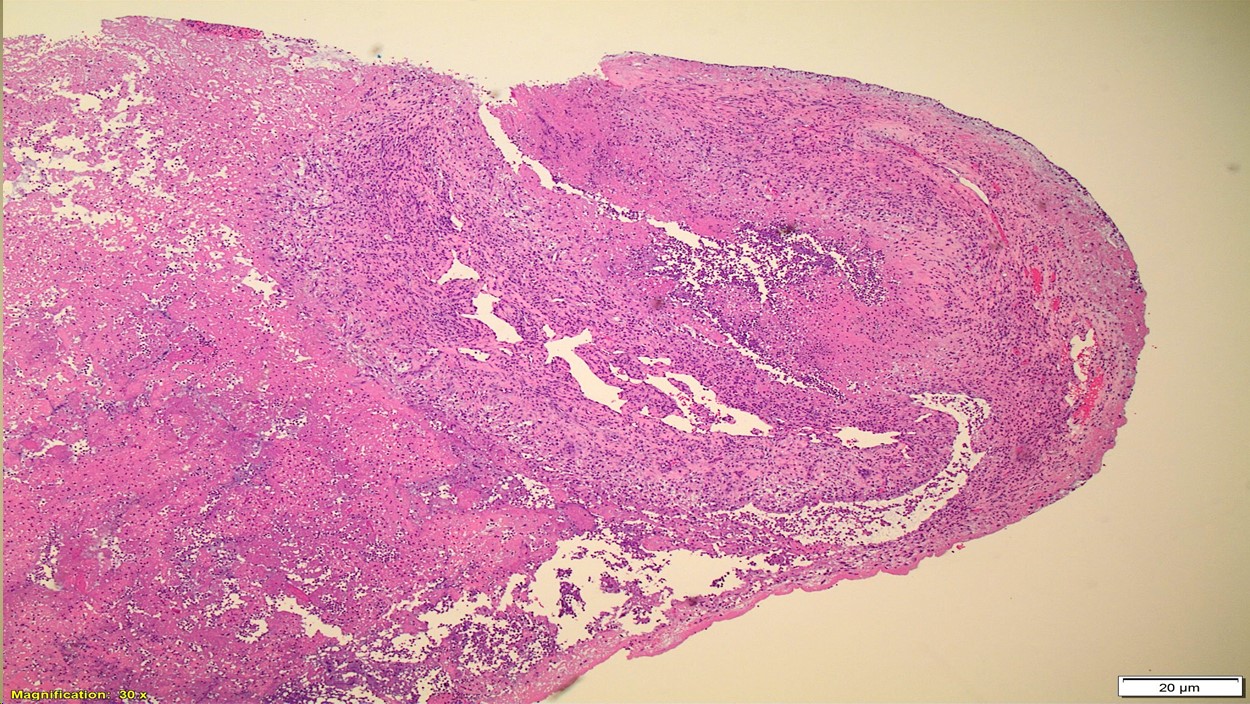
were performed and he was diagnosed with constrictive pericarditis. Pericardiotomy
was performed which showed thickened and calcified pericardium. On pericardial
biopsy specimen, acute necrotizing and granulomatous pericarditis was
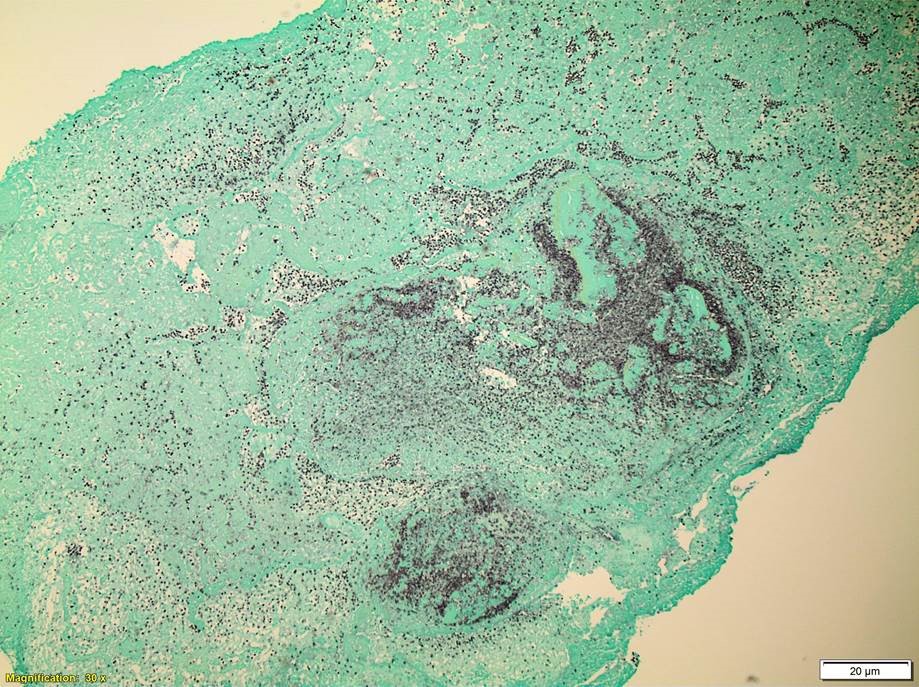
identified (Image 1). Acid fast bacteria stain for mycobacteria was performed which
showed numerous acid-fast bacilli (Image 2). In house validated testing for M. tuberculosis by PCR amplification of the IS6110
insertion sequence and nontuberculous mycobacteria species determination by
heat shock protein 65 (hsp65) gene
with melt curve analysis was performed. Testing was negative for M. tuberculosis. Nontuberculous
mycobacteria testing was consistent with M.
xenopi. For definitive diagnosis, culture was performed which grew M. xenopi (Image 3).
M. Xenopi is a
free-living nontuberculous mycobacterium (NTM). NTM are present in
the environment, mainly in water, and are occasionally responsible for opportunistic
infections in humans.1
With the availability of 16S
ribosomal DNA sequencing and high-performance liquid chromatography (HPLC),
polymerase chain reaction-restriction length polymorphism analysis (PRA), and
multi-gene and whole-genome sequencing, the number of new species of
nontuberculous mycobacteria has risen dramatically. There are
about 180 different species of mycobacteria. The most common nontuberculous species causing
human disease in the United States are the slowly growing species, Mycobacterium avium complex and M.
kansasii. Less common human pathogens include the slowly growing
species M. marinum, M. xenopi, M. simiae, M.
malmoense, and M. ulcerans, and the rapidly growing
species M. abscessus complex, M.
fortuitum, and M. chelonae.2 NTM can
cause pulmonary disease, osteomyelitis or disseminated disease in
immunocompromised patients.
Microscopic examination after acid fast or fluorescent
Auramine-Rhodamine staining and AFB culture using LJ and Middlebrook 7H10 media
are the cornerstones of the identification of mycobacteria. All mycobacteria
share the characteristic of “acid-fastness,” ie, after staining with
carbol-fuchsin or auramine-rhodamine, they do not decolorize with acidified
alcohol. Confirmation of the presence or absence of mycobacteria in clinical
specimens requires culture, because of the relative insensitivity of direct
microscopy.
The presented case highlights the importance of NTM causing
infection in pericardium which is very rare. Special stains, molecular testing,
and culture can aid in timely identification of the organism and aid in patient
management.
References
Tortoli E. Microbiological
features and clinical relevance of new species of the genus Mycobacterium.
Clin Microbiol Rev 2014; 27:727.
Griffith DE, Epidemiology of nontuberculous mycobacterial
infections. Reyn CF UpToDate. April 2017.
Griffith DE, Microbiology of nontuberculous mycobacteria.
Reyn CF UpToDate. Sept 2018.
-Amandeep
Kaur, MD MBBS is a 2nd year anatomic and clinical pathology resident at University
of Chicago (NorthShore). Academically, Amandeep has a particular interest in
hematopathology.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical
Microbiology NorthShore University Health System in Evanston, Illinois.
Follow Dr. McElvania on twitter @E-McElvania.
The patient is a 72 year old female who overall has been
fairly healthy. She has struggled with a cough for several years. A CT scan in
2015 showed some tree-in-bud changes in the lungs potentially consistent with
an atypical mycobacterial infection. She had a positive methacholine challenge
test and was diagnosed with asthma. Her cough has not improved with inhaled
asthma treatments. The cough has been persistent and is at times productive of
small amounts of whitish sputum. She has not noted any progressive shortness of
breath. Over the last several months she has tried trials of both nasal
corticosteroids, and treatment with Prilosec for gastroesophageal reflux. Both
of these trials had no effect on her cough. At the end of November 2018, a CT
scan of the chest was consistent with an atypical mycobacterial infection.
In January 2019, she came back from a skiing trip. She tried
to ski but was unable to because of shortness of breath; she came home on the third
day prematurely. During this time, she developed increased cough, fevers and
chills. An x-ray was obtained by her primary care provider, which showed a
right lower lobe infiltrate, and was placed on levofloxacin for 5 days. After
completing the antibiotic, she is still very fatigued and still coughing. She
presented to her pulmonologist in March 2019. She denied any fevers, chills or
chest pain. Her cough has continued with intermittent sputum production. Her appetite
and weight have been stable, along with bladder and bowel habits.
The patient’s past medical history is significant for arthritis, cataracts, depression, polymyalgia rheumatica, and sciatic nerve pain. Her past surgical history is only a tonseillectomy in her childhood. Her social and family history is that she runs an educational travel business, is currently divorced, has never been a smoker, and has no family history significant for recurrent infections.
Laboratory Findings
Induced sputum samples were obtained and inoculated on a
7H9 bottle that was incubated and continuously monitored for growth. Eight days
later, the 7H9 bottle flagged positive for growth. A gram stain showed
branching gram positive bacilli. The Kinyoun acid-fast stain was negative, but
a modified Kinyoun showed rare positive staining cells. The bottle was
subcultured onto chocolate agar, 7H11 agar, buffered charcoal yeast extract
(BCYE) agar, and LJ slants. Two days later, all plates except the 7H11 plate
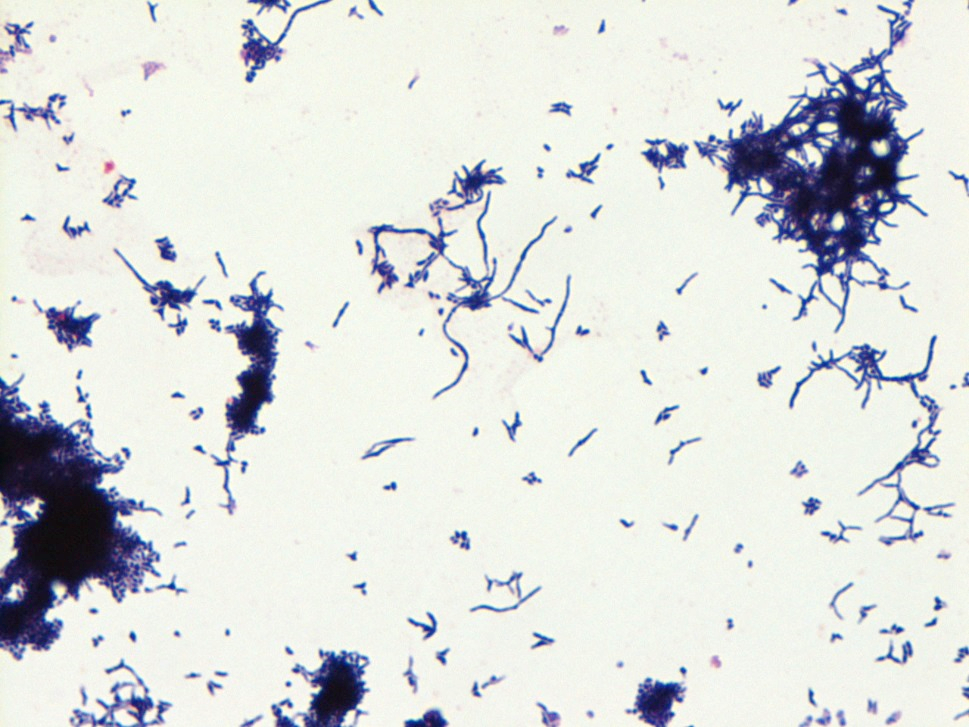
showed growth of white, dry, crinkled colonies as depicted in Image 1. A gram
stain of the colonies showed branching gram positive bacilli as shown in Image
2. Again, the Kinyoun stain of the colonies was negative but the modified
Kinyoun again highlighted cells as seen in Image 3. A representative colony was
sent for identification to Mayo laboratories a day later. MALDI-TOF performed by Mayo Laboratories
revealed the bacteria to be Rothia aeria.
An attempt was made to set up sensitivities but the organism was not able to
grow out on the test medium.
Rothia aeria
is a very rare pathogen with a current PubMed search yielding 20 references. It
was first isolated from the MIR space station (1) and genomic sequencing was
perform on the bacteria (2). It has been shown to be a normal oral flora (3),
but also seems to be most associated with endocarditis. A few case reports have
discussed sepsis, respiratory infections, and joint infections. Importantly, it
has been documented to be confused with Nocardia species (4).
References
Li, Y. et al. Rothia aeria sp. nov., Rhodococcus
baikonurensis sp. nov., and Arthrobacter russicus sp. nov., isolated from air
in the Russian space laboratory Mir. Int J Syst Evol Microbiol. 2004; 54(pt.
3): 827-835.
Nambu, T. et al. Complete Genome Sequence of
Rothia aeria Type strain JCM 11412, Isolated from Air in the Russian Space
Laboratory Mir. Genome Announc. 2016 Dec 29; 4(6).
von Graevenitz, A. et al. Coryneform bacteria in
throat cultures of healthy individuals. J Clin Microbiol. 1998; 36: 2087-2088.
Saraya, T. et al. Rothia aeria: a great mimicker
of the Nocardia species. BMJ Case Rep. Published Online: November 18, 2014.
-Jeff Covington, MD, PhD is a 2nd
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
The patient is a 3
year old male with no significant past medical history who presented to the ED
with left lower extremity pain for 24 hours after falling while playing with
family members. The patient’s mother was present at bedside providing the history,
but was not present at the time of the fall. It is unclear how the patient
injured his ankle, but family members noticed the child grabbing his ankle and
suspected that he may have twisted it. After the fall, the patient was unable/unwilling
to ambulate on the ankle. There is no history of fractures or cancer.
An x-ray and
subsequent MRI were ordered of the ankle which demonstrated an expansile lytic
lesion involving the metaphysis of the distal tibia measuring approximately 3.4
x 2.2 cm (Figure 1 and 2). The margins of this lesion are indistinct, and there
is cortical irregularity at the anterior and lateral aspect of the distal metaphysis
of the tibia, likely representing a pathologic fracture. The differential
diagnosis includes infection, aneurysmal bone cyst, nonossifying fibroma,
osteoblastoma and histiocytosis.
The patient and family
then followed up with Orthopedics, who proceeded to perform a biopsy of the
lytic lesion in order to determine the nature of the lesion. The results are
below.
Figure 1. Xray of the distal tibia demonstrating the lesion.
Figure 2. MRI demonstrating the lytic lesion involving the metaphysis of the distal tibia.
Diagnosis
Received fresh for intraoperative consultation is a 1.1 x 0.6
x 0.5 cm aggregate of white-tan soft tissue fragments. Half of the tissue
fragments are frozen and read out as “spindle cell proliferation.
Consideration of low-grade vasoformative lesion. Defer to permanent,” with
3 pathologists consulting on the diagnosis. The remainder of the tissue not
submitted for frozen section, as well as the entirety of a second container from
the same lesion, is submitted for routine processing.
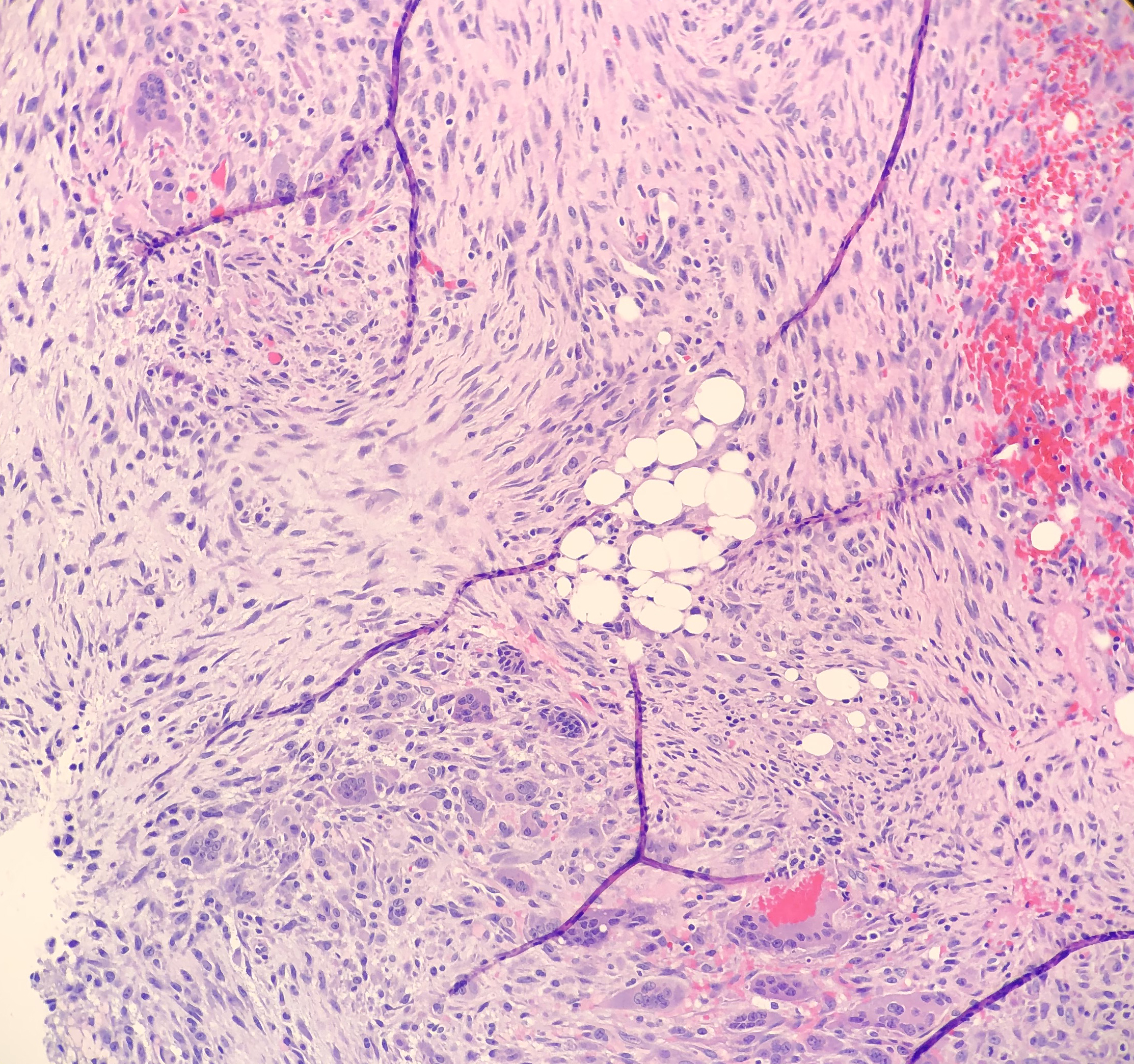
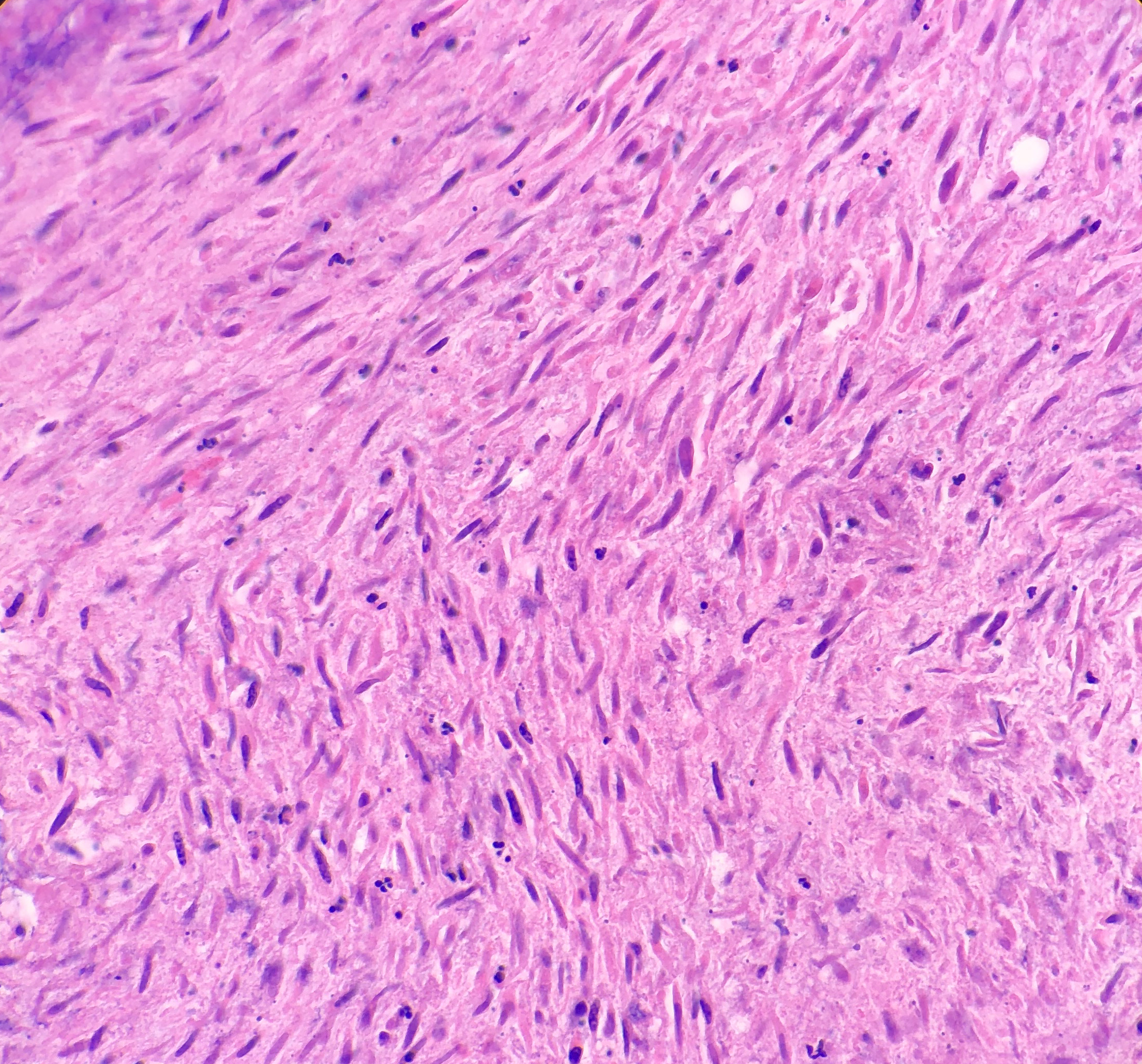
On microscopy, the biopsies demonstrate a moderately cellular
proliferation of fasciculated spindle cells in a collagenous to myxoid stroma.
Nuclei are predominantly oval with variably fine to granular chromatin. Many
cells have moderate amounts of tapering eosinophilic cytoplasm, resembling
strap cells. Inflammatory cells and osteoclast-like giant cells are admixed
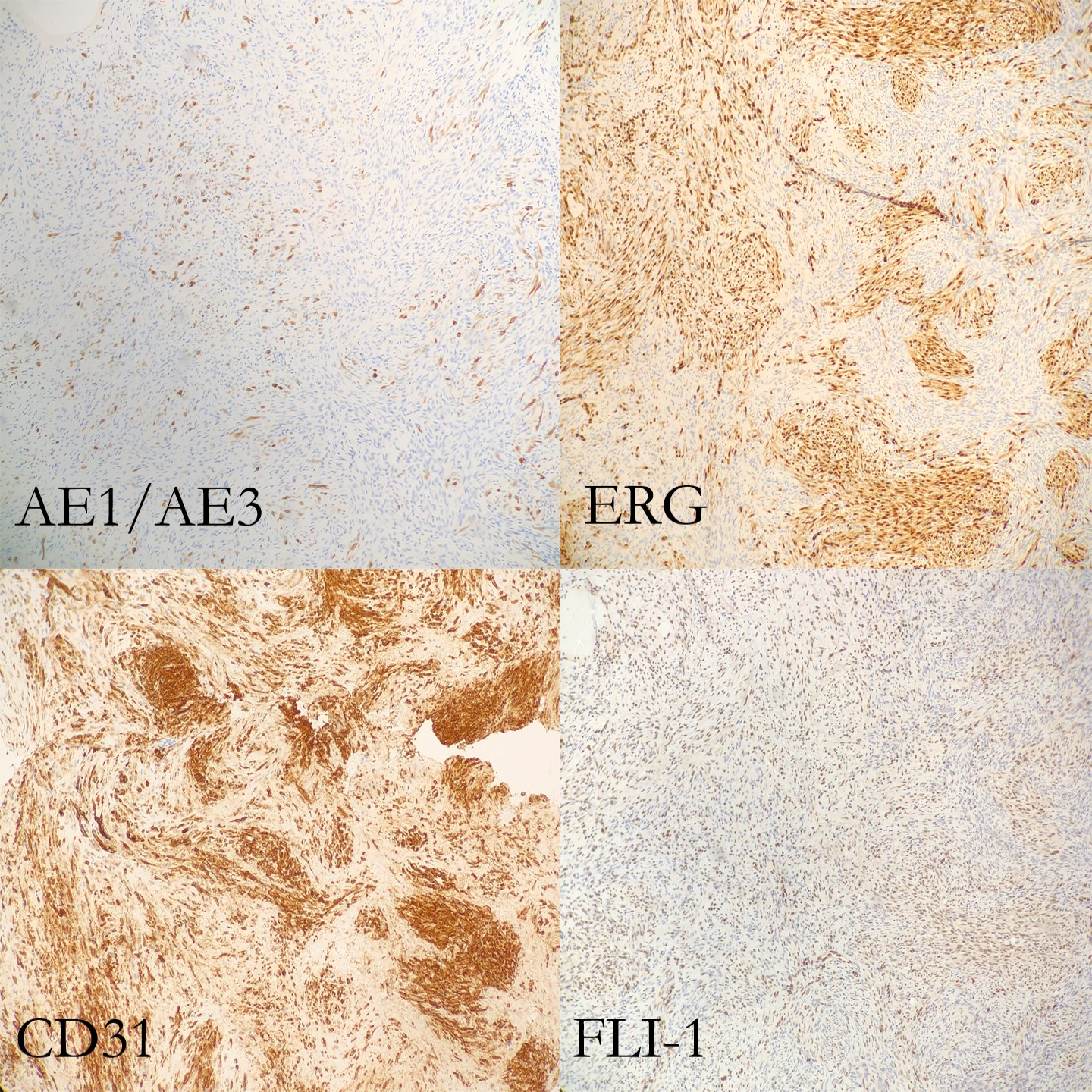
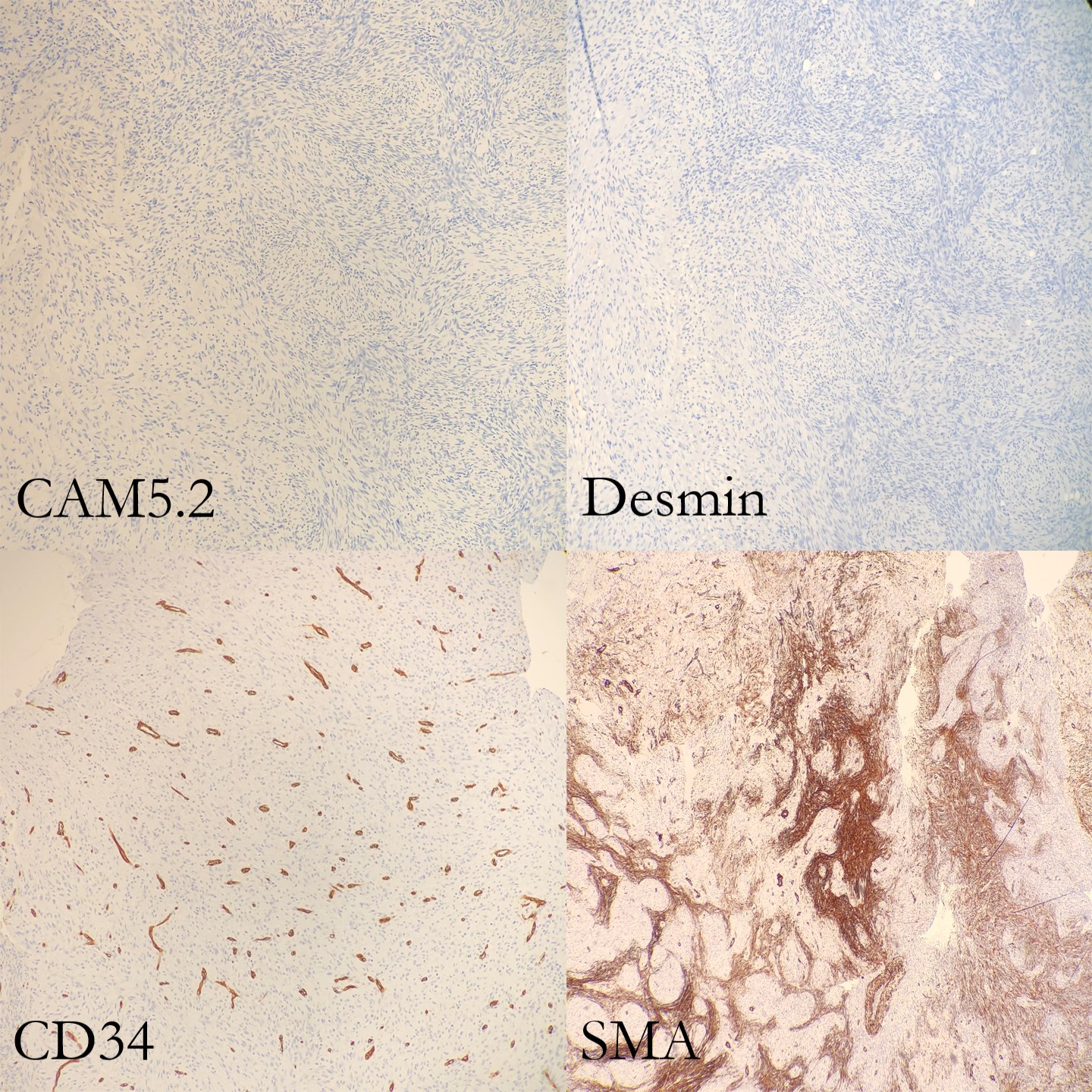
(Figure 3 and 4). Immunohistochemical stains demonstrate lesional spindle cells
to be positive for CD31, ERG, and FLI1. AE1/AE3 and CAM5.2 highlight rare
lesional spindle cells. SMA stains some stellate spindle cells, favored to
represent associated myofibroblasts. Desmin, MDM2, CDK4, ALK, and S100 are negative
in plump lesional cells (Figure 5 and 6). Overall, the features are consistent
with pseudomyogenic hemangioendothelioma, a rare vascular tumor. Although more
commonly present in soft tissue, primary bone cases have been reported. These
neoplasms have some risk for local recurrence, but only rarely distant
metastasis. A portion of tissue was sent to the University of Nebraska Medical
Center to evaluate for a characteristic gene rearrangement (SERPINE1-FOSB) that
is present in at least a subset of pseudomyogenic hemangioendotheliomas. This
was negative.
The lesion was then curettaged by the
surgical team.The patient and his family had two follow up office visits with
the Orthopedics department. The first one, a week after surgery, was
unremarkable. The second visit, two weeks after surgery, was notable for the
patient developing a cutaneous rash on both arms and chest. Due to literature
citing that these tumors generally arise in the soft tissue, the clinician
suggested that the patient and family follow up with pediatric dermatology to
ensure that this new rash is not related to the pseudomyogenic hemangioendothelioma.
Unfortunately due to insurance, the patient and family had to see a dermatologist
at a different institution, and no further visits have taken place.
Figure 3. Photomicrograph of the strap-like cells with tapering eosinophilic cytoplasm , and osteoclast-like giant cells. Figure 4. Higher power photomicrograph demonstrating the appearance of the strap-like cells with tapering eosinophilic cytoplasmFigure 4.
Discussion
Pseudomyogenic hemangioendothelioma (PHE) is a rare vascular
tumor that most commonly arises in the skin and soft tissues of the
extremities. It is usually multifocal, appearing in multiple tissue planes,
such as the mucosa, dermis, subcutis and skeletal muscle, in a variety of
different anatomic sites. Although even less common, PHE can also involve bone
(such as this case). PHE has a male predilection, typically appearing in the second
to fourth decades of life. Of the most common symptoms that the patient
presents with, pain appears to top the list, although it should be stated that
only about half of the patients experience pain.
Grossly, skin and soft tissue PHE tumors appear firm,
ill-defined and gray-white. When they involve bone, they appear as multiple
discrete, pink-tan to dark brown hemorrhagic tumors with surrounding sclerosis,
ranging from 0.1 to 6.5 cm in greatest dimension.
Histologically, PHE demonstrates plump spindle and rhabdomyoblast-like
cells with densely eosinophilic cytoplasm that grows in sheets and fascicles. The
cells can be mistaken as rhabdomyoblasts because of the eosinophilic cytoplasm
that pushes the nucleus to the periphery of the cell. Immunohistochemical studies are very helpful in order to
determine a diagnosis of PHE. AE1/AE3, ERG, FLI-1 and CD31 are positive,
whereas CD34, desmin and S100 are negative. Karyotyping has revealed a
fusion of genes SERPINE1-FOSB that
corresponds to the recurrent translocation t(7;19)(q22;q13). In this case, the SERPINE1-FOSBgene rearrangement was negative, but could possibly be due to
a variant fusion gene.
Making a histologic
diagnosis can be difficult for a Pathologist, due to the wide variety of
differential diagnoses that will need to be excluded first.
The differential diagnosis
for a cutaneous tumor includes:
Cellular benign
fibrous histiocytoma (lacks rhabdomyoblast-like cells and neutrophilic
infiltrates, contains mitotic figures, and is negative for cytokeratin and CD31)
Spindle cell
squamous cell carcinoma (usually in sun-damaged skin, with nuclear atypia and
negative endothelial markers)
Epithelioid
sarcoma (negative INI1, positive EMA and CD34, and a nodular architecture with
central necrosis and more nuclear atypia)
The differential diagnosis
for soft tissue tumors include:
Epithelioid
sarcoma (see above)
Epithelioid
hemangioendothelioma (usually intracytoplasmic vacuoles, positive CD34 and
CAMTA1, and a t(1;3)(p36.3;q25) translocation resulting in WWTR1-CAMTA1 gene fusion)
Epithelioid
angiosarcoma (vasoformative architecture with sheet-like pattern, nuclear
atypia, high nuclear grade, frequent mitosis and irregular vascular channels)
The differential diagnosis for bone tumors
includes:
Giant cell tumor
(lacks rhabdomyoblast-like cells and fascicles of spindle cells)
Osteoblastoma
(lacks rhabdomyoblast-like cells and fascicles of spindle cells)
In a study by Inyang et al,
when PHE involved bone, imaging would demonstrate multiple to innumerable
discontinuous tumors throughout the affected bone, involving the cortex and/or
medullary cavity of the epiphysis, metaphysis, or diaphysis. On x-ray and
computed tomography, the lesions appeared as well circumscribed, lobulated and
lytic, with a sclerotic rim on some of the lesions. On magnetic resonance
imaging, T1-weighted images would appear dark, and T2-weighted images would
appear hyperintense.
PHE has a tendency to recur
locally, but rarely develops distant metastases. Since PHE presents as a
multifocal disease and can be easily confused for a distant metastasis, care
needs to be taken to ensure that a diagnosis of PHE is not overlooked.
Surgical ablation and
excision is the standard treatment for a patient with PHE, with a few cases
noted of patients being treated with radiotherapy and/or adjuvant chemotherapy,
in addition to surgery. Everolimus and sirolimus have recently been found to be
effective in cases of patient with PHE that had metastatic and relapsing multifocal
PHE.
Figure 5. Immunohistochemical stains (part 1 of 2)Figure 6. Immunohistochemical stains (part 2 of 2)
References
Hornick JL, Fletcher CDM. “Pseudomyogenic Hemangioendothelioma:
A Distinctive, Often Multicentric Tumor With Indolent Behavior.” Am J Surg
Pathol. 2011; 35: 190201.
Inyang A, et al. “Primary Pseudomyogenic Hemangioendothelioma
of Bone.” Am J Surg Pathol. 2016; 40: 587598.
Pradhan D. “Pseudomyogenic hemangioendothelioma
of skin, bone and soft tissue; a clinicopathological, immunohistochemical, and
fluorescence in situ hybridization study.” Hum Pathol. 2018; 71: 126134.
Sugita S, Hirano H, Kikuchi N, et al. Diagnostic utility of
FOSB immunohistochemistry in pseudomyogenic hemangioendothelioma and its histological
mimics. Diagn Pathol. 2016;11(1):75. Published 2016 Aug 11.
doi:10.1186/s13000-016-0530-2
-Cory Nash is a board certified Pathologists’ Assistant,
specializing in surgical and gross pathology. He currently works as a
Pathologists’ Assistant at the University of Chicago Medical Center. His
job involves the macroscopic examination, dissection and tissue
submission of surgical specimens, ranging from biopsies to multi-organ
resections. Cory has a special interest in head and neck pathology, as
well as bone and soft tissue pathology. Cory can be followed on twitter
at @iplaywithorgans.
A 75 year old female with a past medical history of breast
cancer presented to the Emergency Department with chills 3 weeks status-post
bilateral breast reconstruction due to ruptured silicone breast implants. Her
white blood cell count was 13,440/cmm and her temperature was 39.4ºC. Physical
examination revealed erythema of the right breast incision and purulent
drainage from the Jackson-Pratt (JP) drain. Two blood cultures were drawn and a
specimen was collected from the JP drain fluid and sent for gram smear and
culture.
Laboratory
Findings
Blood
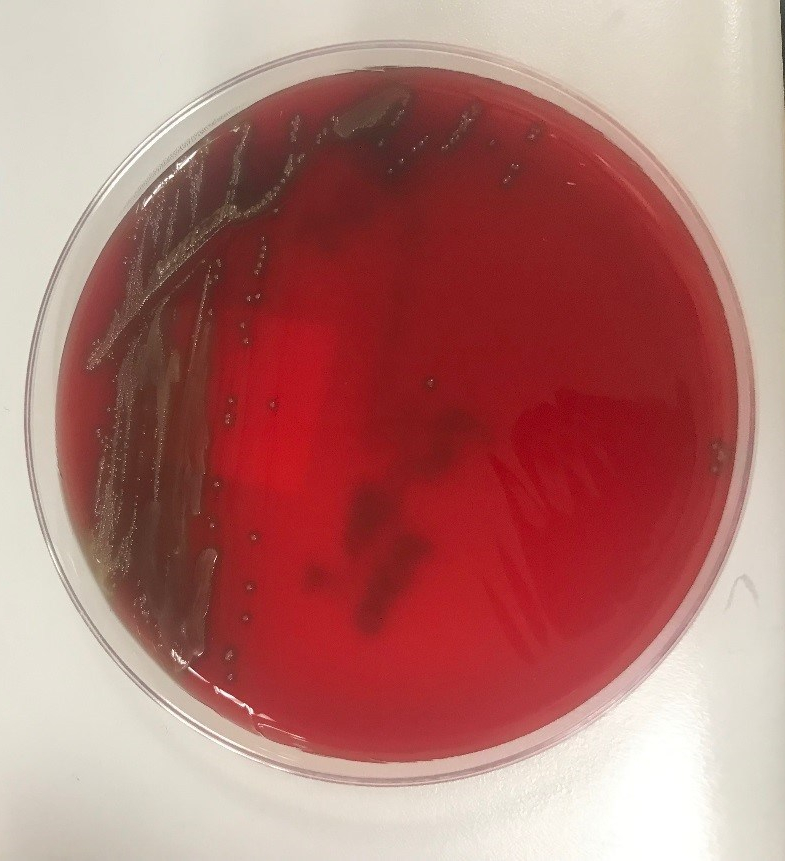
cultures were negative for growth. Gram stain of the drain fluid was
significant for many polymophonuclear neutrophils, however no bacteria were
seen. Aerobic cultures grew gram positive cocci. Matrix assisted laser
desorption ionization-time of flight mass spectrometry (MALDI-TOF) analysis
identified Streptococcus gordonii. The
patient was started on doxycycline and amoxicillin-clavulanate. Antibiotic susceptibility
testing subsequently showed susceptibility to ceftriaxone and penicillin.
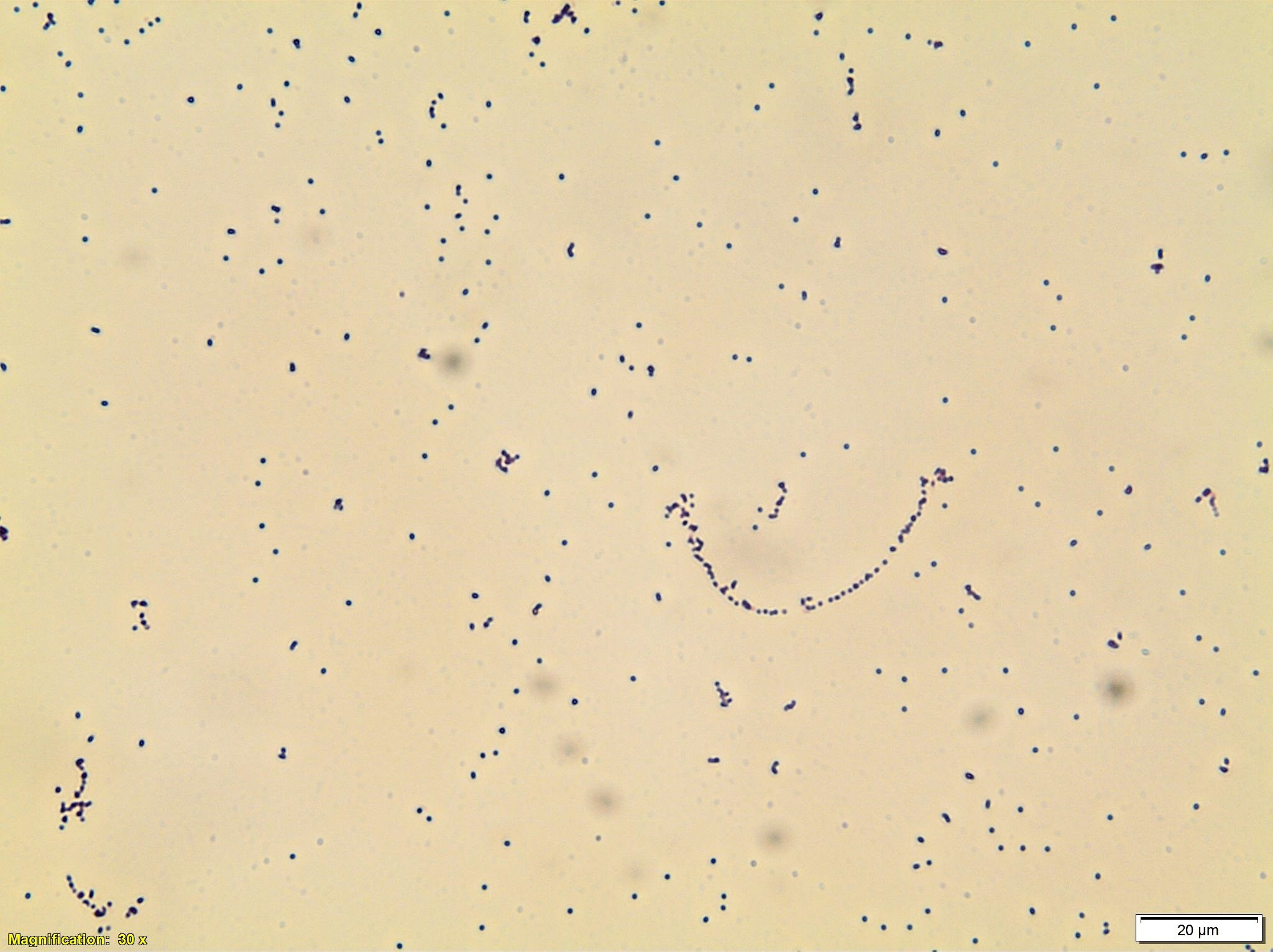
Image 1. Blood agar showing alpha-hemolytic colonies. Image 2. Gram stain from media showing gram positive cocci.
Discussion
Streptococcus gordonii is a gram positive, non-motile, facultative
anaerobic cocci that is part of the Streptococcus
sanguinis group of viridans group streptococci (VGS). It is a common oral
bacteria that has been implicated in invasive infections such as endocarditis
and septic arthritis. It is less frequently a cause of soft-tissue infections
such as orbital cellulitis, osteomyelitis, and subcutaneous abscesses. There
are case reports of joint prosthesis infections, however breast implant
infections have not been reported. Breast implant infections are most commonly
caused by Staphylococcus aureus,
Pseudomonas aeruginosa, and Staphylococcus
epidermidis. There are reports of different VGS species causing breast
implant infections. As the bacteria primarily resides in the mouth, infections
are usually caused by oral trauma. Although symptoms may often be minor, in
cases caused by VGS, systemic symptoms can occur including a toxic shock-like
syndrome. In these cases there is a case fatality rate as high as 80%. S. gordonii has been reported as
susceptible to clindamycin, ceftriaxone, erythromycin, and levofloxacin. Prompt
treatment is important to prevent progression to systemic illness and
mortality.
References
Seng
P, Bayle, S, Alliez, A, et al. The microbial epidemiology of breast implant
infections in a regional referral centre for plastic and reconstructive surgery
in the south of France. Int J Infect Dis. June 2015;35:62-66.
Fenelon
C, Galbraith JG, Dalton DM, Masterson E. Streptococcus
gordonii—a rare cause of prosthetic joint infection in a total hip
replacement. J Surg Case Rep. 2017 Jan;1:235.
Liao
CY, Su KJ, Lin CH, et al. Planta purpura as the initial presentation of viridans
streptococcal shock syndrome secondary to Streptococcus
gordonii bacteremia. Can J Infect Dis Med Microbiol. 2016:946385.
Dadon
Z, Cohen A, Szterenlicht YM, et al. Spondylodiskitis and endocarditis due to Streptococcus gordonii. Ann Clin
Microbiol Antimicrob. 2017:16:68.
Krantz
AM, Ratnaraj F, Velagapudi M et al. Streptococcus
gordonii empyema: a case report and review of empyema. Cureus. 2017
Apr;9(4):e1159.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
A 49 year old male
presented to the emergency department (ED) with complaints of chest pain,
shortness of breath, and chills for the past two weeks. He describes the pain
as sharp and located on the left side of his chest. Past medical history is
non-contributory, except for current IV drug use. His temperature was 97.7°F,
blood pressure 141/63, heart rate 87, respirations 18 with an oxygen saturation
of 91-93% on room air. On physical exam, a regular rate & rhythm with no
murmur or regurgitation was noted and lungs showed fine bilateral crackles. His
white blood cell count was increased at 22.1 TH/cm2 and troponin I
was also elevated at 0.19 ng/ml. Blood cultures were collected and the patient
was started on ceftaroline and piperacillin tazobactam for presumed infective
endocarditis. He was transferred to the medical intensive care unit and
intubated due to respiratory distress. An echocardiogram revealed a large
mobile vegetation on the aortic valve with severe insufficiency and a
vegetation & thickening of the mitral valve with severe regurgitation.
Laboratory Identification
Image 1. Gram stain showed gram positive cocci arranged in pairs and chains (1000x oil immersion).Image 2. Small, gray, non-hemolytic colonies grew on blood and chocolate agar after 48 hours of incubation at 35°C in 5% CO2. There was no growth on MacConkey agar. Image 3. Portions of valve leaflets showing acute neutrophilic fibrinous exudate (H&E, 300x). Image 4. Special stain highlighting numerous bacterial cocci (GMS, 300x).
Blood cultures were positive within 24 hours of collection and
gram positive cocci arranged in pairs and chains were noted (Image 1). Enterococcus spp., vancomycin resistance
not detected was reported by polymerase chain reaction (PCR). Small, gray,
non-hemolytic colonies grew after 2 days of incubation (Image 2). MALDI-TOF
mass spectrometry identified the isolate as Enterococcus
faecalis.
Discussion
Enterococcus spp. are gram positive, catalase negative cocci that are
arranged in pairs & chains and are facultative anaerobes. Enterococcus spp. are widespread in
nature and a component of the normal flora of the gastrointestinal tract and
less commonly found in the oral cavity and on the skin. Commonly, Enterococcus spp. are opportunistic
pathogens and cause infections of the urinary tract, intraabdominal cavity,
surgical sites, bacteremia, and infective endocarditis.
In the microbiology
laboratory, Enterococcus spp. grow
readily on non-selective media and are usually alpha-hemolytic or non-hemolytic
on blood agar. The two main species, E.
faecalis and E. faecium, will grow
in 6.5% NaCl, hydrolyze esculin in the presence of bile salts, and are positive
for both leucine aminopeptidase (LAP) and L-pyrrolidonyl-beta-naphthylamide
(PYR). Biochemically, arabinose utilization serves as a useful indicator to
distinguish E. faecalis (negative)
and E. faecium (positive). A variety
of identification systems are able to identify the great majority of Enterococcus spp. to a species level.
Ampicillin or
vancomycin are acceptable treatment options for Enterococcal infections if
found to be susceptible by antibiotic testing. It is important to note, Enterococcus spp. are intrinsically
resistant to cephalosporins, aminoglycosides, trimethoprim-sulfamethoxazole,
and clindamycin. For serious infections, including infective endocarditis, it
is recommended to treat with a cell wall active agent such as ampicillin and an
aminoglycoside (gentamicin or streptomycin) to create a synergistic
bactericidal effect. Emergence of E.
faecium acquired vancomycin resistance (VanA/VanB) is increasing and more
board spectrum agents such as daptomycin and linezolid are necessary to
effectively treat these infections.
In
the case of our patient, upon identification of E. faecalis from multiple blood cultures, his antibiotics were
switched to IV ampicillin and gentamicin. He underwent valve replacement
surgery and both the aortic and mitral valves grew E.faecalis as well and
showed numerous bacterial cocci on histology (Images 3 & 4). He completed a
six week course of ampicillin and gentamicin and was discharged home in good
condition.
-Hansini Laharwani, MD is a first year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
A 70 year old
male with a history of multiple system atrophy and left hip fracture presented
to his primary care physician after being found by his home health nurse to have
a sacral decubitus ulcer. Physical examination revealed an afebrile immobile
patient with a 3.0 cm stage III ulcer over the sacrum with purulent exudate.
Tissue was obtained and sent to our laboratory for Gram stain and culture.
Laboratory Findings
Gram stain
was significant for many polymorphonuclear neutrophils and mixed gram positive
and gram negative organisms. Blood and chocolate plates grew mixed organisms
with a predominant gram positive coccobacillus. Matrix assisted laser
desorption ionization-time of flight mass spectrometry (MALDI-TOF) identified
this organism as Trueperella bernardiae.
Image 1. Gram stain from tissue showing mixed gram positive and gram negative organisms. Image 2. Blood agar showing non-hemolytic white colonies.
Discussion
Trueperella bernardiae is a nonspore-forming,
facultatively anaerobic, gram-positive coccobacillus. It was previously
categorized within the Actinomyces and
Arcanobacterium genera. It is
classically associated with pig farming. It is often considered to be a
contaminant or normal flora, however, it has been reported as a cause of bone
and soft tissue infections. Highly invasive diseases are rare. The incidence of
infection may have been underreported previously due to the difficulty to
culture and identify it from normal flora prior to the advent of MALDI-TOF.
Antibiotic sensitivity data is limited, however, there are reports of
susceptibility to beta-lactams, clindamycin, tetracycline, and vancomycin.
Minimum inhibitory concentration interpretation is often based on data from
bacteria of the Corynebacterium.
References
Rattes
ALR, Araujo MR, Federico MP, et al. Trueperella
bernardiae: first report of wound infection post laparoscopic surgery. Clin
Case Rep. 2016 Aug;4(8):812-815.
Lawrence
CHD, Waseem S, Newsholme W, Klein JL. Trueperella
bernardiae: an unusual cause of septic thrombophlebitis in an injection
drug user. New Microbes New Infect. 2018 Nov;26:89-91.
Cobo
F, Rodriquez-Granger J, Sampedro A, et al. Two Rare Cases of Wound Infections
Caused by Trueperella bernardiae. Jpn
J Infect Dis. 2017;70:682-684.
Gowe
I, Parsons C, Best M, et al. Successful treatment of olecranon bursitis caused
by Trueperella bernardiae: importance
of environmental exposure and pathogen identification. Case Reports in
Infectious Diseases. 2018;5353085.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
A 90 year old male is transferred from his nursing care facility to the hospital for management of acute appendicitis. He had acute onset of right lower quadrant abdominal pain the morning prior to admission with fevers, rigors and drenching sweats. Imaging showed ruptured appendicitis with a fecalith surrounded by small pockets of fluid. His past medical history included dementia, heart disease, hyperlipidemia, hypertension, and glucose intolerance. He denied having any prosthetic joints or valves. Blood was obtained for microbiological analysis.
Laboratory
Identification
Blood culture bottles flagged positive. Gram stain of the
blood culture bottles showed medium to long gram negative bacilli (Image 1).
The blood culture media was plated on blood, chocolate, and MacConkey agar. Aerobically,
yellow colonies grew on the blood and chocolate agar. The yellow colonies
turned red when exposed to 10% KOH (Image 2). Definitive diagnosis of Chryseobacterium gleum was obtained by
MALDI-TOF.
Image 1. Gram stain from the blood culture bottle shows gram negative bacilli.
Image 2. Growth of the organism on chocolate agar with addition of 10% KOH solution (circled in black).
Discussion
Chryseobacterium
gleum is a gram negative bacillus. They form yellow colonies that
grow on blood and chocolate agar. They rarely grow on MacConkey agar and are
non-fermenters when they do grow. Species of Chryseobacterium will turn red with addition of 20% KOH due to a pigment
protein called flexirubin. Interestingly, our lab had only 10% KOH and the
colonies turned red with this as well. Other key biochemical and physiologic
characteristics of Chryseobacterium
include being indole and oxidase positive and they are non-motile.
Chryseobacterium species
are found in the environment and are usually not part of normal flora, therefore
infection requires exposure of the bug to a debilitated patient in order to
colonize the respiratory tract. However, infection of other body sites that may
or may not have preceded respiratory tract colonization have been reported. These
organisms can survive in chlorinated tap water. They are an emerging cause of
hospital associated infections. No virulence factors have been studied. Risk
factors for infection include immunosuppression, trauma, surgery, burns,
foreign body implants and infused fluids. Of note, the patient was thought to
obtain his Chryseobacterium bacteremia
from his ruptured appendicitis.
For therapy, there are no definitive guidelines due to lack
of understanding of resistance mechanisms. These antibiotics have been reported
to have potential activity: Ciprofloxacin, rifampin, clindamycin,
trimethoprim/sulfamethoxazole and vancomycin (reportedly for C. indologenes). Our patient was given
Piperacillin/tazobactam, Ceftriaxone and metronidazole for two days, Cefepime
for one day, Vancomycin for a day. Infectious disease recommended continuing
piperacillin/tazobactam and starting trimethoprim/sulfamethoxazole and
discontinuing vancomycin.
Antimicrobial susceptibility testing was performed and
showed resistance to meropenem, aztreonam, gentamicin, and tobramycin. The
organism was susceptible to piperacillin/tazobactam and
trimethoprim/sulfamethoxazole.
Murray
P. Medical Microbiology. Seventh Edition. Elsevier; 2013.
Jain V, Hussain NAFA, Siddiqui T, Sahu C, Ghar M, Prasad
KN. Simultaneous isolation of Chryseobacterium gleum from bloodstream
and respiratory tract: first case report from India. JMM Case Rep.
2017;4(10):e005122. Published 2017 Oct 16. doi:10.1099/jmmcr.0.005122
-Angela Theiss, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
A 71 year old man with a history of multiple myeloma
presented with urinary incontinence and confusion and was found to have
hyperkalemia with renal failure. Imaging showed extensive inguinal
lymphadenopathy with concern for new lymphoma.
Excisional Lymph Node Biopsy
H&E 40x
Diagnosis
Sections
show an enlarged lymph node with complete effacement of the normal lymph node
architecture by sheets of medium and large plasmablastic cells. The cells have
round nuclear contours, large prominent nucleoli and moderate amounts of
amphophilic cytoplasm. Frequent apoptotic cells and scattered mitoses are seen.
Immunohistochemical stains show that the neoplastic cells
are immunoreactive for CD138, CD38, CD19 (dim) and MUM1. They are negative for
CD20, which highlights only small admixed B-cells. The cells are kappa
restricted by kappa and lambda immunostain. The Ki-67 proliferation index is
greater than 90%.
Taken together, the morphologic and immunophenotypic
features are of a high grade plasmablastic neoplasm. The differential diagnosis
includes plasmablastic myeloma and a plasmablastic lymphoma. Given the
patient’s history of a kappa restricted plasma cell dyscrasia, plasmablastic
myeloma is favored.
Discussion
Multiple myeloma is a neoplasm of clonal plasma cells that
accounts for 10% of all hematologic malignancies. It is most commonly seen in
adult and elderly patients with a male predominance. Plasma cells are generally
characterized by the presence of a “clockface” nuclei and distinct perinuclear
Hof or clearing of the cytoplasm containing a large number of Golgi bodies. The
morphology of plasma cell tumors can range from small mature plasma cells to
anaplastic or plasmablastic morphology. In this case, the cells showed
plasmablastic (PB) morphology, which is characterized by a large nucleus, large
nucleolus, fine reticular nuclear chromatin pattern, lack of nuclear Hof and
less abundant cytoplasm than typical plasma cells.1
The differential diagnosis for cases with this morphology primarily
includes PB lymphoma and PB myeloma with extramedullary involvement. PB
lymphoma is seen more commonly in HIV positive patients or patients with other
causes of immunodeficiency. It typically occurs in adults and has a male
predominance. The tumor generally presents outside of nodes and is most
frequently seen in the oral cavity/jaw. Patients tend to present with advanced
stage and bone marrow involvement. While PB lymphoma is categorized as a
distinct subtype of diffuse large B-cell lymphoma, PB myeloma is considered an
atypical morphologic variant of multiple myeloma and is treated with therapy
geared towards plasma cell neoplasms. 2
Making the distinction between these entities is difficult due to similarities in morphology and immunophenotype. Ultimately, the diagnosis is generally made based on the clinical context. In one series of “plasmablastic” neoplasms by Ahn, et. al., 6 out of 11 cases were called PB lymphoma, 2 out of 11 were called multiple myeloma and 3 were called indeterminate. Among the PB lymphoma patients, 4 were either HIV positive or had a history of immunosuppression. All 6 cases were positive for CD138 and negative for CD20 with EBV in situ hybridization positivity in 3 out of 6 cases. The multiple myeloma cases had evidence of end organ damage without lymphadenopathy. One indeterminate case had peritoneal nodules, lytic lesions and an EBV positive neoplasm in the bone marrow, which precluded a definitive diagnosis. 3
The immunophenotypic pattern seen in this case is typical of
these neoplasms and is characterized by the expression of plasma cell antigens (CD138,
CD38, MUM1) with either weak or negative expression of B-cell antigens (CD20). A
study by Vega et. al. looked at the immunophenotypic profiles in nine cases of
PB lymphoma and seven cases of PB myeloma. They found that the profiles were
nearly identical. All cases were
positive for MUM1/IRF4, CD138 and CD38 and negative for CD20, consistent with a
plasma cell immunophenotype. PAX5 and BCL6 were weakly positive in 2/9 and 1/5
PB lymphomas and were negative in all PB myelomas. A high Ki-67, overexpression
of P53 and loss of p16 and p27 were present in both tumors. There was no
evidence of HHV8 detected in either neoplasm. The presence of EBV-encoded RNA,
was seen in all PB lymphoma cases tested and negative in all plasma cell
myeloma cases. This was found to be statistically significant. 4
Unfortunately, both PB lymphoma and PB myeloma are aggressive
high grade neoplasms with a poor prognosis. A study conducted by Greipp et. al.
assessed the prognostic significance of plasmablastic morphology in a cohort of
patients from the Eastern Cooperative Oncology Group Myeloma Trial E9486. They
looked at bone marrow aspirates from 453 newly diagnosed multiple myeloma cases
in a 5 year period. Of the 453 aspirates, 8.2% were classified as PB
morphology. The overall survival of
patients with PB morphology was significantly shorter than patients with non-PB
morphology with a median of 1.9 years compared to 3.7 years. There did not
appear to be a relationship between PB morphology to other clinical or
laboratory features such as age, sex, bone lesions or type of M-protein. 5
References
M Srija, P Zachariah, V Unni, et. al.
Plasmablastic myeloma presenting as rapidly progressive renal failure in a
young adult, Indian Journal of Nephrology,
Volume 24(1): 2014, Page 41-44.
JJ Castillo, M Bibas, RN Miranda, The biology
and treatment of plasmablastic lymphoma, Blood,
Volume 125, 2015, Page 2323-2330.
J Ahn, R Okal, J Vos, et. al. Plasmablastic
Lymphoma vs Myeloma With Plasmablastic Morphology: An Ongoing Diagnostic
Dilemma, American Journal of Clinical Pathology,
Volume 144(2): 2015, Page A125.
F Vega, CC Chang, LJ Medeiros, et. al.
Plasmablastic lymphomas and plasmablastic plasma cell myelomas have nearly
identical immunophenotypic profiles. Modern
Pathology, Volume 18: 2005, Page 806-815.
PR Greipp, T Leong, J Bennett, et. al. Plasmablastic Morphology – An
Independent Prognostic Factor With Clinical and Laboratory Correlates: Eastern
Cooperative Oncology Group (ECOG) Myeloma Trial 39486 Report by the ECOG
Myeloma Laboratory Group, Blood, Volume 91: 1998, Page 2501-2507.
–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
The infectious disease service was consulted on an 81 year old female for persistent fevers. She initially presented a few weeks prior with cough & shortness of breath which was diagnosed as an acute chronic obstructive pulmonary disease (COPD) exacerbation for which she received levofloxacin and steroids. The patient continued to have a persistent cough and dysphagia after discharge. Her respiratory status and cough worsened and she was readmitted and intubated. Vancomycin, piperacillin/tazobactam and levofloxacin were started as well as fluconazole for suspected esophageal candidiasis. Her past medical history was significant for breast cancer, atrial fibrillation, and diabetes mellitus. Of note, patient was originally from Puerto Rico but moved to the United States 40 years ago and denied recent travel and any known tuberculosis exposures. She formerly worked in a deli packing cheeses. A bronchoscopy was performed and a brochoalveolar lavage (BAL) specimen as well as blood and stool specimens were submitted for bacterial culture and ova and parasite exam.
Laboratory
Identification
Image 1. Multiple larval forms in the stood specimen from an ova and parasite exam. (Iodine stain, 100X).
Image 2. High power of the larvae with a short buccal cavity (red arrow) and prominent genital primordium (blue arrow), (Iodine stain, 1000x).
The bronchoscopy revealed a bloody fluid admixed with clots
which was clinically consistent with diffuse alveolar hemorrhage. The
roundworms depicted above were identified in both the BAL and stool O&P
exam. Based on the presence of the short buccal cavity and the prominent
genital primordium and the absence of eggs, the identification of Strongyloides stercoralis was made.
Given the large amount of larvae present in both the lungs and gastrointestinal
tract, the patient was diagnosed with a strongyloidiasis hyperinfection.
Discussion
Strongyloides
stercoralis is classified as a nematode (roundworm) and is the cause of strongyloidiasis
in humans. The helminth is found worldwide, especially in warm climates and
underdeveloped countries, and is the cause of 30-100 million infections. Infection
is due to fecal contamination of soil, where free-living forms are found, or
water. Infective filariform larvae penetrate intact skin, particularly bare
feet, resulting in infection. The free living cycle begins with the
rhabditiform larvae passed through the stool develops into the infective
filariform larvae or when the
rhabditiform larvae mature into free living adult male & female
forms that mate and produce eggs which then hatch and become infective filariform
larvae that can infect humans. The parasitic life cycle begins with the
infective filariform larvae penetrates human skin. The worm is then either
coughed up from the lungs and swallowed or migrates to the small intestine
where eggs are laid and hatch.
Patients may present with gastrointestinal symptoms such as
abdominal pain, bloating, and diarrhea, pulmonary symptoms like dry cough and throat
irritation, or skin rashes along points of entry (feet, ankles). When the
larvae are in the lung, Loeffler’s syndrome, characterized by pneumonia
symptoms with coughing and wheezing, may develop due to an accumulation of
eosinophils in response to the parasitic infection. In patients who are
immunocompromised, the rhabditiform larvae can develop into the filariform
larvae in the host and can directly penetrate the bowel mucosa or perianal skin
resulting in autoinfection, dissemination throughout the body, and high
parasite burden. Symptoms of hyperinfection include bloody diarrhea, bowel
perforation, destruction of lung parenchyma with bloody sputum, meningitis, and
septicemia. Hyperinfection most commonly occurs after steroid administration
for asthma or COPD exacerbation, but can also be seen in those receiving
chemotherapy or who have had organ transplants.
In the laboratory, the diagnosis of S. stercoralis is most often made by an ova and parasite exam of
the stool, duodenal fluid, sputum or BAL specimens (Image 1). Most commonly the
rhabditiform larvae are present and are identified by the presence of a short
buccal cavity and prominent genital primordium (Image 2). These two features
are helpful in distinguishing S.
stercoralis from hookworms (Ancylostoma
spp. and Necator americanus) which
have a longer buccal cavity and indistinct genital primordium. The eggs of
these two nematodes are also very similar, although typically S. stercoralis eggs hatch before they
are passed in stool specimens. S.
stercoralis can also be visualized on H&E histology sections in the
crypts of intestinal biopsies where the adult female measures up to 2.2 mm in
length. Finally, serologic testing can be helpful when there is a high
suspicion of disease in the face of multiple negative stool exams, but cannot
distinguish between a current or past infection.
Most patients do not remember a specific
exposure and prevention includes wearing gloves and shoes when handling or
walking on soil that may contain contaminated fecal material. Treatment options
for an acute or chronic S. stercoralis include
a short course of ivermectin or albendazole. In the case of disseminated infection,
ivermectin should be given until stool and sputum exams are negative for 2
weeks. In the case of our patient, she was started on ivermectin, but succumbed
to the disease due to extensive pulmonary hemorrhage.
-Jaswinder Kaur, MD, is a fourth year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
A 54 year old male with a past medical history of Type II diabetes mellitus and obesity was admitted for a few days history of severe pain over right upper quadrant accompanied by fevers, chills, nausea, vomiting and diarrhea. Physical exam revealed a palpable gallbladder. Ultrasound imaging showed a distended gallbladder with a thickened, edematous and hyperemic wall that was interpreted as acalculus cholecystitis. The patient underwent percutaneous drainage of the gallbladder with plans to undergo a cholecystectomy once the acute phase of his illness stopped. The gallbladder fluid was sent to microbiology for analysis.
Laboratory Findings
Anaerobic plates obtained from organisms growing in thioglycollate broth grew low, convex opaque white colonies. The organisms did not produce the classic double zone of beta hemolysis (Image 1). Gram stain of the culture showed gram positive bacilli that were “boxcar” shaped (Image 2). Aerobic plates had no growth. The organisms were catalase negative and non-motile. MALDI-TOF identified the organism as Clostridium perfringens.
Image 1. Growth on CNA plate in anaerobic environment Image 2. Gram stain from the anaerobic culture shows boxcar-shaped gram positive bacilli.
The patient was also placed on piperacillin-tazobactam while in the hospital. His condition improved and he was discharged home with a seven day course of cefpodoxime and metronidazole with a general surgery follow up appointment.
Discussion
Clostridium
perfringensis a gram
positive bacilli with blunt ends (boxcar shaped). These obligate anaerobes are
spore formers, however these are rarely seen. When seen, they produce
subterminal spores. These organisms cause of crepitant myonecrosis (gas
gangrene), gangrenous cholecystitis, septicemia, and food poisoning. They are present in large numbers as normal
microbiota in the gastro-intestinal tract of humans and animals, the female
genital tract and oral mucosa. Typically, infections are caused by endogenous
strains gaining access to normal sterile sites due to a predisposing factor
that compromise normal anatomy: surgery, trauma, or altered host defense
mechanisms (diabetes, burns, immunosuppression, and aspiration).
Penicillin is recommended in most infections,
however resistance has been reported. Optimal management of intra-abdominal
infection is to achieve appropriate source control and drainage is important.
Murray
P. Medical Microbiology. Seventh Edition. Elsevier; 2013.
-Angela Theiss, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.