Case History
The patient is a 3 year old male with no significant past medical history who presented to the ED with left lower extremity pain for 24 hours after falling while playing with family members. The patient’s mother was present at bedside providing the history, but was not present at the time of the fall. It is unclear how the patient injured his ankle, but family members noticed the child grabbing his ankle and suspected that he may have twisted it. After the fall, the patient was unable/unwilling to ambulate on the ankle. There is no history of fractures or cancer.
An x-ray and subsequent MRI were ordered of the ankle which demonstrated an expansile lytic lesion involving the metaphysis of the distal tibia measuring approximately 3.4 x 2.2 cm (Figure 1 and 2). The margins of this lesion are indistinct, and there is cortical irregularity at the anterior and lateral aspect of the distal metaphysis of the tibia, likely representing a pathologic fracture. The differential diagnosis includes infection, aneurysmal bone cyst, nonossifying fibroma, osteoblastoma and histiocytosis.
The patient and family then followed up with Orthopedics, who proceeded to perform a biopsy of the lytic lesion in order to determine the nature of the lesion. The results are below.


Diagnosis
Received fresh for intraoperative consultation is a 1.1 x 0.6 x 0.5 cm aggregate of white-tan soft tissue fragments. Half of the tissue fragments are frozen and read out as “spindle cell proliferation. Consideration of low-grade vasoformative lesion. Defer to permanent,” with 3 pathologists consulting on the diagnosis. The remainder of the tissue not submitted for frozen section, as well as the entirety of a second container from the same lesion, is submitted for routine processing.
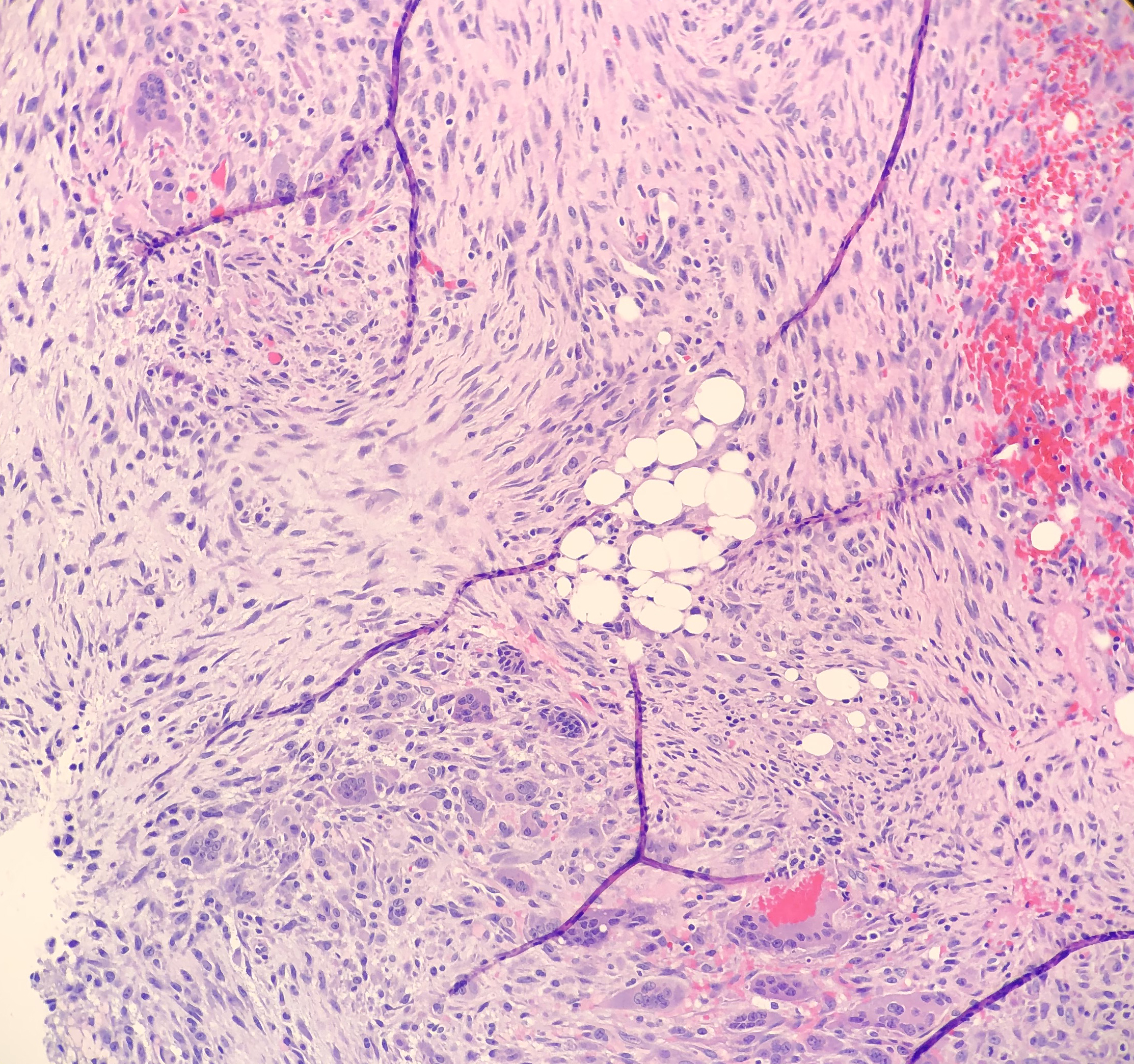
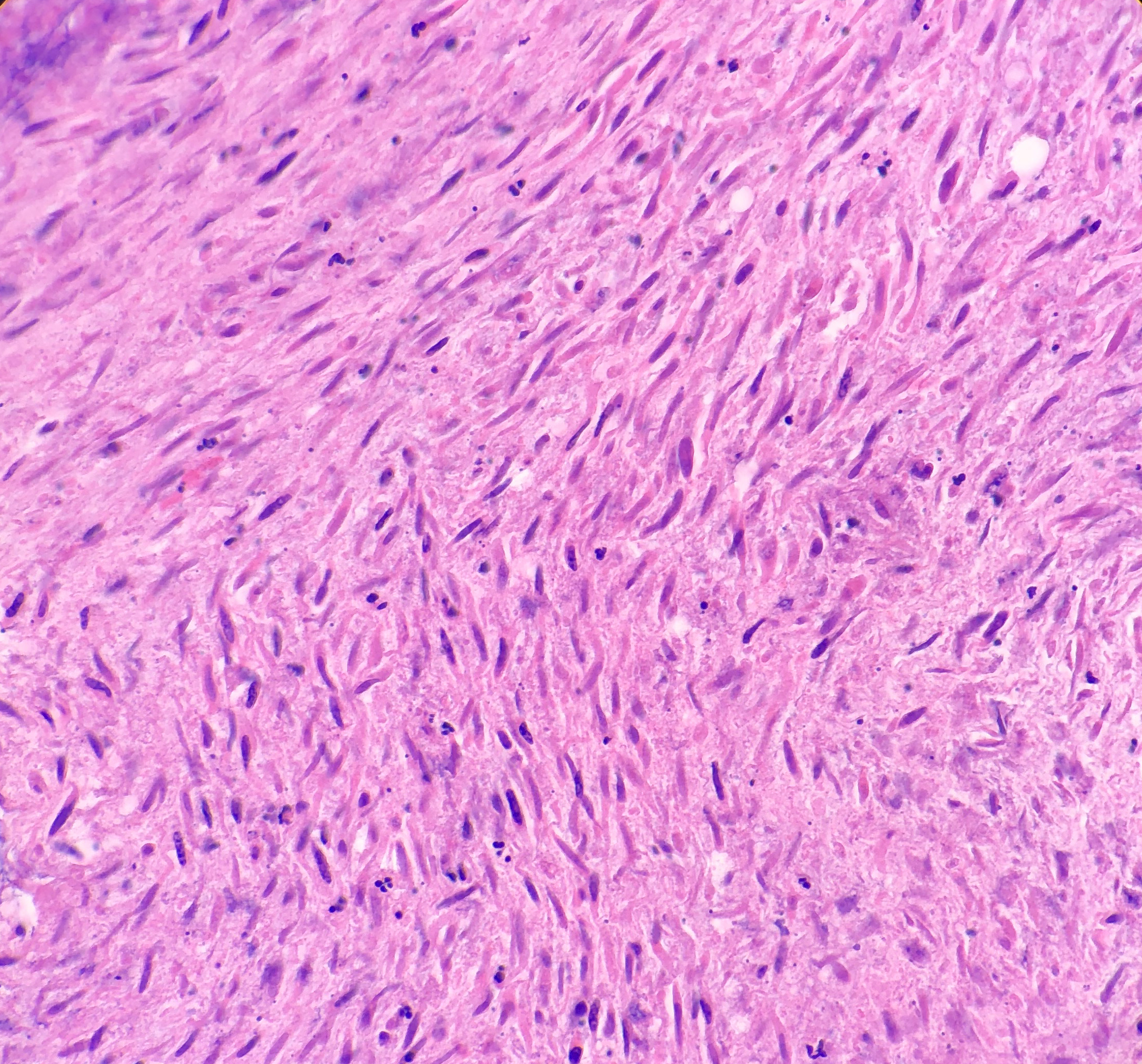
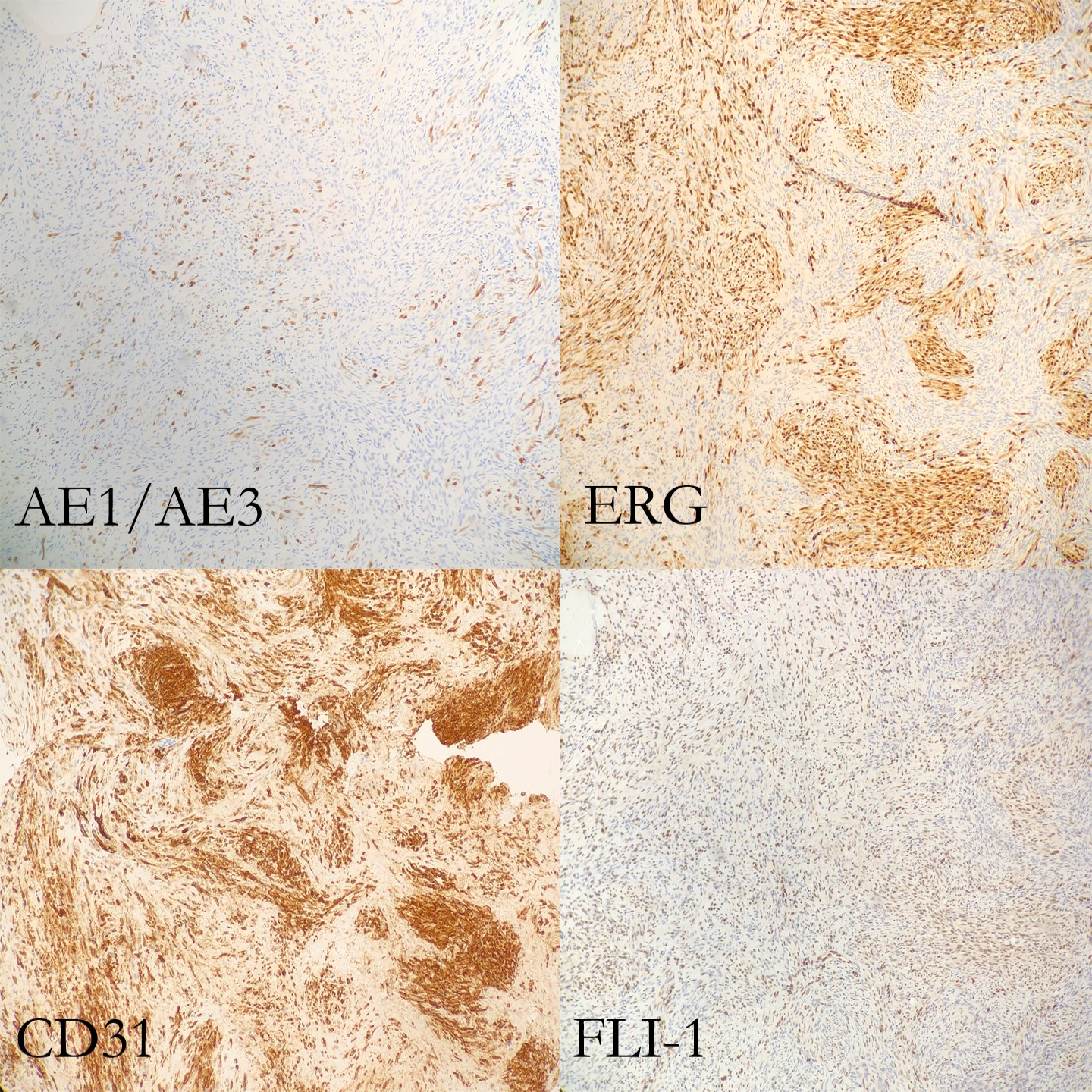
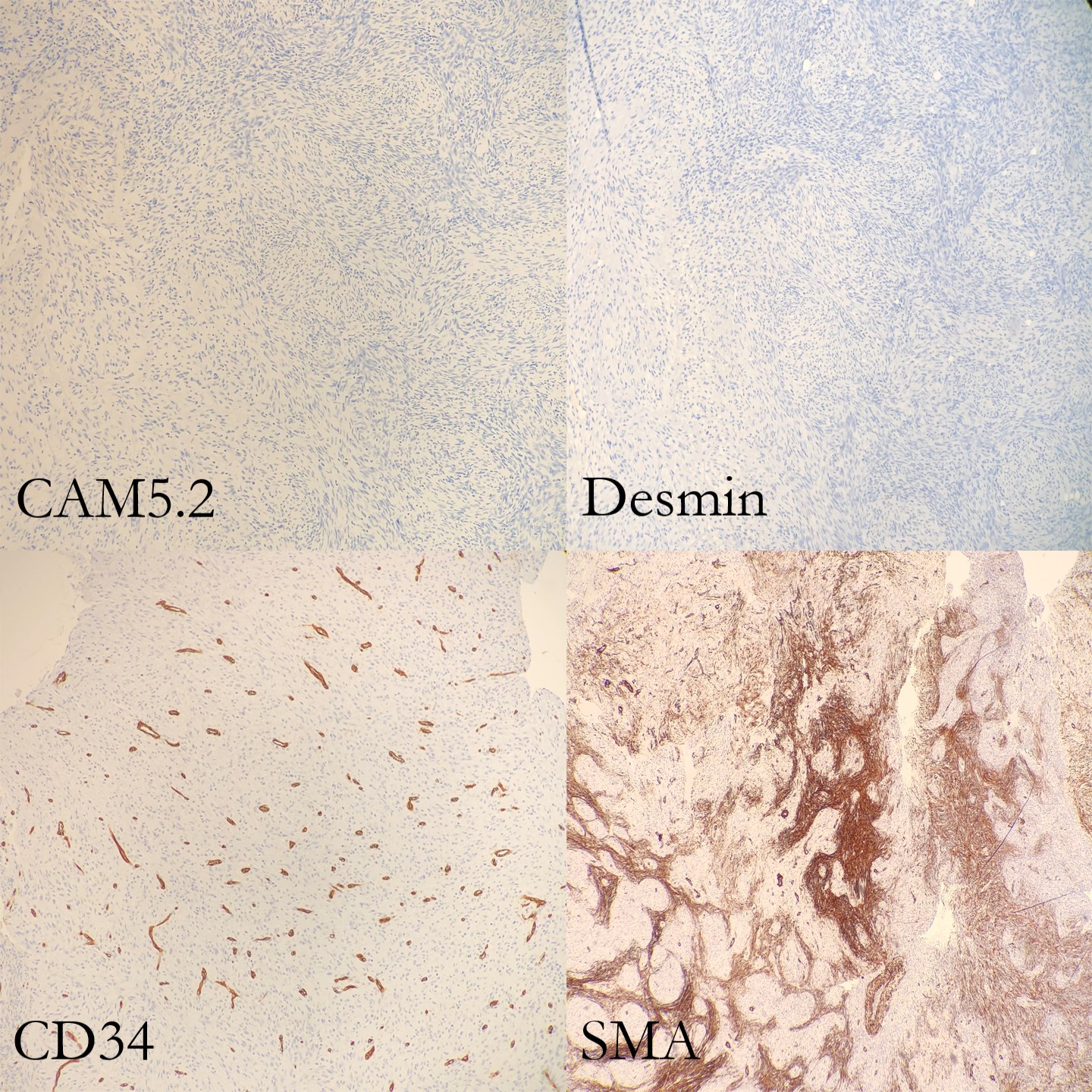
On microscopy, the biopsies demonstrate a moderately cellular proliferation of fasciculated spindle cells in a collagenous to myxoid stroma. Nuclei are predominantly oval with variably fine to granular chromatin. Many cells have moderate amounts of tapering eosinophilic cytoplasm, resembling strap cells. Inflammatory cells and osteoclast-like giant cells are admixed (Figure 3 and 4). Immunohistochemical stains demonstrate lesional spindle cells to be positive for CD31, ERG, and FLI1. AE1/AE3 and CAM5.2 highlight rare lesional spindle cells. SMA stains some stellate spindle cells, favored to represent associated myofibroblasts. Desmin, MDM2, CDK4, ALK, and S100 are negative in plump lesional cells (Figure 5 and 6). Overall, the features are consistent with pseudomyogenic hemangioendothelioma, a rare vascular tumor. Although more commonly present in soft tissue, primary bone cases have been reported. These neoplasms have some risk for local recurrence, but only rarely distant metastasis. A portion of tissue was sent to the University of Nebraska Medical Center to evaluate for a characteristic gene rearrangement (SERPINE1-FOSB) that is present in at least a subset of pseudomyogenic hemangioendotheliomas. This was negative.
The lesion was then curettaged by the surgical team.The patient and his family had two follow up office visits with the Orthopedics department. The first one, a week after surgery, was unremarkable. The second visit, two weeks after surgery, was notable for the patient developing a cutaneous rash on both arms and chest. Due to literature citing that these tumors generally arise in the soft tissue, the clinician suggested that the patient and family follow up with pediatric dermatology to ensure that this new rash is not related to the pseudomyogenic hemangioendothelioma. Unfortunately due to insurance, the patient and family had to see a dermatologist at a different institution, and no further visits have taken place.
Discussion
Pseudomyogenic hemangioendothelioma (PHE) is a rare vascular tumor that most commonly arises in the skin and soft tissues of the extremities. It is usually multifocal, appearing in multiple tissue planes, such as the mucosa, dermis, subcutis and skeletal muscle, in a variety of different anatomic sites. Although even less common, PHE can also involve bone (such as this case). PHE has a male predilection, typically appearing in the second to fourth decades of life. Of the most common symptoms that the patient presents with, pain appears to top the list, although it should be stated that only about half of the patients experience pain.
Grossly, skin and soft tissue PHE tumors appear firm, ill-defined and gray-white. When they involve bone, they appear as multiple discrete, pink-tan to dark brown hemorrhagic tumors with surrounding sclerosis, ranging from 0.1 to 6.5 cm in greatest dimension.
Histologically, PHE demonstrates plump spindle and rhabdomyoblast-like cells with densely eosinophilic cytoplasm that grows in sheets and fascicles. The cells can be mistaken as rhabdomyoblasts because of the eosinophilic cytoplasm that pushes the nucleus to the periphery of the cell. Immunohistochemical studies are very helpful in order to determine a diagnosis of PHE. AE1/AE3, ERG, FLI-1 and CD31 are positive, whereas CD34, desmin and S100 are negative. Karyotyping has revealed a fusion of genes SERPINE1-FOSB that corresponds to the recurrent translocation t(7;19)(q22;q13). In this case, the SERPINE1-FOSBgene rearrangement was negative, but could possibly be due to a variant fusion gene.
Making a histologic diagnosis can be difficult for a Pathologist, due to the wide variety of differential diagnoses that will need to be excluded first.
The differential diagnosis for a cutaneous tumor includes:
- Cellular benign fibrous histiocytoma (lacks rhabdomyoblast-like cells and neutrophilic infiltrates, contains mitotic figures, and is negative for cytokeratin and CD31)
- Spindle cell squamous cell carcinoma (usually in sun-damaged skin, with nuclear atypia and negative endothelial markers)
- Epithelioid sarcoma (negative INI1, positive EMA and CD34, and a nodular architecture with central necrosis and more nuclear atypia)
The differential diagnosis for soft tissue tumors include:
- Epithelioid sarcoma (see above)
- Epithelioid hemangioendothelioma (usually intracytoplasmic vacuoles, positive CD34 and CAMTA1, and a t(1;3)(p36.3;q25) translocation resulting in WWTR1-CAMTA1 gene fusion)
- Epithelioid angiosarcoma (vasoformative architecture with sheet-like pattern, nuclear atypia, high nuclear grade, frequent mitosis and irregular vascular channels)
The differential diagnosis for bone tumors includes:
- Epithelioid hemangioma (lacks rhabdomyoblast-like cells)
- Giant cell tumor (lacks rhabdomyoblast-like cells and fascicles of spindle cells)
- Osteoblastoma (lacks rhabdomyoblast-like cells and fascicles of spindle cells)
In a study by Inyang et al, when PHE involved bone, imaging would demonstrate multiple to innumerable discontinuous tumors throughout the affected bone, involving the cortex and/or medullary cavity of the epiphysis, metaphysis, or diaphysis. On x-ray and computed tomography, the lesions appeared as well circumscribed, lobulated and lytic, with a sclerotic rim on some of the lesions. On magnetic resonance imaging, T1-weighted images would appear dark, and T2-weighted images would appear hyperintense.
PHE has a tendency to recur locally, but rarely develops distant metastases. Since PHE presents as a multifocal disease and can be easily confused for a distant metastasis, care needs to be taken to ensure that a diagnosis of PHE is not overlooked.
Surgical ablation and excision is the standard treatment for a patient with PHE, with a few cases noted of patients being treated with radiotherapy and/or adjuvant chemotherapy, in addition to surgery. Everolimus and sirolimus have recently been found to be effective in cases of patient with PHE that had metastatic and relapsing multifocal PHE.
References
- Hornick JL, Fletcher CDM. “Pseudomyogenic Hemangioendothelioma: A Distinctive, Often Multicentric Tumor With Indolent Behavior.” Am J Surg Pathol. 2011; 35: 190201.
- Inyang A, et al. “Primary Pseudomyogenic Hemangioendothelioma of Bone.” Am J Surg Pathol. 2016; 40: 587598.
- Pradhan D. “Pseudomyogenic hemangioendothelioma of skin, bone and soft tissue; a clinicopathological, immunohistochemical, and fluorescence in situ hybridization study.” Hum Pathol. 2018; 71: 126134.
- Sugita S, Hirano H, Kikuchi N, et al. Diagnostic utility of FOSB immunohistochemistry in pseudomyogenic hemangioendothelioma and its histological mimics. Diagn Pathol. 2016;11(1):75. Published 2016 Aug 11. doi:10.1186/s13000-016-0530-2

-Cory Nash is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology. He currently works as a Pathologists’ Assistant at the University of Chicago Medical Center. His job involves the macroscopic examination, dissection and tissue submission of surgical specimens, ranging from biopsies to multi-organ resections. Cory has a special interest in head and neck pathology, as well as bone and soft tissue pathology. Cory can be followed on twitter at @iplaywithorgans.
